Updated August 2014
Guide to American Medical Association (AMA) Manual of Style, 10
th
Edition
Purposes of references: documentation, acknowledgement, & directing/linking the reader to more information
ALL authors are responsible for ALL reference citations
Always consult primary source and never cite a reference you yourself have not read
Whatever reference style is used (e.g. AMA, NLM), consistency is imperative
Each reference is separated into bibliographic groups by a period. Within each group, commas, semi-colons, or colons are used.
Authors: Use authors’ surname followed by their initials without periods. If there are < 6 authors, all should be named. If there
are > 6 authors, list the first 3 followed by “et al.” Roman numerals and “Jr/Sr” follow the initials. Original spelling and
capitalization of surnames with prefixes or particles (e.g. von, de, La, van) are retained.
Titles: Retain the spelling, abbreviations, style (e.g. capitalization) of the original title (including numbers). Exception: numbers
at the beginning of the title should be spelled out (except specific years (e.g. 1948).
Journal: Use NLM-abbreviated titles (e.g. N Engl J Med). Search titles here: http://www.ncbi.nlm.nih.gov/nlmcatalog/journals.
Information about abbreviated titles: http://www.nlm.nih.gov/pubs/factsheets/constructitle.html.
Citation Type
Format
Example
Journal article
(print)
Author(s). Title. Journal. Year;Volume(Issue):Page
number(s).
Rainer S, Thomas D, Tokarz D, et al. Myofibrillogenesis
regulator 1 gene mutations cause paroxysmal dystonic
choreoathetosis. Arch Neurol. 2004;61(7):1025-1029.
Journal article
(online)
1. With URL
2. With DOI
3. Published
ahead of
print
Author(s). Title. Journal. Year;Volume(Issue):Page
number(s). URL. Published date. Updated date.
Accessed date.
Author(s). Title. Journal. Year;Volume(Issue):Page
number(s). DOI.
Author(s). Title [published online ahead of print
date]. Journal. Year;Volume(Issue):Page number(s).
DOI.
Duchin JS. Can preparedness for biological terrorism save
us from pertussis? Arch Pediatr Adolesc Med.
2004;158(2):106-107. http://archpedi.ama-
assn.org/cgi/content/full/158/2/106. Accessed June 1,
2004.
Smeeth L, Iliffe S. Community screening for visual
impairment in the elderly. Cochrane Database Syst Rev.
2002;(2):CD001054. doi:10.1002/14651858.CD1001054.
van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of
a new human coronavirus [published ahead of print
March 21, 2004]. Nat Med. doi:10.1038.nm1024.
Book chapter
(print)
Chapter author(s). Chapter title. In: Book author(s)
or editor(s). Book title. Volume number and title.
Edition number (do not indicate 1
st
edition). Place
of publication: Publisher; Year:Page number(s).
Solensky R. Drug allergy: desensitization and treatment
of reactions to antibiotics and aspirin. In: Lockey P, ed.
Allergens and Allergen Immunotherapy. 3
rd
ed. New York,
NY: Marcel Dekker; 2004:585-606.
Book chapter
(online)
Chapter author(s). Chapter title. In: Book author(s)
or editor(s). Book title. Volume number and title.
Edition number (do not indicate 1
st
edition). Place
of publication: Publisher; Year:Page number(s).
URL. Accessed date.
Resnik NM. Geriatric medicine. In: Braunwald E, Fauci AS,
Isselbacher KJ, et al, eds. Harrison’s Online. Based on:
Braunwald E, Hauser SL, Fauci AS, Kasper DL, Longo DL,
Jameson JL, eds. Harrison’s Principles of Internal
Medicine. 15
th
ed. New York, NY: McGraw-Hill; 2001.
http://www.hsls.pitt.edu/resources.documentation/harri
soninfo.html. Accessed December 6, 2005.
Book (print)
Book author(s) or editor(s). Book title. Volume
number and title. Edition number (do not indicate
1
st
edition). Place of publication: Publisher; Year.
Adkinson N, Yunginger J, Busse W, Bochner B, Holgate S,
Middleton E, eds. Middleton’s Allergy: Principles and
Practice. 6
th
ed. St Louis, MO: Mosby; 2003.
General Notes about References (p40-41)
1
Formatting Citations (p39-71)
1-3
Updated August 2014
Book (online)
Book author(s) or editor(s). Book title. Volume
number and title. Edition number (do not indicate
1
st
edition). Place of publication: Publisher; Year.
URL. Accessed date.
Lunney JR, Foley KM, Smith TJ, Gelband H, eds.
Describing Death in America: What We Need to Know.
Washington, DC: National Cancer Policy Board, Institute
of Medicine; 2003.
http://www.nap.edu/books/0309087252/html/.
Accessed December 6, 2005.
Website
Author(s). Title of item cited. Name of Web site.
URL. Published date. Updated date. Accessed date.
Antimicrobial Resistance. Infectious Diseases Society of
America.
http://www.idsociety.org/Topic_Antimicrobial_Resistanc
e/. Accessed July 21, 2014.
Drug Information
Database
Author(s). Title of entry. In: Title of database
[database online]. Place of publication: Publisher;
Year. URL. Updated date. Accessed date.
Acetaminophen poisoning. In: DynaMed [database
online]. EBSCO Information Services. http://0-
search.ebscohost.com.topcat.switchinc.org/login.aspx?di
rect=true&site=DynaMed&id=113862. Updated March
09, 2010. Accessed March 23, 2010.
Monograph
Author(s). Monograph. In: Title of database
[database online]. Place of publication: Publisher;
Year. URL. Updated date. Accessed date.
Minoxidil. In: Lexicomp, Lexi-Drugs [database online]. St.
Louis, MO: Wolters Kluwer Health, Inc; 2005. http://0-
online.lexi.com.topcat.switchinc.org/lco/action/doc/rere
trie/docid/patch_f/1799123. Updated July 8, 2014.
Accessed July 24, 2014.
Government/
Organization
Reports
Author(s). Title. Place of publication: Name of
issuing organization; Year. Page(s)/ publication/
series numbers.
Centers for Disease Control and Prevention. Sexually
Transmitted Disease Surveillance, 2000. Atlanta, GA:
Centers for Disease Control and Prevention, US Dept of
Health and Human Services; 2000.
Government/
Organization
Reports (online)
Author(s). Title. Place of publication: Name of
issuing organization; Year. Page(s)/ publication/
series numbers. URL. Published date. Updated date.
Accessed date.
World Health Organization. Equitable access to essential
medicines: a framework for collective action.
http://whqlibdoc.who.int/hq/2004/WHO_EDM_2004.4.p
df. Published March 2004. Accessed December 6, 2005.
Package inserts
Drug. [package insert]. Place of manufacturing:
Manufacturer; Year.
Cialis [package insert]. Indianapolis, IN: Eli Lilly & Co;
2003.
Patents
Inventor(s), inventors; Company, assignee. Title.
Patent number. Patent date.
Guiliano K, Kapur R, inventors; Cellomics Inc, assignee.
System for cell-based screening. US patent 6,875,578.
March 15, 2005.
Unpublished
Material (accepted
for publication)
Author(s). Title. Journal. In press.
Carrau RL, Khidr A, Crawley JA, Hillson EM, Davis JK,
Pashos CL. The impact of laryngopharyngeal reflux on
patient-reported quality of life. Laryngoscope. In press.
Unpublished
Material (submitted
for publication)
In-text only (author(s), unpublished data, date)
Do not include in reference list
(H. E. Marman, MD, unpublished data, January 2005)
Conference
Presentations
Author(s). Title. Poster/Paper presented at:
Meeting name; Date(s); Location.
Weber KJ, Lee J, Decresce R, Subjasis M, Prinz R.
Intraoperative PTH monitoring in parathyroid hyperplasia
requires stricter criteria for success. Paper presented at:
25
th
Annual American Association of Endocrine Surgeons
Meeting; April 6, 2004; Charlottesville, VA.
Conference
Presentations
(online)
Author(s). Title. Poster/Paper presented at:
Meeting name; Date(s); Location. URL. Accessed
date.
Chu H, Rosenthal M. Search engines for the World Wide
Web: a comparative study and evaluation methodology.
Paper presented at: American Society for Information
Science Annual Conference; October 19-24, 1996;
Baltimore, MD. http://www.asis.org/annual-
96/electronicproceedings/chu.html. Accessed February
26, 2004.
Updated August 2014
List references in numerical order (i.e. consecutively as they appear in the document/presentation; NOT alphabetical order)
During the draft phase of your document, it is often easiest to use parenthetical citations with the author’s last name as place-holders
until the document/presentation is complete; then put the citations in numerical order on the final version
DRAFT FINAL
Number references consecutively with superscript Arabic
numerals, including text, tables, or figures
For 2 or more references cited at a given place:
Use hyphens to join the first and last numbers of a
closed series
Use commas without a space to separate other parts
of a multiple citation
If a multiple citation involves many references and
creates the appearance of a hole (usually 20-25
characters or more), use an asterisk in the text and
give the citation in a footnote
Place superscript numerals outside periods and commas,
inside colons and semicolons
Do NOT place a superscript reference immediately after a
number or abbreviated unit of measure
You may cite page numbers within superscript reference
Be sure to cite often enough throughout the
document/presentation so that the reader can know where
you got the information, but be careful not to cite too often
(i.e. do not only include your list of references and not cite
throughout; if several consecutive sentences are from the
same reference, you may only cite the first sentence)
Reference List (p41-42)
1,4
1. Hall JE, Brands MW. Intrarenal and circulating angiotensin II and renal function. In: Robertson
JIS, Nicholls MG, eds. The Renin-Angiotensin System. London: Gower Medical, 1993.
2. Weber KT, Brilla CG. Pathological hypertrophy and cardiac interstitium: fibrosis and renin-
angiotensin-aldosterone system. Circulation. 1991;83:1849-1865.
3. Weber KT, Villarreal D. Aldosterone and antialdosterone therapy in congestive heart failure.
Am J Cardiol. 1993;71:3A-11A
4. Barr CS, Lang CC, Hanson J, Arnott M, Kennedy N, Struthers AD. Effects of adding
spironolactone to an angiotensin-converting enzyme inhibitor in chronic congestive heart
failure secondary to coronary artery disease. Am J Cardiol. 1995;76:1259-1265.
5. Staessen J, Lijnen P, Fagard R, Verschueren LJ, Amery A. Rise in plasma concentration of
aldosterone during long-term angiotensin II suppression. J Endocrinol. 1981;91:457-465.
Aldosterone is known to be important in the pathophysiology
of heart failure.(Hall; Weber (1991); Weber (1993); Barr) Many
clinicians have assumed that angiotensin-converting enzyme
(ACE) inhibitors, by inhibiting the conversion of angiotensin I to
angiotensin II, inhibit the production of aldosterone. Increasing
evidence, however, suggests that currently recommended and
usual doses of ACE inhibitors do not completely suppress
aldosterone production.(Staessen)
Aldosterone is known to be important in the pathophysiology
of heart failure.
1-4
Many clinicians have assumed that
angiotensin-converting enzyme (ACE) inhibitors, by inhibiting
the conversion of angiotensin I to angiotensin II, inhibit the
production of aldosterone. Increasing evidence, however,
suggests that currently recommended and usual doses of ACE
inhibitors do not completely suppress aldosterone production.
5
Numbering (p42-44)
1,4
Aldosterone is known to be important in the pathophysiology
of heart failure.
1-4
Many clinicians have assumed that
angiotensin-converting enzyme (ACE) inhibitors, by inhibiting
the conversion of angiotensin I to angiotensin II, inhibit the
production of aldosterone. Increasing evidence, however,
suggests that currently recommended and usual doses of ACE
inhibitors do not completely suppress aldosterone production.
5
Citation
1-4
Citation
1-2,4
Citation
1,3,5-7,10-13,15,18,19,21
Citation*
Citation.
1,2
Citation,
1,2
Citation
1,2
:
Citation
1,2
;
Table 1
3
; 50 m
2
Citation
2(p67),3
Updated August 2014
Citations for references not yet accepted for publication or personal communications (oral, written, and electronic) should NOT be
included in the reference list, but should be included parenthetically in the text
Other in-text citations for references that should be included in a reference list are not common in most professional documents
(except presentations, see below) and should be reserved for circumstances where reference lists are not used (e.g. news articles)
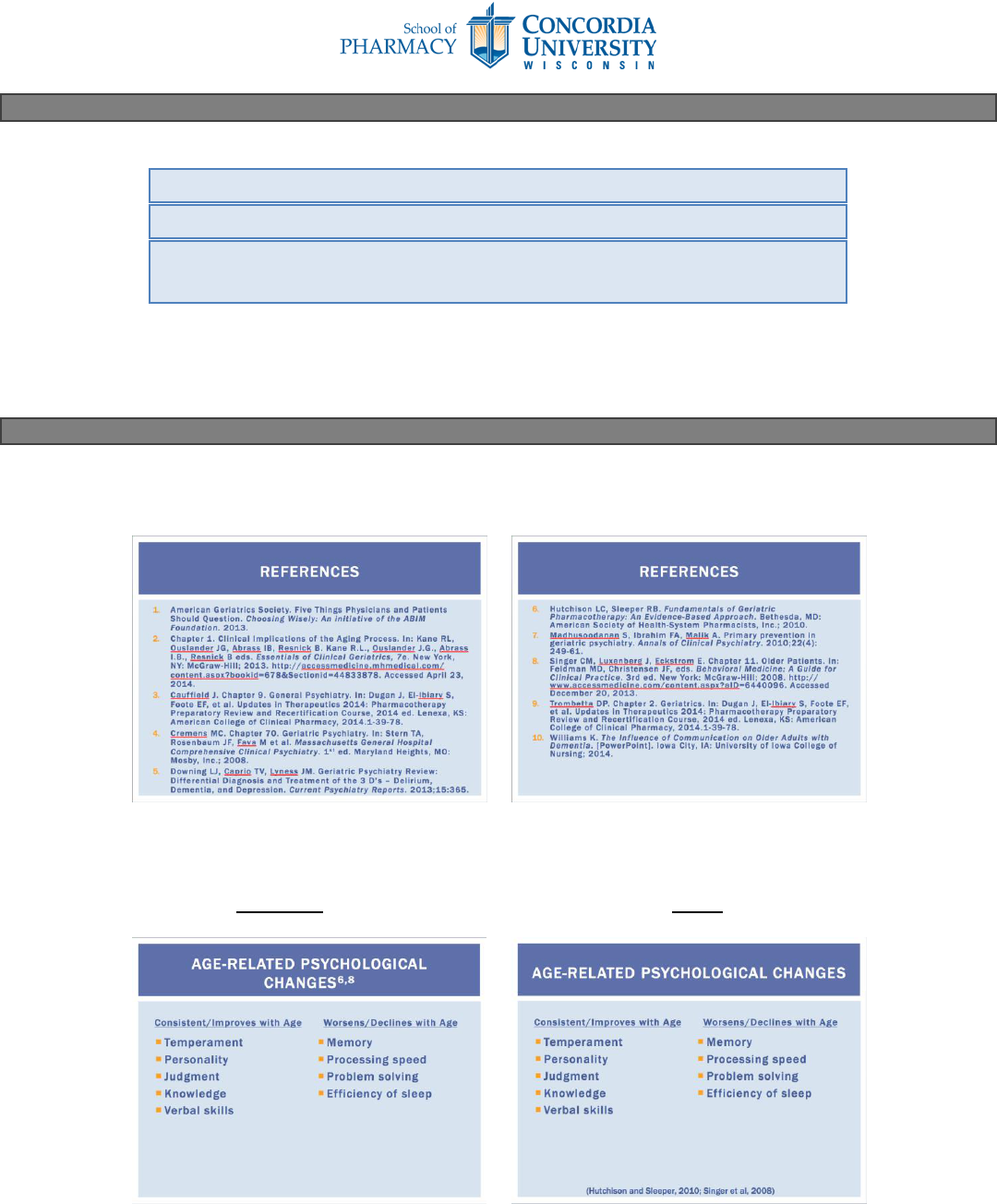
AMA does not provide official guidance on PowerPoint presentations. However, just like any other piece of work, it is important to
give credit to your sources.
At a minimum, all presentations should include a reference slide at the end AMA formated citations (may or may not be numbered).
(Kostrzewa, Geriatric Psychiatry, April 2014, Concordia University Wisconsin, School of Pharmacy)
Ideally, you should also cite individual slides. There are several ways to do this. Make sure to ask your instructor what they prefer
before formatting your citations. Two possible examples are given here:
Superscript In-text
(in numerical order; much correspond with reference list) (Bottom of slide; in parentheses; may be smaller font)
Book: (Author*, Year, Page(s))
*Surname only; if 2, list both; if > 2, list first + “et al”
Journal: (Journal [abbreviated]. Year;Volume(Issue):Page(s))
In-Text Citations (p41)
1
As described in recent literature (H. E. Marman, MD, unpublished data, January 2005)…
In a conversation with Dr. Smith (October 2009)…
According to Dr. Kostrzewa (Introduction to Tertiary References lecture, September
2013, Concordia University Wisconsin, School of Pharmacy)…
PowerPoint Presentations
1,5
Updated August 2014
Follow AMA rules above. Typically, there is a reference section in the bottom left or right corner of the poster and the font size is
often smaller than the rest of the poster text.
1. Iverson C. References. In: Iverson C et al. AMA Manual of Style: A Guide for Authors and Editors. 10
th
ed. New York, NY: Oxford University Press, Inc.;
2007:39-79.
2. NLM Catalog: Journals referenced in the NCBI Databases. National Center for Biotechnology Information, U.S. National Library of Medicine.
http://www.ncbi.nlm.nih.gov/nlmcatalog/journals. Accessed July 25, 2014.
3. Fact Sheet: Construction of the National Library of Medicine Title Abbreviations. National Institutes of Health, U.S. National Library of Medicine.
http://www.nlm.nih.gov/pubs/factsheets/constructitle.html. Published May 23, 2007. Updated March 10, 2014. Accessed July 25, 2014.
4. Pitt B, Pierard LA, Bilge A, et al. Effectiveness of Spironolactone Added to an Angiotgensin-Converting Enzyme Inhibitor and a Loop Diuretic for Severe
Chronic Congestive Heart Failure (The Randomized Aldactone Evaluation Study [RALES]). Am J Cardiol. 1996;78:902-907.
5. Kostrzewa A, Smith E, Daniels A, Antonopoulos J, Karczewski C, Kotz K. Optimizing Medication Reconciliation Communication between Hospital and
Nursing Home Upon Discharge. Poster presented at: University HealthSystem Consortium Conference; December 2012; Las Vegas, NV.
6. Valdovinos K, Kostrzewa A, Harrison L, Paly E. Effect of an inter-professional project on pharmacy and physical therapy student’s readiness for inter-
professional learning. Poster presented at: AACP Annual Meeting; July 26-30, 2014. Grapevine, TX.
Professional Posters
1,5,6
References
If you have any questions about referencing or the AMA format, please contact your course coordinator or
Audrey Kostrzewa, PharmD, MPH at audrey.kostr[email protected] or 262-243-2750
Superscript
citation
Reference
list
