Disabled Facilities
Grant (DFG) and
Other Adaptations
– External Review
Dec
2018
Main Report
Sheila Mackintosh, Paul Smith, Helen Garrett, Maggie Davidson, Gareth Morgan, and Rachel Russell

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Acknowledgements
From the beginning we realised this was a rare opportunity to refresh and revitalise a
programme that helps thousands of people every year but has become overly
complicated through a changing health and care environment and nearly 30 years of
custom and practice. With only three months to complete the field work we are very
appreciative of all the contributions received.
Thank you to everyone who contributed to this review. Around 200 people came to the
initial free consultation workshops to consider, debate and vote on a range of options
that set the direction and tone of the narrative, supported by Foundations’ commercial
partners. Hundreds more watched the online videos and gave detailed feedback on
the options. A number of organisations also submitted more detailed written responses
that helped to further shape our recommendations. The passion and dedication with
which people expressed their views was remarkable.
We also spoke to a range of experts from within the sector and beyond whose
knowledge and varying perspectives either challenged our preconceptions or
reinforced our thinking – but in either case strengthened our recommendations.
Particular thanks also go to the members of the DFG Champions Facebook group who
provided instant opinions, case studies and data when we needed it.
A number of home improvement agencies and local authorities had previously
participated in ‘Rethinking DFG’ workshops with Foundations and the Social Change
Agency that strongly influenced our thinking on assessment and the upper limit.
We would like to acknowledge the support of both the Department of Health and Social
Care and the Ministry of Housing, Communities and Local Government in developing
this review.
Finally, we would like to thank all our colleagues who provided support and
encouragement while we were busy writing up the findings. We would also like to thank
Anna Bornioli of the Centre for Public Health and Wellbeing who did the final edit of
the report.
We set out to #fixtheDFG and make it fit for purpose for the next 30 years and beyond.
We think our recommendations will go a long way to achieving that aim.
First published December 2018
University of the West of England
Centre for Public Health and Wellbeing
Faculty of Health and Applied Sciences
Frenchay Campus, Coldharbour Lane
Bristol BS16 1QY
ISBN 9781860435522
2

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Contents
Acknowledgements.................................................................................................. 2
Glossary.................................................................................................................. 10
Chapter 1. Introduction.......................................................................................... 11
The aims of this review ......................................................................................... 11
Why the review is needed..................................................................................... 12
Changes since the last review .......................................................................... 12
Changing context.................................................................................................. 13
Integration ......................................................................................................... 13
Increased resources.......................................................................................... 14
Ageing population and rising numbers of disabled people ................................ 14
Changing expectations and impact of technology ............................................. 14
Changes in tenure............................................................................................. 14
Problems with service delivery ............................................................................. 15
The focus of the report.......................................................................................... 15
Chapter 2. Methodology ........................................................................................ 17
The review ............................................................................................................ 17
Methodology ......................................................................................................... 17
Part A How the DFG is used currently................................................................. 20
Chapter 3. DFG funding ......................................................................................... 21
Funding sources and trends ................................................................................. 21
Reasons behind the trends................................................................................... 23
The need to increase the number of grants .......................................................... 26
Summary - funding issues .................................................................................... 26
Chapter 4. Who receives the grant ....................................................................... 27
Age of DFG recipients .......................................................................................... 27
Tenure of DFG recipients ..................................................................................... 29
Home owners.................................................................................................... 29
Registered providers ......................................................................................... 30
Private rented sector tenants ............................................................................ 31
Council stock..................................................................................................... 34
Rural housing ....................................................................................................... 34
Who is excluded from the DFG?........................................................................... 35
3

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Reasons for exclusion .......................................................................................... 39
Summary - who gets the DFG and who is excluded ............................................. 41
Chapter 5. Types of adaptations and costs ......................................................... 43
Types of impairment ............................................................................................. 43
Impairment of DFG recipients............................................................................... 44
Type of work allowed ............................................................................................ 45
Type of work carried out ....................................................................................... 46
The cost of DFG work........................................................................................... 47
More expensive grants and those over the upper limit of £30,000 ....................... 49
Rehousing as an alternative to expensive grants ................................................. 50
The Means Test.................................................................................................... 51
Land Charges ....................................................................................................... 52
Summary - types of adaptations and costs........................................................... 52
Chapter 6. Costs and benefits to local authorities.............................................. 54
The benefits of adaptations and potential cost savings ........................................ 54
Costs savings of adaptations for children and young people ............................ 57
DFG outcome data............................................................................................ 58
The revenue costs of delivering the DFG ............................................................. 59
Independent HIAs ............................................................................................. 60
Staff costs by type of work ................................................................................ 61
Summary - costs and benefits to local authorities ................................................ 63
Chapter 7. Processing arrangements and waiting times.................................... 64
Processing arrangements..................................................................................... 64
Time taken to process grants ............................................................................... 68
The effect of RRO policies on timescales ......................................................... 68
The effect of shortages of contractors on timescales ........................................ 69
Effect on disabled and older people, their families and carers.............................. 70
The suitability of the six-month time limit........................................................... 71
The impact of delays ......................................................................................... 72
Summary of issues - processing arrangements and waiting times ....................... 72
Part B How the DFG should change.................................................................... 74
Chapter 8. Introduction to Part B.......................................................................... 75
The structure of Part B ...................................................................................... 76
Chapter 9. The bigger picture ............................................................................... 77
The Disabled Facilities Grant - a hidden service .................................................. 77
4

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
DFG and the Better Care Fund (BCF) .................................................................. 78
Strategic oversight ................................................................................................ 80
The options for strategic oversight........................................................................ 81
Making partnerships work..................................................................................... 84
National level oversight......................................................................................... 86
Cultural change..................................................................................................... 86
Recognising the broader role of the DFG ............................................................. 87
The need for person-centred services .................................................................. 87
Providing more choice by engaging with housing providers ................................. 88
What should the grant be called? ......................................................................... 89
Recommendations - strategic oversight................................................................ 90
Chapter 10. Local delivery..................................................................................... 91
The need for integrated teams.............................................................................. 91
How an integrated team works ............................................................................. 92
Key elements of integrated services ..................................................................... 98
National transformation fund................................................................................. 99
Recommendations – local delivery ..................................................................... 100
Chapter 11. Working better together .................................................................. 101
Establishing local need and handling referrals ................................................... 101
Finding people needing help with their homes ................................................ 101
Information, advice and routing people down the right pathways.................... 104
Effective working................................................................................................. 105
Deciding what is complex and needs occupational therapy input ................... 105
Improving the model for assessing what adaptations are necessary, appropriate,
reasonable and practicable ............................................................................. 107
A collaborative model for the process of determining necessary and appropriate,
reasonable and practicable ............................................................................. 109
Developing a standardised design and construction process for housing
adaptations ..................................................................................................... 111
Communicating with customers, carers and their families .............................. 112
Working in partnership with contractors .......................................................... 113
Delivering better health and social care outcomes ............................................. 114
Examples of preventative services providing savings to health and care........ 114
Dementia and the DFG ................................................................................... 116
Making every contact count (MECC)............................................................... 118
Data collection and reporting .............................................................................. 119
5

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Local reporting ................................................................................................ 119
National reporting............................................................................................ 122
Recommendations – working better together ..................................................... 123
Chapter 12. The allocation of resources ............................................................ 124
Current allocations methodology and the need for review .................................. 124
Our approach to the review of resource allocation.............................................. 126
1. The baseline................................................................................................ 128
2. Adjusting this ‘baseline need’ using factors................................................. 132
3. ‘Frail elderly factor’ ...................................................................................... 137
4. The new baseline and impact of adding each factor ................................... 139
Building costs/cost of adaptations................................................................... 149
Summary points – allocation of resources .......................................................... 150
Recommendations - allocation of resources....................................................... 152
Chapter 13. Other funding issues....................................................................... 153
Local contributions to DFG funding..................................................................... 153
Risk sharing contingency fund............................................................................ 154
Joint decision-making and combined funding ..................................................... 155
Personal health budgets ..................................................................................... 156
Recommendations – other funding issues.......................................................... 157
Chapter 14 The means test.................................................................................. 158
Means testing in practice .................................................................................... 159
The options......................................................................................................... 160
Remove the Means test Completely ............................................................... 160
Use of Passporting Only ................................................................................. 162
Update the Existing Means test....................................................................... 163
Adopt the Care and Support Charging Regulations (CSCR)........................... 170
Example scenarios.......................................................................................... 173
Choosing a preferred option ............................................................................... 176
Recommendations – the means test .................................................................. 177
Chapter 15. Regulation and the upper limit ....................................................... 178
The legislation .................................................................................................... 178
The upper limit.................................................................................................... 180
Options for change.......................................................................................... 181
The evidence for change................................................................................. 182
Move away from one size fits all delivery ........................................................ 186
6

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Setting a maximum amount ............................................................................ 186
Joint funding, risk sharing and joint decision-making ...................................... 188
Moving rather than adapting ........................................................................... 189
Summary about the upper limit ....................................................................... 190
Regulatory Reform Order (RRO) ........................................................................ 190
Suitability of the 6-month time limit ..................................................................... 194
Other regulation.................................................................................................. 194
The Services and Charges Order.................................................................... 194
Other Funding Considerations ........................................................................ 195
Need for clearer guidance............................................................................... 196
Recommendations – regulation and the upper limit............................................ 196
Chapter 16. Developing a market........................................................................ 197
The current situation ........................................................................................... 197
Procurement ....................................................................................................... 197
Need for Change............................................................................................. 197
Procurement Reform....................................................................................... 200
Value for money, standards and cost benchmarking ...................................... 202
Assistive technology ........................................................................................... 203
Introduction ..................................................................................................... 203
Technology for Ageing Well ............................................................................ 204
Mainstreaming Assistive Technology .............................................................. 206
Cognitive and dementia AT Case Study ......................................................... 209
Using the Data ................................................................................................ 209
User Acceptance............................................................................................. 210
The Downsides ............................................................................................... 210
Assistive Technology and the DFG................................................................. 211
Support for people outside the DFG ............................................................... 211
Market provision.............................................................................................. 213
The role of local authorities ............................................................................. 214
Where people go for information..................................................................... 215
Paying for adaptations .................................................................................... 218
Incentivising home adaptations through the social care cap ........................... 223
Summary – helping people outside the DFG .................................................. 223
Recommendations – developing a market.......................................................... 224
Chapter 17. Tenure and equality......................................................................... 225
7

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Inequality of access to the DFG by tenure.......................................................... 225
Home owners.................................................................................................. 226
Registered providers ....................................................................................... 228
Council stock................................................................................................... 230
Social housing generally ................................................................................. 230
Private rented sector ....................................................................................... 231
Adaptations without delay ............................................................................... 232
Common parts grants and the Equality Act....................................................... 232
DFG for adaptations to communal areas ............................................................ 232
Level access in flats with shared facilities ....................................................... 235
Potential cost of providing level access to flats with shared facilities.................. 241
Lifts..................................................................................................................... 241
Housing Health and Safety Rating System (HHSRS) hazards ........................... 243
FOI data.............................................................................................................. 243
Summary points – Section 36 of the Equality Act ............................................... 245
Recommendations – tenure and equality ........................................................... 245
Chapter 18. Summary, conclusions and recommendations ............................ 246
Housing and Health Partnership Board .............................................................. 246
Making the service more visible.......................................................................... 246
Integrating services............................................................................................. 247
Resources .......................................................................................................... 249
The means test................................................................................................... 250
The upper limit.................................................................................................... 251
Regulation .......................................................................................................... 252
Developing a market........................................................................................... 252
Helping people outside the DFG......................................................................... 253
Tenure and equality issues................................................................................. 254
Conclusions ........................................................................................................ 255
Recommendations - overview ............................................................................ 257
Further research and development work ............................................................ 260
The Review Team ................................................................................................. 263
List of organisations contributing to the review ............................................... 264
Appendix............................................................................................................... 267
Appendix 1 - Proposed DFG Metrics .................................................................. 268
Appendix 2 Allocation formula ............................................................................ 269
8

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
A2.1 Income Deprivation Domain.................................................................... 269
A2.2 Other data sources investigated but not included in the allocations formula
modelling......................................................................................................... 270
Appendix 3 Means Testing ................................................................................. 271
A3.1 Current rates of allowances and premiums............................................. 271
A3.2 Example scenarios - details.................................................................... 272
A3.3 Summary of main differences between the two preferred options .......... 283
References............................................................................................................ 285
9

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Glossary
We have tried to avoid using acronyms, but you will see some abbreviations in the
text. They have had to be used in tables and diagrams to fit the space.
AA Attendance Allowance
ALMO Arms-Length Management Organisation
BAME Black, Asian and minority ethnic
BCF Better Care Fund
CA Carers Allowance
CSCR Care and Support (Charging and Assessment of Resources) Regulations 2014
CCG Clinical Commissioning Group
DFG Disabled Facilities Grant
DHSC Department of Health and Social Care
DLA Disability Living Allowance
DWP Department of Work and Pensions
ESA Employment and Support Allowance
EHS English Housing Survey
FOI Freedom of Information request
HB Housing Benefit
HIA Home Improvement Agency
HRA Housing Revenue Account
HMPP Home Modification Process Protocol
HWB Health and Wellbeing Board
ICES Integrated Community Equipment Service
IIDB Industrial Injuries Disablement Benefit
IMD Index of Multiple Deprivation
JSNA Joint Strategic Needs Assessment
LAC Looked After Child
MHCLG Ministry of Housing, Communities and Local Government
NHF National Housing Federation
ONS Office of National Statistics
OT Occupational Therapist
PIP Personal Independence Payment
RCOT Royal College of Occupational Therapists
RP Registered Provider
RRO Regulatory Reform (Housing Assistance) (England and Wales) Order 2002
Note: where web addresses are given in the text, these were live Nov 2018.
10

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 1. Introduction
The aims of this review
1.1 Across England the population is ageing, there are high numbers of disabled
working age adults and rising numbers of families with disabled children. The
majority live in ordinary housing, but most homes are not well designed for
disabled people. In 2014 just 7% of homes (around 1.7 million) had all four basic
accessibility features of level access, flush threshold, downstairs toilet, and
sufficiently wide doorways and circulation space
1
.
1.2 The Disabled Facilities Grant (DFG) is a means tested capital grant which can
contribute towards the cost of adapting a home, for example by installing a
stairlift, creating a level access shower room, widening doorways, providing
ramps and hoists or creating a ground floor extension. However, delivery of the
grant is changing. It is increasingly being used to provide a wider range of
solutions to the problems people face in their home.
1.3 This review is divided into two parts which will:
A. Provide an assessment of how the DFG is currently being used
B. Make evidence-based recommendations about how the DFG should change.
1.4 There are two main aims:
1) To support more people to live in suitable housing so they can stay
independent for longer. Many disabled and older people spend most of their
time in their home and the accessibility, warmth and comfort of that home has
a vital role to play in health and wellbeing. For disabled people of working age,
the home also needs to be a place that makes it easy for them to earn a living.
For families with disabled children the home should enable children to grow,
develop and lead as normal a life as possible.
2) To make the case for more joined-up action across housing, health and
social care. Suitable housing plays a key role in preventing accidents, allowing
swift return from hospital, restoring health and wellbeing, supporting carers and
encouraging independent living. Responsibility for the DFG at local authority
level is often split between different departments and directorates. The review
will look at the need for the DFG to be joined more closely with other services
to provide better support for disabled and older people.
1
Ministry of Housing Communities and Local Government (2016b) English housing survey 2014 to
2015: Housing for older people report, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-housing-for-older-
people-report.
11
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Why the review is needed
Changes since the last review
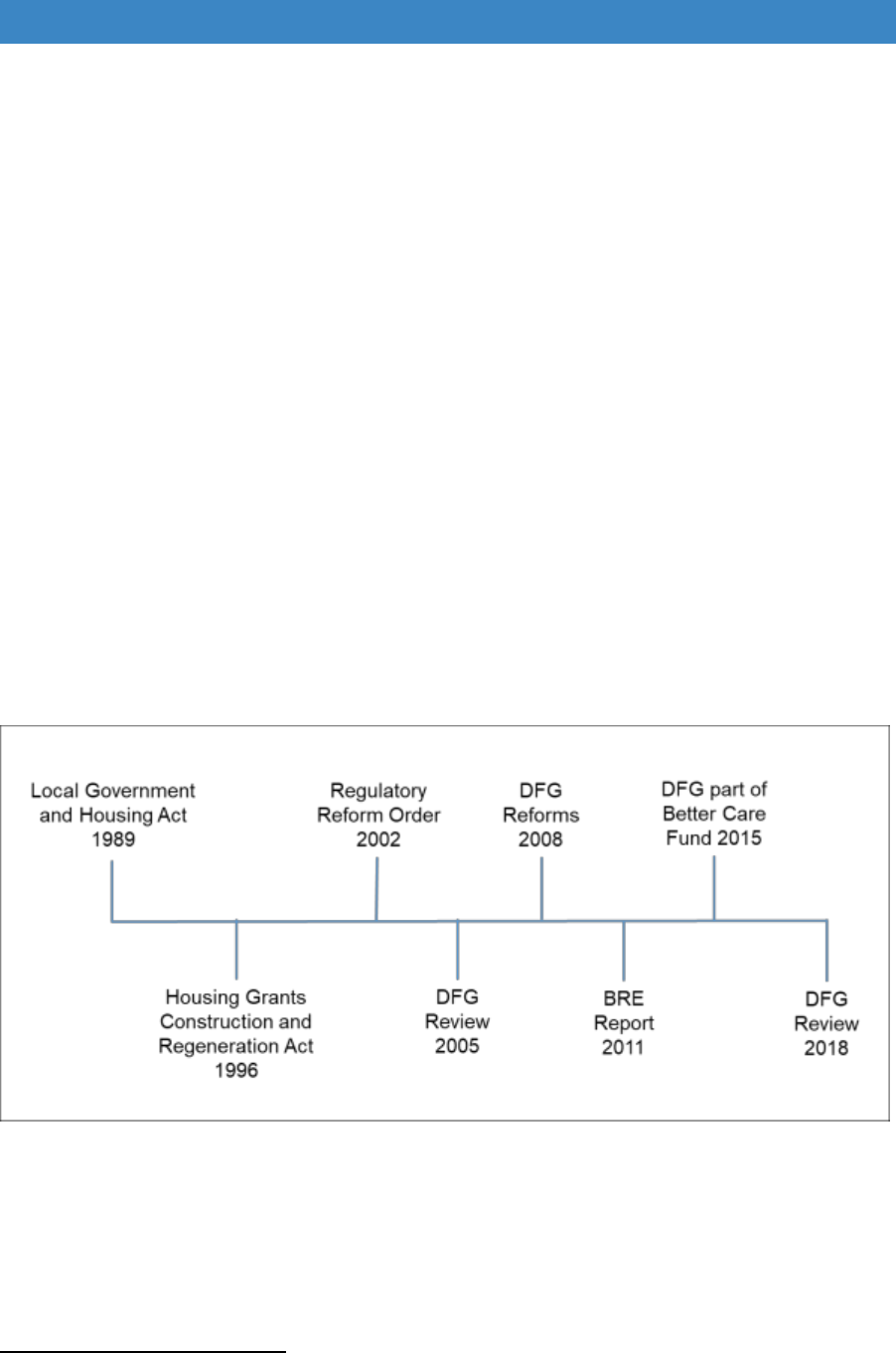
1.5 The Disabled Facilities Grant (DFG) is now nearly 30 years old. It was introduced
in 1989 as one small part of a raft of grants designed to improve the poorest
housing stock. The legislation was reviewed in the early 1990s, and it is the 1996
Housing Grants Construction and Regeneration Act which governs operation of
the DFG today (Figure 1.1). Further changes to introduce more flexibility in the
use of the DFG were brought in with the Regulatory Reform (Housing Assistance)
(England and Wales) Order 2002 (RRO). Over the intervening period, all the
housing renewal and improvement grants that were part of the original legislation
have been discontinued and the only grant that remains is the DFG.
1.6 The DFG is a mandatory grant, which means that it is a legal requirement for
local authorities to provide help to people who meet the eligibility criteria, whether
or not the authority has sufficient budget
2
. These criteria include ensuring that
the works are necessary and appropriate to meet the needs of the disabled
person, and that they are reasonable and practicable given the age and condition
of the property.
Figure 1.1 DFG Timeline
1.7 The last major review of DFG was in 2005, which immediately led to the removal
of the means test for children and young people aged 18 or under and other
significant changes which came into effect in 2008. These took away the ring
fence on funding; raised the maximum grant limit from £25,000 to £30,000; and
allowed passporting of people on certain mean-tested benefits through the test
2
A high court ruling in 1998 stated that local housing authorities are not entitled to have regard to
their financial resources in determining whether or not to approve an application for a DFG for
purposes within Section 23(1) of HGCRA 1996 (R v Birmingham City Council ex p Taj Mohammed
(1998) Times Law Reports 429, QBD).
12

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
of resources to remove unnecessary bureaucracy. The 2008 reforms also
allowed more flexibility in the use of the grant, for example: to fast-track grants;
to make homes safe and warm for people being discharged from hospital; or to
help people relocate to more suitable housing. However, not all the
recommendations arising from the 2005 review were implemented. Many of the
remaining issues are dealt with in this review.
1.8 In 2011, the Building Research Establishment (BRE) did an in-depth review of
the means test and the allocation methodology. The formula they developed for
the allocation of resources has been used to distribute most of the additional
central government funding since this date. However, a more recent report on
the DFG suggested that the distribution of resources might need further changes
to provide a more equitable spread
3
.
1.9 Recent and substantial changes to house prices, benefits, retirement ages and
the costs of work mean that the allocation formula, the means test and the upper
limit all need reviewing.
1.10 Over the years there have also been a considerable number of court judgements,
Ombudsman reports and letters of guidance which have had an impact on the
use of the grant and the delivery process. This plethora of different sources of
information needs bringing together to give local authorities a blueprint for
effective operation of the grant.
Changing context
Integration
1.11 The context in which the DFG is delivered has also changed significantly in the
last decade. Although the DFG is about altering the built environment, it is also
about supporting disabled and older people to be independent, enabling carers
to continue their role safely, preventing accidents and helping people to return
from hospital. It therefore crosses the boundaries between housing, health, and
social care
1.12 Reflecting this cross-sector role, in April 2015 the grant became part of a joint
health and social care budget, the Better Care Fund (BCF). Responsibility for
funding the DFG is now held by the Department of Health and Social Care
(DHSC). The Ministry of Housing, Communities and Local Government
(MHCLG) continues to lead on policy and the distribution of funding.
1.13 At national level there is beginning to be a clearer focus on the integration of
housing with health and care services. In March 2018 an updated Memorandum
of Understanding on Improving Health and Care Through the Home was signed
3
Mackintosh, S. and Leather, P. (2016) The Disabled Facilities Grant Before and after the
introduction of the Better Care Fund, Glossop: Foundations.
http://www.foundations.uk.com/media/4665/dfg-report-final-interactive-converted-draft-6-small.pdf
13

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
by all the principal national organisations concerned with the delivery of housing,
health and care services.
1.14 The way services are delivered at local level is also changing, driven by the 2014
Care Act, Sustainable Transformation Planning for health and social care, and
local authority restructuring and devolution. Good practice is evolving as
transformation and service integration takes place. The review looks at the
different models that are developing and how this is beginning to join-up formerly
separate services and provide more holistic solutions for disabled and older
people.
1.15 New local structures at strategic level may be needed to ensure that this best
practice gets properly embedded across the country to enable disabled and older
people get access to fast and effective services no matter where they live.
Increased resources
1.16 Since the DFG became part of the BCF there has been a significant increase in
central government resources. In 2014/15 central government contributed
£220m, but by 2017/18 this had more than doubled to £473m in total. There is a
need to show how this has impacted on local funding contributions and whether
there has been a significant increase in the number of people helped to remain
independent each year.
Ageing population and rising numbers of disabled people
1.17 The impact of the ageing population in the UK has begun to be much more
apparent. The pressures on health and social care have been increasing,
particularly in the winter of 2017/18 when there were delays in accident and
emergency departments and a shortage of hospital beds. Research is beginning
to demonstrate the role adaptations play in reducing accidents, enabling faster
hospital discharge, providing support to carers, and enabling people to remain
living in their own homes for longer, rather than needing residential care. The
need for services that wrap around the patient or service user, rather than them
having to seek out relevant services from a myriad of different sources is also
becoming better understood, which will affect the findings of the review.
Changing expectations and impact of technology
1.18 The review also needs to consider the evidence about what people feel about
their homes, the type of adaptations that they want to see provided and how
this might affect how the DFG could develop in future. Expectations are
changing and there are new materials and advances in information technology
and artificial intelligence which are rapidly being incorporated into people’s
homes. The DFG needs to evolve if it is to remain relevant for the next decade
and beyond.
Changes in tenure
1.19 When the DFG was originally conceived it was mainly for people who were low
income home owners living in poorer housing. Since then, registered provider
tenants (housing associations) have begun to use the DFG in much greater
14

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
numbers, but the DFG it is not used by tenants in the council stock who have a
separate funding stream through the housing revenue account.
1.20 The mix of tenures is changing with increasing numbers of disabled people now
in the private rented sector. Adaptations in the private rented sector are more
difficult to deliver as people often have short-term tenancies. This report makes
some suggestions about better ways of working with landlords. Tenure issues
are not explored in depth and need further review.
Problems with service delivery
1.21 Over the years there have been continual complaints about DFG delivery. A CLG
Committee report on Housing for Older People pointed out that the DFG followed
‘a clunky process’ and that waiting times varied significantly between authorities
4
.
A report by the Equality and Human Rights Commission also said that grant
delivery was too slow
5
.
1.22 The 2005 review pointed out the lack of strategic oversight, the paucity of
evaluation information and the absence of effective performance targets. It also
made the point that part of the strategic challenge was to shift the thinking from
‘welfare’ to ‘investment’ so that decisions were not made on the basis of lowest
cost but instead looked at the long-term health and wellbeing of the disabled
person and their family. These issues are key areas that this review addresses.
The focus of the report
1.23 This review examines the current situation and shows some of the ways in which
the grant might not be working as well as it might. However, the emphasis is on
ways in which DFG delivery could change in future and how it can move from
being a stand-alone service to being part of a package of provisions to help
people remain independent. It is a practical review with detailed information
about new ways of working that could drive service change. It also uses evidence
to provide options for Government about future allocation of resources and
means testing.
1.24 Throughout the report, the focus is on the disabled or older person and how they
can be put at the centre of service provision. The report considers what would
make it easier for them, and their families, to find their way through what can be
confusing service pathways. It also considers how those who are not eligible for
the DFG, or chose not to use this funding route, might go about getting advice,
4
Communities and local Government Committee (Feb 2018) Housing for older people: Second report
of session 2017-19, London: House of Commons.
https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/370/370.pdf.
5
Equalities and Human Rights Commission (2018) Housing and disabled people: Britain’s hidden
crisis. https://www.equalityhumanrights.com/sites/default/files/housing-and-disabled-people-britains-
hidden-crisis-main-report.pdf.
15

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
information and support to create a home environment that helps them remain
active and independent.
1.25 Prevention is a major issue. Many services are not delivered in an optimal way
because they are dealing with people at crisis point. The DFG has a key role to
play in prevention as providing adapted housing when people are first
experiencing difficulties is much more effective long-term than reacting when
they have a serious injury or have become very frail. The review will look at how
this preventative role might be delivered more effectively.
1.26 The report only covers the DFG in England. The legislation and arrangements
for providing adaptations are different in the other parts of the UK. However,
where lessons can be drawn from other jurisdictions these will be mentioned in
the report.
16

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 2. Methodology
The review
2.1 There are two main parts to the review, each with several components:
Part A: How the DFG is used currently
DFG funding
Who receives the grant
Types of adaptations and costs
Costs and benefits to local authorities
Processing arrangements and waiting times
Part B: How the DFG should change
The bigger picture
Local delivery
Working better together
Allocation of resources
Funding
The means test
Regulation and the upper limit
Developing a market
Tenure and equality
Methodology
2.2 The review took place over a very short period: February-May 2018. The team
conducting the review already had a depth of understanding about the DFG.
They had worked on previous reviews or had been involved in national or local
service improvement. They understood the variation in delivery across the
country, particularly the differences in operation between unitary and county
authorities. They knew the data sources available, had carried out evaluation of
delivery methods, and examined the evidence about the outcomes of
adaptations. Although the methodology was inevitably constrained by the
restricted time frame, the team was able to access a considerable amount of
national and local evidence and consult a wide range of organisations. Sources
of evidence included:
Analysis of data from LOGASnet returns made annually by local authorities
to the Ministry of Housing, Communities and Local Government combined
with data from a series of Freedom of Information requests. This gave a
17

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
national picture of annual budgets, the value of work, information on who
receives the grants, time scales, costs of work and type of work carried out.
Three consultation events were held, each with about 70 participants from
local authorities, home improvement agencies and other organisations. An
online survey provided further feedback with responses from 234 people.
There was almost equal representation from people working in occupational
therapy roles (44% online) and those in housing (43% online). Opinions were
obtained relating to key aspects of the review, including: how the means test
might be reformed; whether the upper limit should be changed; how best to
link the DFG to health and social care; effective methods of delivering the
grant; and how to help people outside of the DFG.
The review also drew on the findings of previous consultation events
held by Foundations, the Home Adaptations Consortium and the Royal
College of Occupational Therapists (RCOT) such as: the DFG Summit
December 2016; DFG Champions events over the period 2015-17; and
comments on the DFG Champions Facebook page.
Means test - The review considered the existing means test and compared it
with means tests being used for state benefits (both legacy and those being
introduced) and social care. The methods and results of assessing the levels
of income needed for recipients, the methods by which earnings, income and
capital are used to determine resources and the ways in which those are used
to determine eligibility were all examined. These were modelled against a
number of household types using a model derived from Ferret’s Future
Benefits Model (FFBM) which enabled outcomes to be compared. The effects
of bringing the existing means test in line with the parameters used in other
current means testing was considered, allowing a number of options to be
proposed.
Allocations methodology - the starting point for the review of the allocations
methodology was to create a baseline of the number of people within the local
authority or region who could potentially benefit from adaptations to their
home and then add in ‘adjustment’ factors one by one to examine the
cumulative effect of each stage on the allocation of funds (using 2016/17
funding levels); this helped determine where the greatest shifts in the
distribution of allocations might occur. All adjustment factors, which were
considered suitable proxy indicators of DFG demand, were given equal weight
to help assess their impact. Due to the timescale of this project, the review
focussed on two regions; London, which is very diverse, and Yorkshire and
Humberside, which has a mix of rural and urban authorities. As with the
previous BRE review in 2011, it was considered imperative that the data
available for the proxy indicators of DFG need should meet specific criteria;
simplicity, transparency, be readily accessible, be fair, and provide
sustainability over the medium-term (at least 5 years) but be responsive to
changes in the population and their circumstances.
Interviews with staff from selected local authorities demonstrating
aspects of good practice in grant delivery. These provided more detail
18

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
about budgets, operating costs, sources of income and management
structures.
Collaboration with other researchers conducting parallel lines of inquiry
provided further information, including: a pilot study of DFG-funded bathroom
adaptations being conducted in Nottingham
6
; minor adaptations research
being carried out by the Royal College of Occupational Therapists and the
Housing LIN
7
; and a study of good practice in the delivery of adaptations to
older people by the Centre for Ageing Better and Care & Repair England
8
.
Meetings with representatives of the national organisations providing
support to local government and the housing association sector were held to
discuss how DFG delivery and oversight might change and to determine how
it might be better joined up with other health and social care services. One
meeting was done in conjunction with the researchers involved in the study of
minor adaptations.
Meetings with the private market sector, combined with online searches
and a short literature review, looked at how the DFG could evolve to embrace
new products and materials and how more people could be helped outside of
the DFG.
Telephone and email contact with academic and policy staff in other parts
of the UK enabled the team to gain insights into alternative methods of DFG
delivery and effective integration of the DFG with health and social care
services.
A short review of the academic, policy and practice literature provided
additional material to determine what disabled and older people want to see in
terms of adaptations and DFG reform.
2.3 The first part of the report, Part A, looks at the evidence relating to the current
situation and the need for change, with a summary of the main findings at the
end of each chapter. In the second section, Part B, these findings are used to
assess the options for to improve services, with a list of recommendations at the
end of each chapter. The main findings and recommendations are brought
together at the end of the report.
6
Whitehead, P., James, M., Belshaw, S., Dawson, T., Day, M. and Walker, M. (2016) Bathing
adaptations in the homes of older adults (BATH-OUT): Protocol for a Feasibility Randomised
Controlled Trial (RCT) BMJ Open. http://dx.doi.org/10.1136/bmjopen-2016-013448.
7
Royal College of Occupational Therapists (In Press) Adaptations without delay: a guide to thinking
about and delivering adaptations differently. London: Royal College of Occupational Therapists.
8
Adams, S. and Hodges, M. (2018) Adapting for ageing: Good practice and innovation in home
adaptations, London: Centre for Ageing Better. https://www.ageing-
better.org.uk/sites/default/files/2018-10/Adapting-for-ageing-report_CfAB_0.pdf.
19

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Part A
How the DFG is used currently
20
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 3. DFG funding
Funding sources and trends
3.1 Information on DFG budgets and spending nationally comes from two main
sources: the annual returns made by local authorities to central government
(LOGASnet); and Freedom of Information requests (FOIs) by Foundations.
LOGASnet returns have become less complete over the last few years (only
returned by 66% of authorities in 2016/17), but they are still one of the best
sources of information at national level
9
. The returns for 2016/17 included some
additional questions on the use of discretionary grants and the time taken to
process cases.
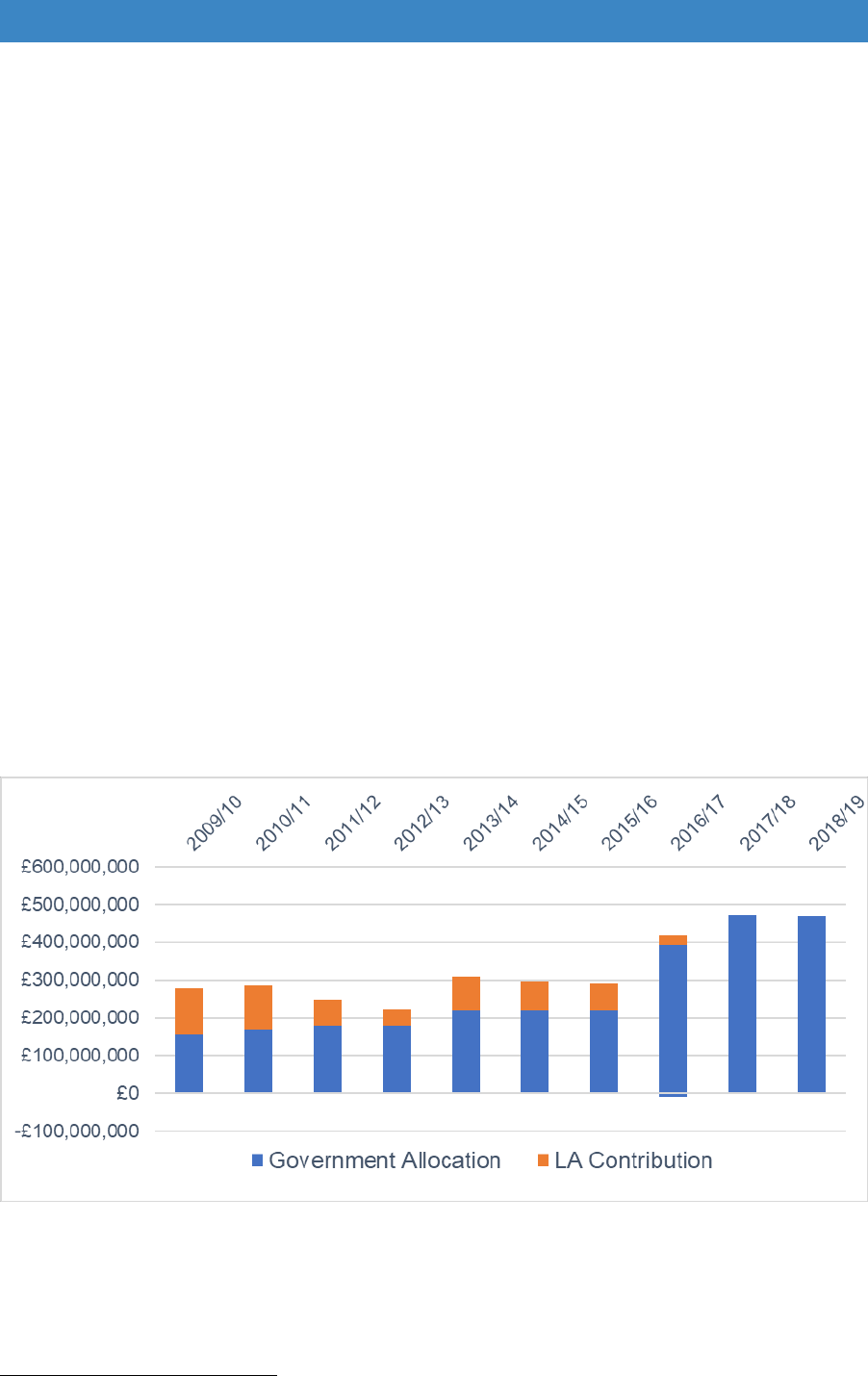
3.2 DFG funding has fluctuated over the last decade (Figure 3.1). Until 2008, local
authorities had to provide a 40% contribution to DFG budgets to match the 60%
coming from central government. The total amount was ring-fenced and had to
be spent on mandatory work as laid down in the 1996 Act. In 2008 the ring fence
was removed to give local authorities more flexibility to use the grant for
discretionary purposes. It was thought this might reduce local authority capital
contributions, but despite the greater freedom, matched contributions continued
for several years (Figure 3.1).
Figure 3.1 Annual DFG budget for England
?
?
Source: Annual Government allocations from official figures, LA contribution based on average
percentage contribution from LOGASNET (2009/10 – 2014/15) and Foundations FOI request (2015/16
– 2016/17).
2016/17 shows negative contribution due to top-slicing of allocation for other purposes.
Data on LA contribution not yet available for 2017/18 onwards.
9
For further details about LOGASnet see Mackintosh, S. and Leather, P. (2016) ibid.
21
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
3.3 Austerity measures were introduced in the 2010 Autumn Statement. Central
government funding for Repairs Grants ceased entirely at this point which
removed £300m of annual funding from private sector housing. This was often
used to supplement the adaptations budget, and when it disappeared local
authority contributions were cut in many areas, although the impact was not fully
felt until 2012/13. Local authority funding picked up in 2013/14 but declined to a
very low level in 2016/17 at the point when central government funding increased
significantly. The overall budget is now considerably higher than it was in
2009/10.
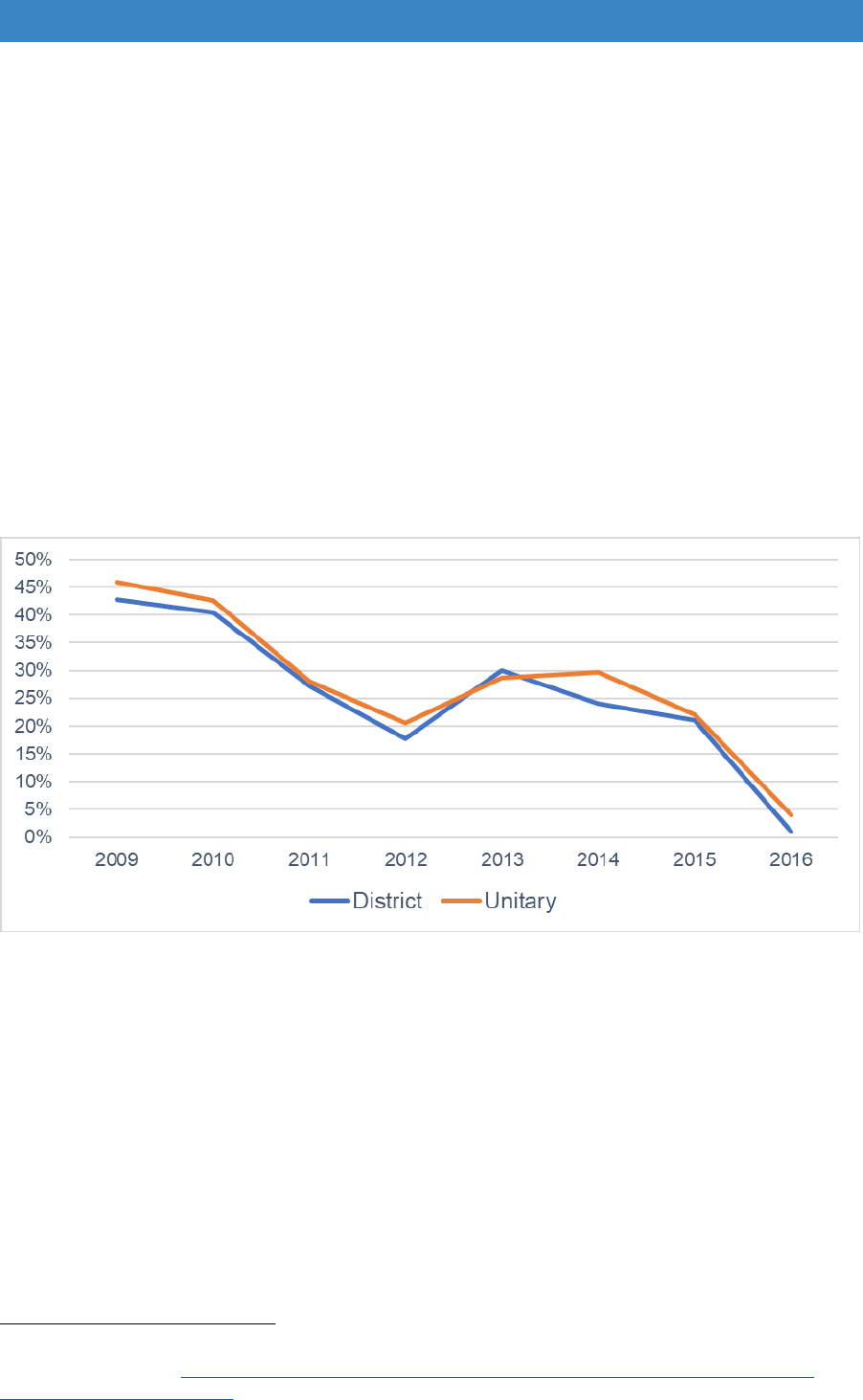
3.4 Figure 3.2 shows that local authority contributions have declined in both unitary
and two-tier authorities. They have also fallen at a similar rate in areas with
retained council stock, compared to those where the stock has been transferred.
Figure 3.2 Average local authority contributions 2009-2016.
Source: LOGASnet and Foundations FOI requests
3.5 In the 2015 Spending Review, it was announced that central government
contributions to the DFG would increase until the end of the decade to help meet
the objectives of the 2014 Care Act and the Better Care Fund.
“The Care Act reforms introduced in April focus on wellbeing, prevention
and delaying the need for social care. In support of these principles, the
Spending Review includes over £500 million by 2019-20 for the Disabled
Facilities Grant, which will fund around 85,000 home adaptations that
year. This is expected to prevent 8,500 people from needing to go into
a care home in 2019-20”
10
.
10
HM Treasury (Nov 2015) Spending Review and Autumn Statement 2015, Adult Social Care,
Section 1.109, p. 33. https://www.gov.uk/government/publications/spending-review-and-autumn-
statement-2015-documents.
22
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
3.6 It was clearly hoped that local authorities would continue to add resources and
that the number of grants delivered would more than double from the 41,000
completed in 2014/15. With the decline in local authority contributions, overall
DFG funding levels only rose 44% from 2015/16 to 2016/17, and a further 13%
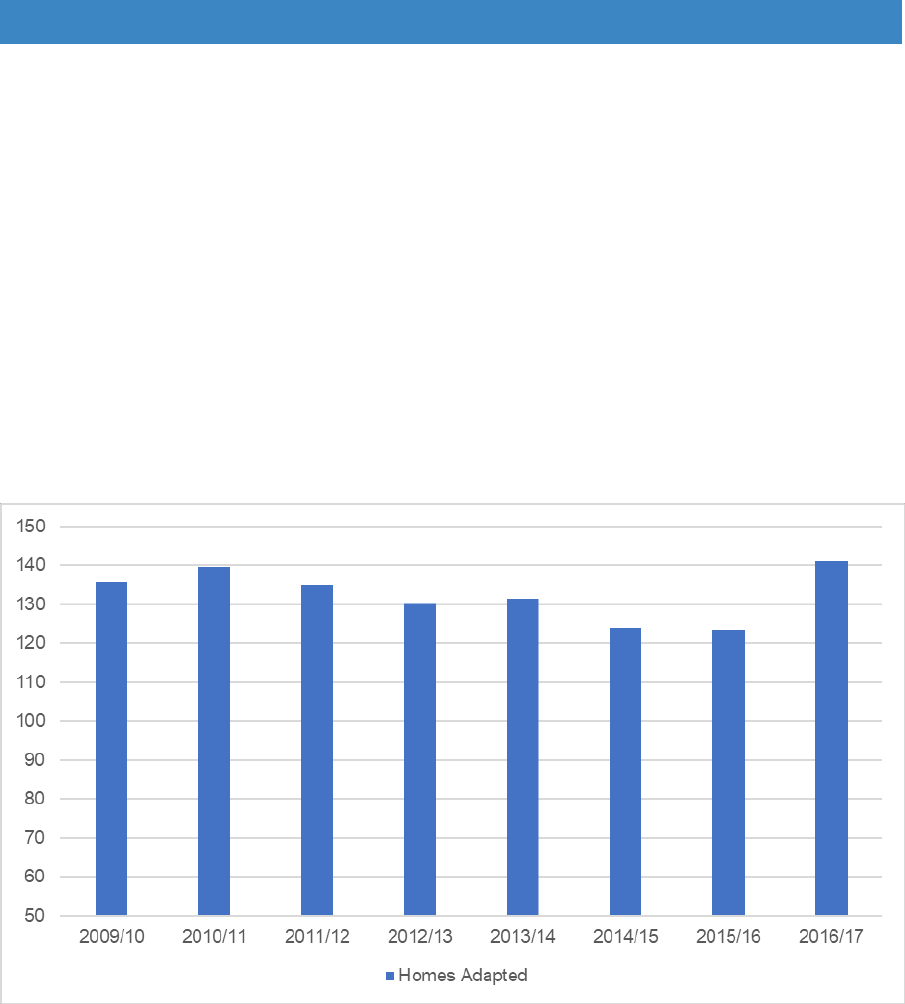
to 2017/18 (Figure 3.1). Grant completions have taken longer to respond. The
average number of grants per authority declined after 2010/11. Completions only
increased after 2015/16 when they rose from an average of 123 to 141 per
authority in 2016/17; a rise of only 15%. This takes the levels of completions back
to the amount achieved in 2010/11, before austerity measures were introduced
(Figure 3.3). In 2010/11, about 45,500 grants were completed nationally, and we
estimate it was only 46,000 in 2016/17.
Figure 3.3 Average number of DFGs completed per authority 2009/10-2016/17
Source: LOGASnet – includes both mandatory and discretionary grants for 2016/17
Reasons behind the trends
3.7 The reasons why numbers of DFG completions are not increasing as fast as
expected are complex and may include the following:
a) Time lag – in the first year that funding increases, the number of grant
approvals may rise. However, due to the time it takes to schedule building
work the number of grant completions may not show in the figures until the
following year. The figures for 2017/18 are not yet available to show the true
impact of the increase in central government funding.
23

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
b) Delays in obtaining DFG allocations - DFG resources used to be passed
directly from central government to the housing authorities based in unitary
authorities and at borough or district level. Now the grant is part of the BCF,
in shire authorities it goes to the county before being passed to the boroughs
or districts.
In 2016/17, there was a small negative contribution when 22% of authorities
saw their budgets top sliced for other purposes, mainly to meet social care
obligations under another funding stream that was discontinued. Other
authorities may have received their allocation quite late in the year. The
guidance issued in a letter to all authorities and in the BCF planning
requirements for 2017-19 states clearly that the statutory duty on local
housing authorities to provide the DFG to those who qualify for it remains
11
.
“DFG funding allocated by central government should be
passed down by the county to the districts (in full, unless
jointly agreed to do otherwise) to enable them to continue
to meet their statutory duty to provide adaptations.”
12
Although top slicing may have impacted grant completion levels in 2016/17
(the most recent LOGASnet data currently available), it appears to have
affected few authorities in 2017/18.
c) More discretionary grants - discretionary grants include: fast-tracked grants
for hospital discharge; grants for people with dementia; funding to improve
heating; and a range of other measures to ensure that people can remain
safely at home. Many are given without a means test to ensure that they can
be delivered quickly. These grants are only just being introduced in most
areas and may not be reflected in the figures until 2017/18. LOGASnet returns
in 2016/17 included totals of discretionary grants for the first time (they are
included in the data in Figure 3.1 above). However, three quarters of
authorities did none, 17% did less than 10 and only 5% of local authorities did
more than 50 in 2016/17 (Foundations FOI 2017). It is hoped that more of
these flexible grants will be shown in the data for 2017/18.
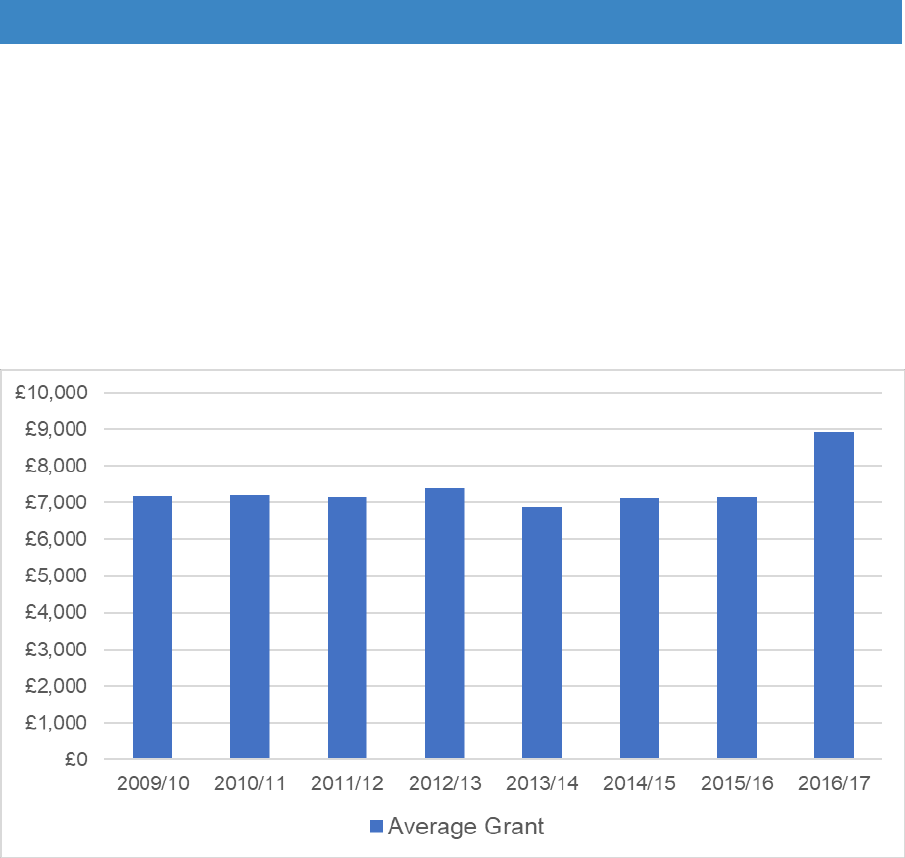
d) Rising cost of work – until central government contributions increased after
2015, local authorities were struggling with restricted DFG resources relative
to demand. Therefore, there was a focus on value for money and on driving
down costs. As a result, the average remained constant for many years,
despite rising building costs (Figure 3.4).
11
NHS England (2017) Integration and Better Care Fund planning requirements for 2017-19.
https://www.england.nhs.uk/wp-content/uploads/2017/07/integration-better-care-fund-planning-
requirements.pdf.
12
NHS England (Aug 2017) The Better Care Fund Planning Requirements 2017-19: Frequently
Asked Questions, p. 9. https://www.england.nhs.uk/wp-content/uploads/2017/08/bcf-planning-
requirements-faqs.pdf.
24
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
In 2016/17 average costs rose from around £7,000 over the period 2009/10-
2015/16 to nearly £9,000 in 2016/17, showing that the overall increase in
resources has allowed prices to rise, perhaps to more realistic levels (Figure
3.4). Cost rises may also reflect the increased complexity of cases which is
discussed later in the report. Minimal specifications may not provide the best
solutions, and a relaxing of very tight cost controls may be beneficial, but it
has the effect of reducing the overall number of grants delivered.
Figure 3.4 Trends in average grant value 2009/10 to 2016/17
Source: LOGASnet
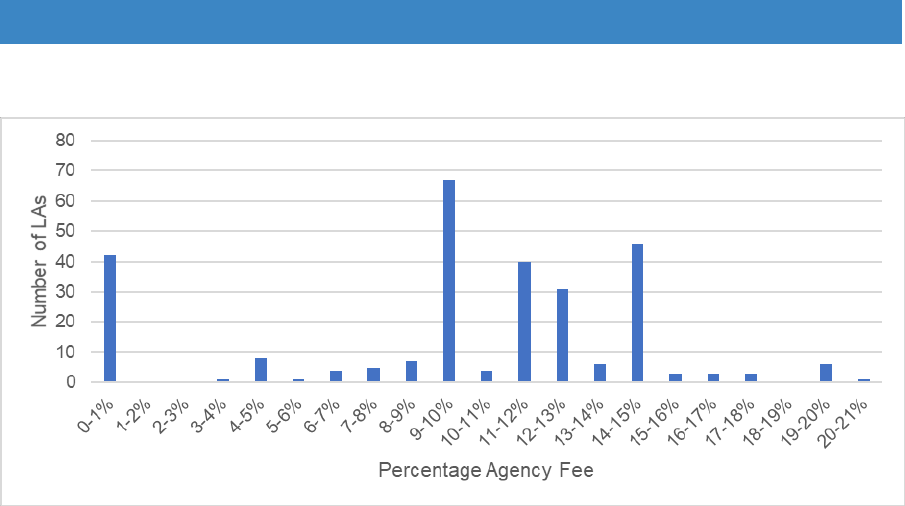
e) Problems with revenue funding – the increase in DFG capital allocations
happened at a time when local authorities were continuing to cut staff to
reduce costs. This may have impacted on their ability to deliver more
adaptations in 2016/17. To maintain staffing levels, some authorities began
to look at other ways of finding revenue funding. As a result, more started to
charge fees of 10-15% on top of each DFG grant to cover running costs
(these fees are not charged on to DFG recipients). A few other authorities
top-sliced the budget to cover service costs. This may have further reduced
grant completion numbers (Figure 3.5).
25
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 3.5 The range of agency fees charged as part of the DFG in 2016/17
Source: Foundations FOI 2017
The need to increase the number of grants
3.8 Given the pressures on health and social care and the rising numbers of people
living with impairments or long-term conditions, it is essential to enable more
people to remain independent in their homes. There is an urgent need to work
towards the target of 85,000 grants per year, which was set when central
government funding increased in 2015. How revenue funding could be increased
and DFG funding used to help more people is discussed further in Section B.
Summary - funding issues
There are several reasons why numbers of grants have not increased as much as
expected by 2016/17. These include: reduction in local authority contributions;
delays in funding being passed to authorities; lack of detail about use of
discretionary grants; a rise in the complexity of work; and the relaxation of strict
cost controls resulting in an increase in the average cost of work.
Austerity has affected the ability of local authorities to add their own investment,
both in terms of grant spending and revenue costs. Using the grant to provide fees
to cover staff and overhead costs has further reduced outputs.
It will not be until the LOGASnet figures for 2017/18 are available that the full
benefits of increased central government spending will become apparent.
26
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 4. Who receives the grant
4.1 The DFG is designed to help people of all ages and with a range of impairments.
A person is deemed disabled if: their sight, hearing or speech is substantially
impaired; they have a mental disorder or impairment of any kind or they are
physically substantially disabled by illness, injury, or an impairment present since
birth.
4.2 The grant provides adaptations to allow access to the home and garden, permit
use of all the normal facilities and, where appropriate to enable a disabled person
to provide care for others. It also allows for a care plan to be implemented to
enable the disabled occupant to remain living in their existing home as
independently as possible
13
.
Age of DFG recipients
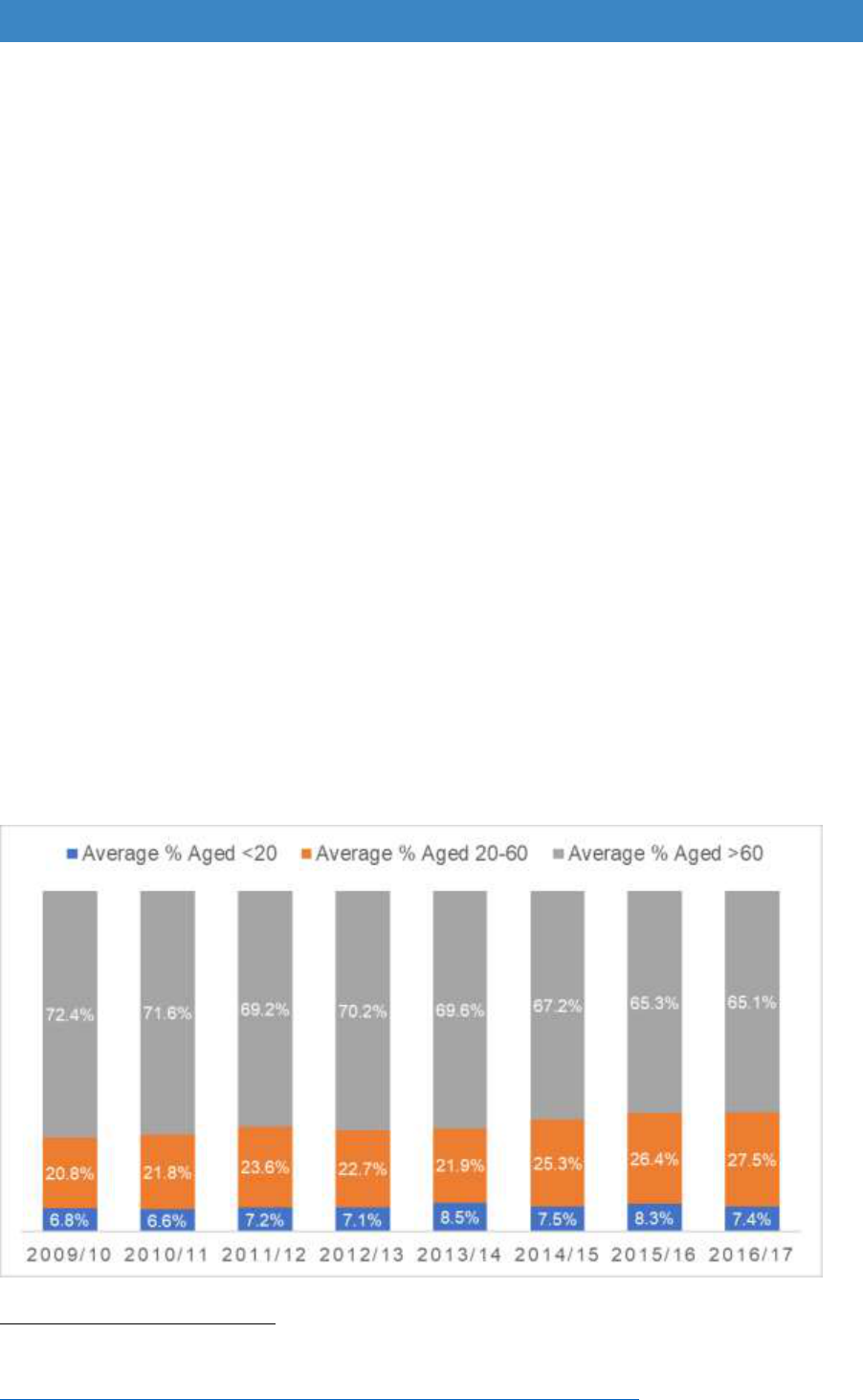
4.3 In 2016/17 most grants (65%) went to people aged 60 and over. The proportion
has gradually decreased since 2009/10, with slightly more grants going to people
of working age and to children and young people under 20 (Figure 4.1). However,
the number of grants going to people under 20 is still relatively small and
fluctuates slightly from year to year.
Figure 4.1 Trends in age of people receiving the DFG
Source: LOGASnet
13
Wilson, W. and Fears, C. (Dec 2016) Disabled Facilities Grants for home adaptation, Briefing Paper
No. 03011, London: House of Commons Library.
http://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN03011.
27
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
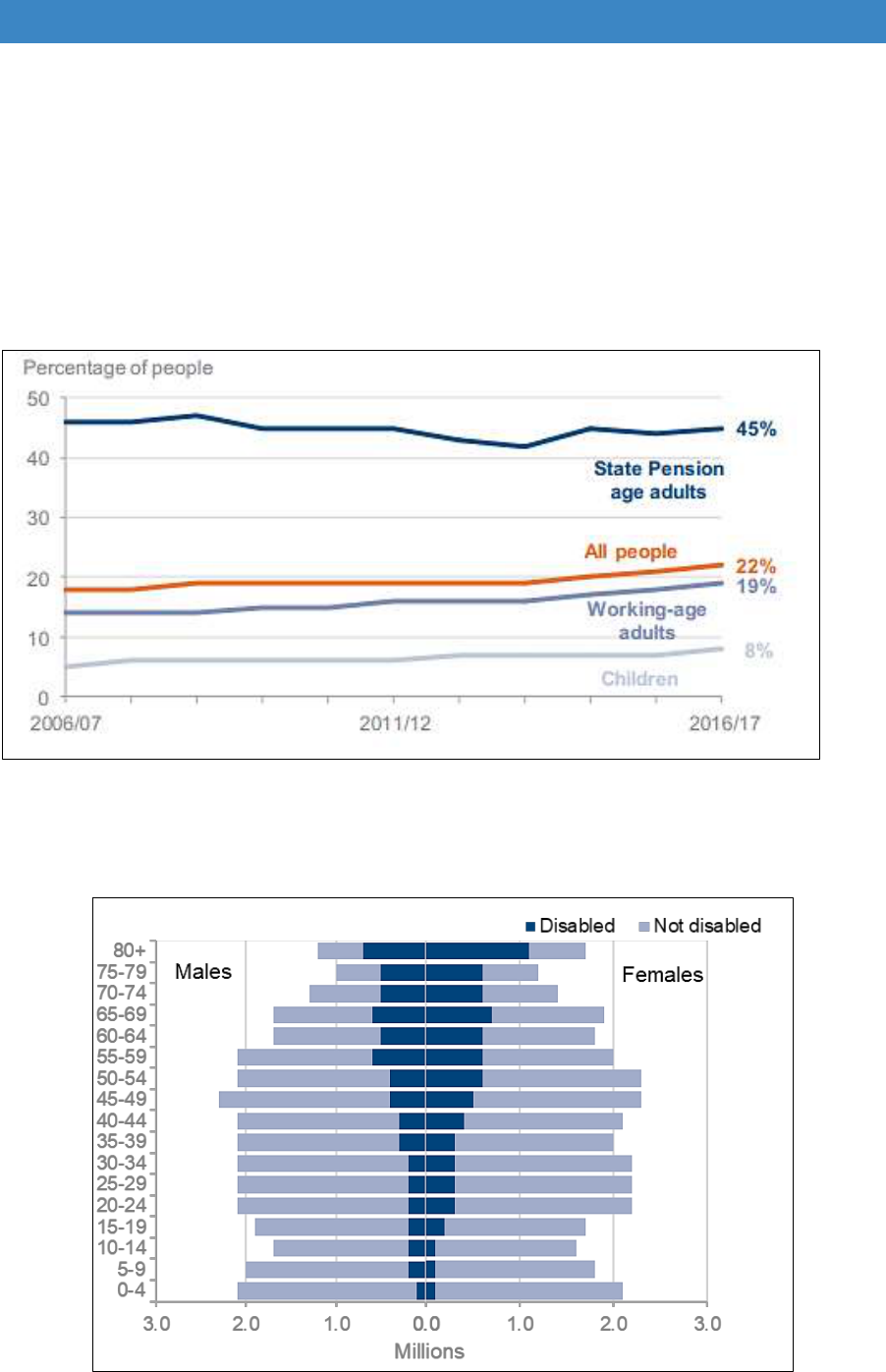
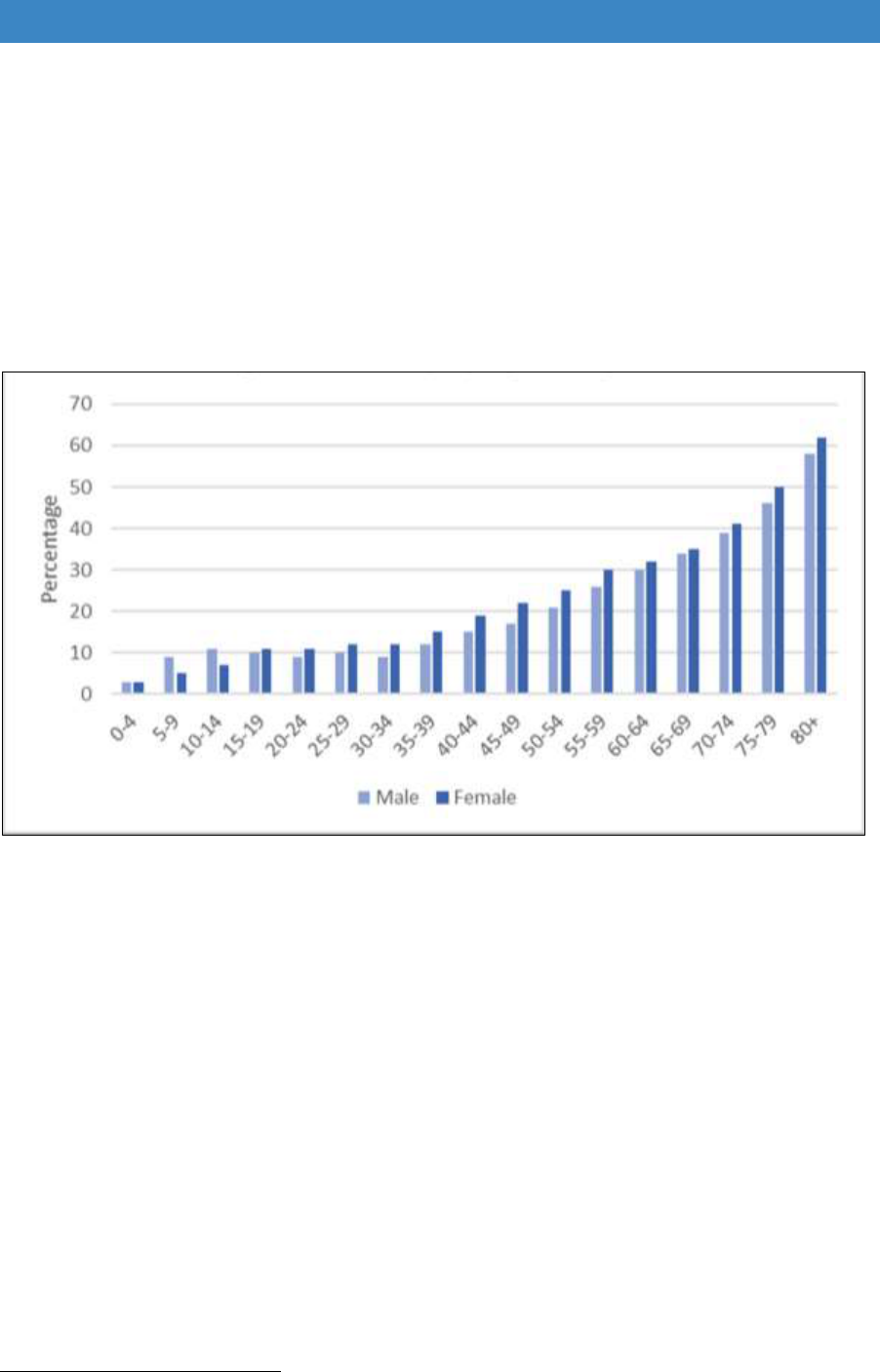
4.4 These proportions reflect broader trends in levels of disability in the UK, with a
rise in the number of children and working age adults with impairments. Medical
advances are enabling disabled children to live longer lives and helping more
people survive illness and accidents (Figure 4.2). There is a predominance of
disabled boys in childhood, while women are slightly more likely to be disabled
than men as people age. There is high proportion of disabled women in the later
stages of life due to their longer life expectancy (Figure 4.3).
Figure 4.2 Disability prevalence by age group 2006/07 to 2016/17
Source: Department of Work and Pensions (Mar 2018) Family Resources Survey 2016/17, Table 4.1.
Note: figures are for the UK.
Figure 4.3 Prevalence of disability by age and gender UK
Source: Family Resources Survey 2016/17 Table 4.3 - average of 2014/15-2016/17
28
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
4.5 Higher numbers of older people are likely to get DFG funding in any year due to
the substantial rise in the proportion of people with impairments as people reach
their 70s and 80s (Figure 4.4). The preventative role of adaptations in helping
people before they reach crisis point needs to be addressed. Services also need
to reflect the fact that many of those needing help will be on their own. The
English Housing Survey shows that in 2014/15 47% of those aged 75-84 and
61% of those aged 85 and over were living alone
14
. Many of those will be single
women.
Figure 4.4 Disabled people by age UK
Source: Family Resources Survey 2016/17 Table 4.3
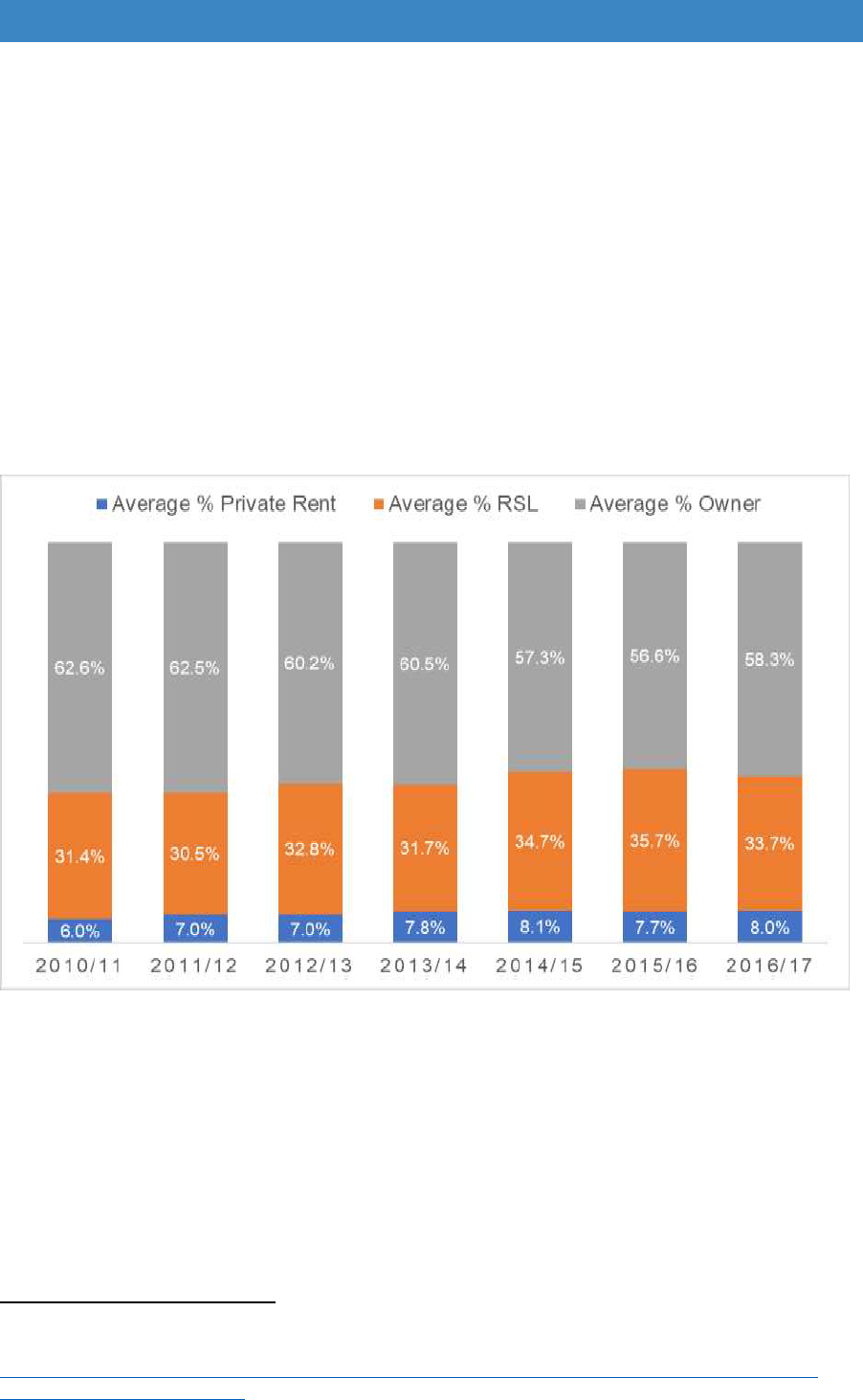
Tenure of DFG recipients
4.6 It is useful to look at who gets the grant by tenure, and the likely future trends, to
see how this might affect grant allocations and the delivery process. Applicants
for DFG funding can be owners, those renting privately and tenants of registered
providers, but not council tenants. Landlords are allowed to apply directly on
behalf of their tenants.
Home owners
4.7 Home owners on low incomes have always been the biggest recipients of DFG
funding as the grant mostly goes to older people, and 76% are home owners. In
2016/17, 58% of grants went to home owners but there has been a slight
decrease in the proportion going to this tenure since 2010/11 (Figure 4.5). It is
14
Ministry of Housing, Communities and Local Government (2016b) English housing survey 2014 to
2015: Housing for older people report, ibid.
29
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
an optimistic sign that in the English Housing Survey over half (55%) of
households over 75 that required adaptations in their home said that they already
had them installed (although there was no independent check on the quality or
appropriateness of these adaptations)
15
. There has been a lot of investment in
the owner-occupied stock over the last 30 years, with showers and wet rooms
seen as desirable features which may start to reduce the need for the
replacement of baths.
4.8 However, the English House Condition Survey shows that people over 65 are
still by far the biggest group requiring adaptations. Home ownership is also
common in the cohort approaching retirement and as the population continues
to age, grants for older home owners will continue to dominate DFG allocations.
Figure 4.5 Trends in tenure of DFG recipients
Source: LOGASnet
Registered providers
4.9 A third of grants go to tenants of registered providers. Many disabled people are
in this sector as they tend to have lower incomes and cannot afford home
ownership. However, registered providers only hold between 5 and 15% of the
housing stock in any local authority area. From previous research, areas where
15
Ministry of Housing, Communities and Local Government (2016a) English housing survey 2014 to
2015: Adaptations and accessibility of homes report, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-adaptations-and-
accessibility-of-homes-report.
30
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
stock has been transferred have a higher proportion of grants going to registered
providers than those with retained council stock
16
.
4.10 Registered providers’ use of the DFG seems disproportionate as their housing is
newer on average, with a higher proportion of accessible homes. It is probably
because registered provider tenants have a clear route. They are signposted
directly to the DFG with some landlords applying on their behalf. In contrast,
home owners and private tenants have very few ways of finding out about the
grant, as it is seldom advertised and not easy to find on local authority websites.
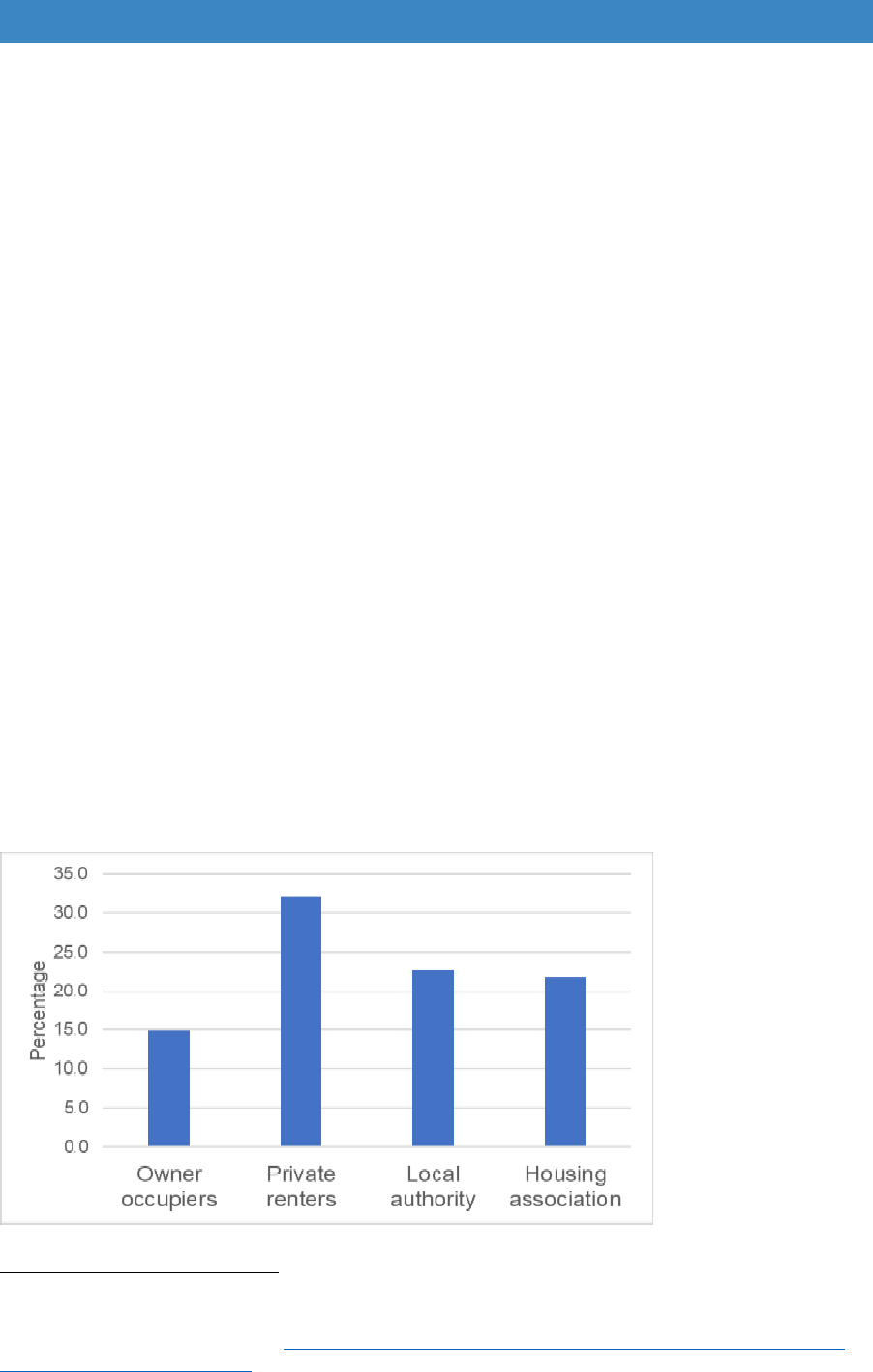
Private rented sector tenants
4.11 Private renting is becoming increasing common and the share of grants going to
this sector is inevitably going to continue to rise, particularly for younger age
groups. However, one in four privately rented dwellings do not meet the Decent
Homes standard and they are more likely than other tenures to have Category 1
hazards such as excess cold or risk of falls
17
. One in three disabled private rented
sector tenants feels that their home does not meet their needs, which is higher
than any other tenure (Figure 4.6)
18
.
4.12 There are now almost as many disabled households in the private rented sector
as renting from registered providers (Figure 4.7). Although they are worse
housed, they get a fraction of DFGs (8%) compared to registered providers
(34%).
Figure 4.6 Unsuitable accommodation by tenure 2014-15
Source: MHCLG (2016) English Housing Survey, Table 1.3
16
Mackintosh S. and Leather P. (2016) ibid.
17
Department of Communities and Local Government (Mar 2018) English Housing survey: Headline
Report 2015/16, London: DCLG. https://www.gov.uk/government/statistics/english-housing-survey-
2015-to-2016-headline-report.
18
Department of Communities and Local Government (2016a) English Housing survey: 2014 to 15,
Adaptations and accessibility of homes report, ibid.
31
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
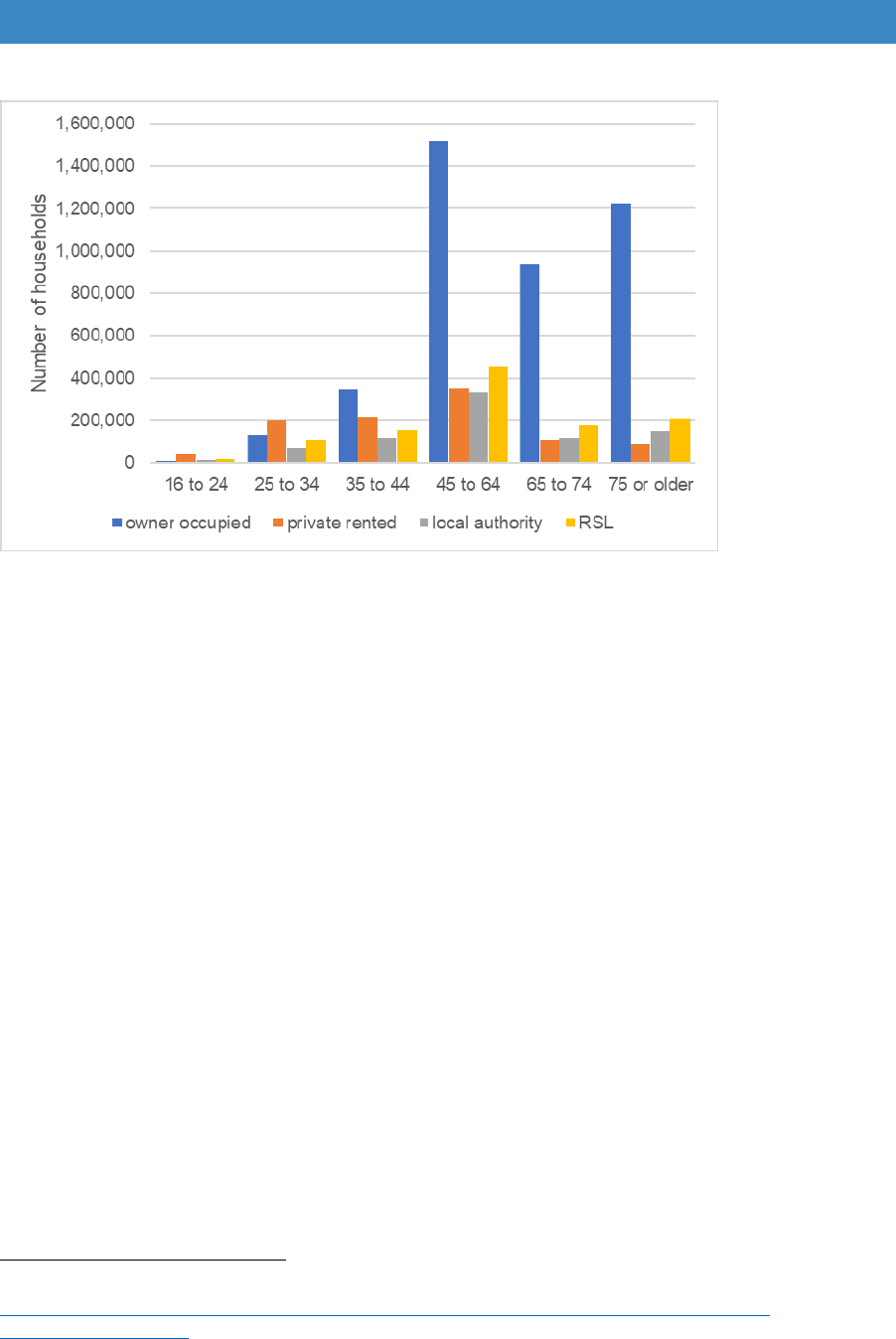
Figure 4.7 Number of households with long-term limiting illness by age and tenure
Source: English Housing Survey 2014-15, full household sample
4.13 Most households with long-term limiting illness are of working age. Increasingly
they are in private rented homes as it becomes harder to get into social housing
or on to the home ownership ladder. The focus of government policy is on getting
as many disabled people as possible into work, but this is difficult if the home is
not accessible, lacks level access to the street outside, or does not facilitate
home working.
4.14 There are now more children in the private rented sector than in social housing
19
.
Households with dependent children rose from 30% of all privately renting
households in 2005-06 to 36% in 2015-16 and half a million (510,000) children
live in privately rented homes that are unsafe. Research has shown that disabled
children tend to be the worst housed of any age group
20
. They also tend to spend
a lot of time at home and are often very isolated, meaning the accessibility and
quality of the home assumes even greater importance
21
.
4.15 Despite the rise of families in the tenure, the private rental sector remains an
insecure place to live
22
. A third (34%) of private renters have lived in their current
home for less than a year, and two thirds for less than three years (67%).
4.16 Until recently, the number of older people in the private rented sector was low. In
2014-15, households over 65 made up just 8.5 per cent (360,000) of all those
19
Parker, I. and Isaksen, M. (2017) A state of disrepair: Why renters deserve a better deal.
https://www.citizensadvice.org.uk/Global/CitizensAdvice/Housing%20Publications/PRS-
AStateofDisrepair.pdf.
20
Beresford, B. and Rhodes, D. (2008) Housing and disabled children, York: Joseph Rowntree
Foundation.
21
Contact a Family (2011) Forgotten Families: The impact of isolation on families with disabled
children across the UK, London: Contact a Family.
22
Parker and Isaksen (2017) ibid.
32
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
renting privately
23
. However, there is a diversity of supply and tenancy
arrangements, with some older tenants living in very poor conditions
24
. Numbers
of older people in this sector will begin to increase in the 2020s as higher
proportions are in the cohorts approaching retirement age (Figure 4.7 above). A
survey in 2016 for Citizens Advice revealed that 40% of people aged 55-64 and
34% of those over 65 renting privately have a tenancy that lasts six months or
less
25
. As numbers in this tenure increase, for a significant proportion, it may
become difficult to age in place successfully.
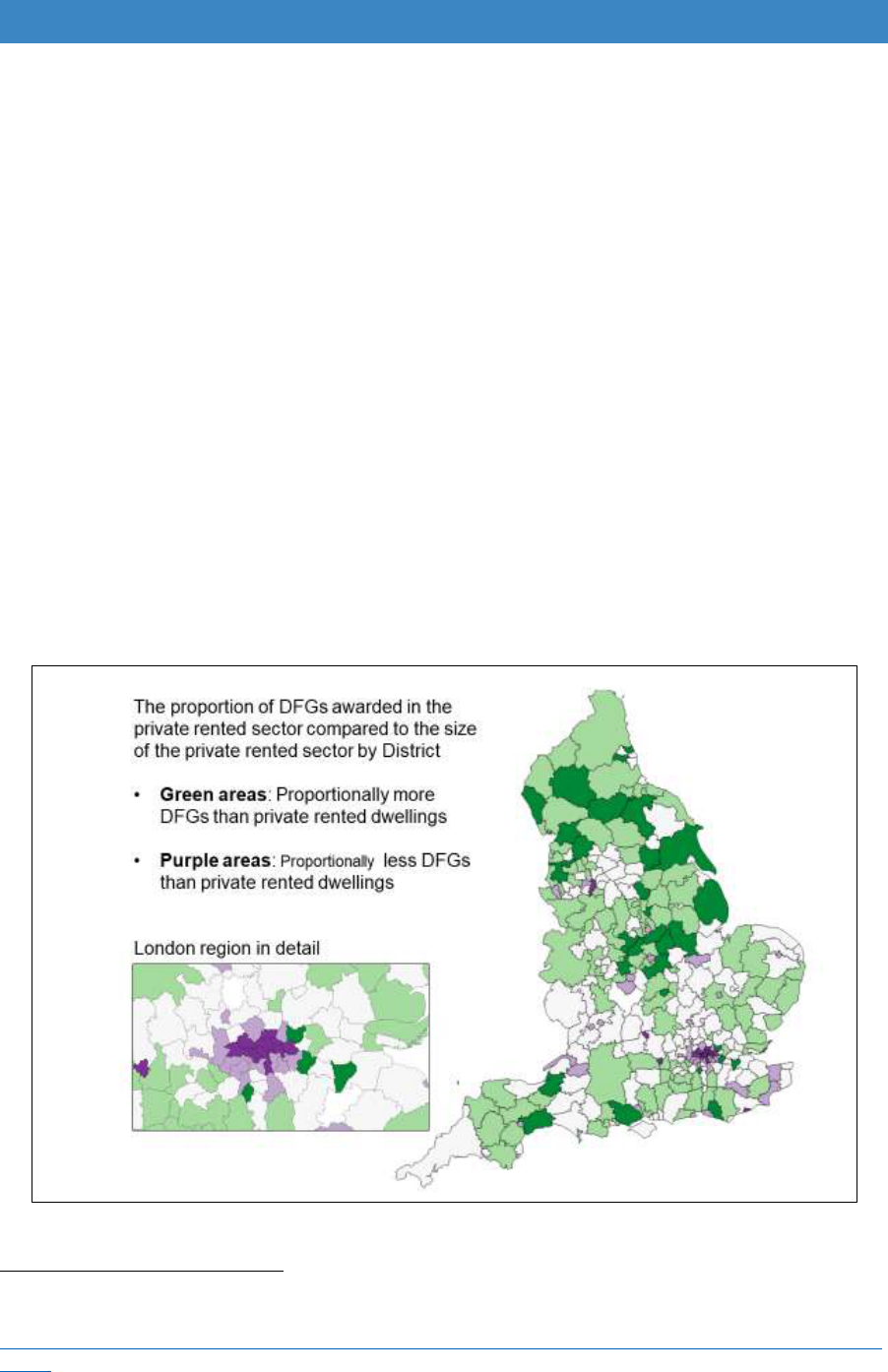
4.17 There are problems delivering the DFG in this tenure. Grants are difficult to
approve if the home is in poor condition, but in many areas of the country
alternative accommodation is not easy to find at a price people can afford. Short-
term tenancies also have a major effect on DFG approvals as residents are
supposed to show they plan to remain for at least five years. In addition, landlords
may not always give permission for the necessary changes to the property. Parts
of the country with high proportions of private renting, such as central London,
appear to be getting fewer grants than might be expected, probably because of
these reasons (Figure 4.8).
Figure 4.8 Distribution of DFGs in the private rented sector
Source: LOGASnet
23
Ministry of Housing, Communities and Local Government (2016c) English Housing Survey 2014 to
2015: Private Rented Sector report, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-private-rented-sector-
report.
24
Rugg, J. and Croucher, K. (2010) Older People’s Experiences of Renting Privately, London: Age
Concern and Help the Aged.
25
Parker and Isaksen (2017) ibid.
33

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Council stock
4.18 The main DFG budget cannot be used to fund adaptations to local authority
properties
26
. Council landlords are expected to use their own resources from the
local authority Housing Revenue Account (HRA). Additional funding was
included for disabled adaptations in self-financing determinations from 2012
27
.
Compared to registered providers, council tenants tend to be older, and the stock
was built at an earlier date.
4.19 How funding levels and delivery processes differ using the HRA relative to the
DFG is outside the remit of this review. However, if more stock is transferred and
becomes eligible for the DFG, account will need to be taken of this in the national
allocation of resources. A FOI in 2017 to 176 authorities with more than 100 units
of retained stock was returned by 76% of authorities (80% of those with
significant amounts of stock). This showed that the majority were using the HRA
(91%). Those that were not using the HRA were all Arms-Length Management
Organisations (ALMOs). It is hoped that they have their own budgets for
adaptations, but some may be using the DFG.
4.20 Whichever funding source is used to access assistance with home adaptations
(DFG or HRA), it should be tenure neutral with all applicants given equal access
to funding. In some areas, local adaptation teams handle council stock
modifications alongside DFG work, making it easier to apply to apply the same
standards.
Rural housing
4.21 The rural population is ageing faster than in urban areas. In the next 20 years it
is estimated that half of rural households will be aged over 65. There are already
more 75- year olds in rural than in urban areas
28
. There are higher levels of home
ownership with around 80% of older people owner occupiers. However, homes
in rural areas are less likely to be adapted
29
. People are less likely to move as
they want to stay in their communities where rehousing options may be more
limited. Delivering adaptation services to more scattered and isolated
populations is costlier and will need to be adequately resourced.
26
Department for Communities and Local Government (2008) Disabled Facilities Grant – The
Package of Changes to Modernise the Programme, London: DCLG.
27
Wilson, W. and Fears, C. (Dec 2016) ibid p. 27.
28
Porteus, J. (Apr 2018) Rural Housing for an Ageing Population: Preserving Independence, The
Rural HAPPI Inquiry, HAPPI 4.
https://www.housinglin.org.uk/Topics/type/Rural-Housing-for-an-Ageing-Population-Preserving-
Independence-HAPPI-4/.
29
Connors, C., Kenrick, M. and Bloch, A. (2013) Rural Ageing Research: Summary Report of
Findings, London: DEFRA.
34

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Who is excluded from the DFG?
4.22 It is important to look at who drops out of the grant process and why this happens.
If specific groups are being excluded, it may reflect issues to do with assessment
process, difficulties in dealing with landlords as discussed above, or the way the
means test operates. Any issues identified will need to be addressed in the
review. Unfortunately, it is hard to get exact figures as there are several stages
when people may drop out:
a) Before reaching the local authority or home improvement agency – There
may be people looking for help who never locate it. In most areas the DFG is
not advertised and it is hard to find information on most local authority websites.
Telephone systems are confusing with numerous push button options.
b) At the social care help desk – It is impossible to know who might have been
eligible for a DFG who drops out at this stage. Local authorities with significant
pressures on social care budgets may exclude people, sometimes
inadvertently, as eligibility for social care differs from that for the DFG.
c) At the assessment stage (usually in social care) – some people may be given
equipment or minor adaptations, others may have a preliminary means test and
realise they would not be eligible for a DFG. Others may decide they do not
wish to proceed further with local authority help. There is no source of data for
who might have been eligible for a DFG who drops out at this stage.
d) At the referral stage – when the assessment has been completed and the
case referred, but it does not proceed to grant application. This is the first point
in the process when those who might be eligible for a DFG are recorded
reasonably consistently. The reasons for exclusion at this stage were explored
using a Freedom of Information request (FOI) with the following question: For
Disabled Facilities Grant referrals received from social care between 1 April
2016 and 31 March 2017, how many did not proceed to full application? The
FOI also asked for a breakdown by age, tenure and a pre-coded list of reasons.
4.23 The results of the FOI show that, on average, two thirds of grants proceed and a
third are closed at the referral stage, but there is a lot of variation (Figure 4.9). In
a few places, only a very small proportion proceed, while in others almost all go
to full application. This may be because some places do a preliminary means
test earlier in the process to screen out people who would be ineligible. Why
other authorities have such high closure rates is less clear.
35
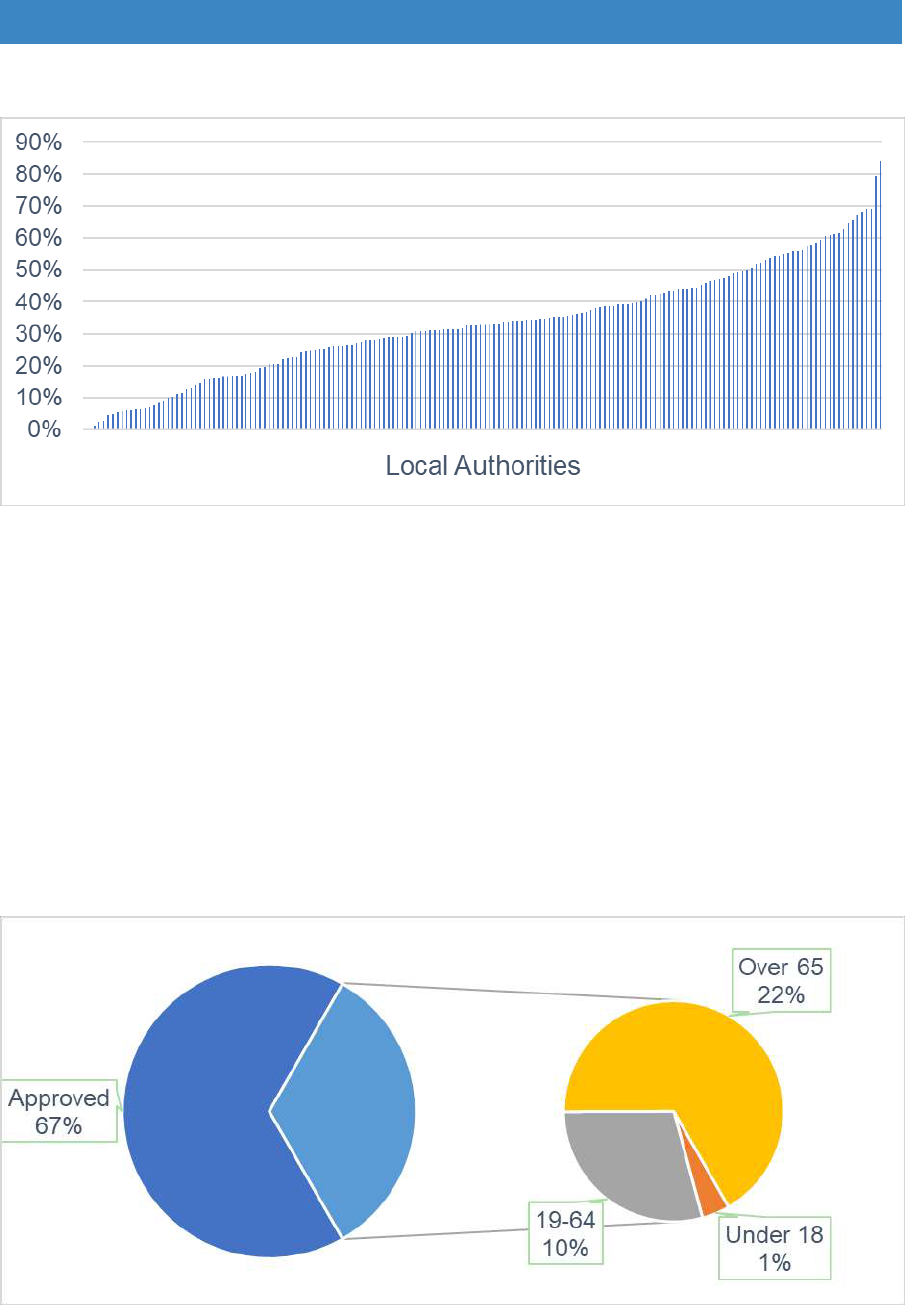
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 4.9 Referrals that do not proceed to full application by local authority
Source: Foundations FOI 2018
4.24 Looking at overall averages, of the third that do not proceed, the drop out by age
is similar to the proportion proceeding with their application (Figure 4.10). Slightly
fewer children’s cases drop out, perhaps because they are not means tested.
However, there are some substantial differences at regional level (Table 4.1). In
the West Midlands more children’s cases fail to proceed compared to other
areas, whereas in London more people of working age drop out.
Figure 4.10 Closed referrals by age 2016/17
Source: Foundations FOI 2017
36
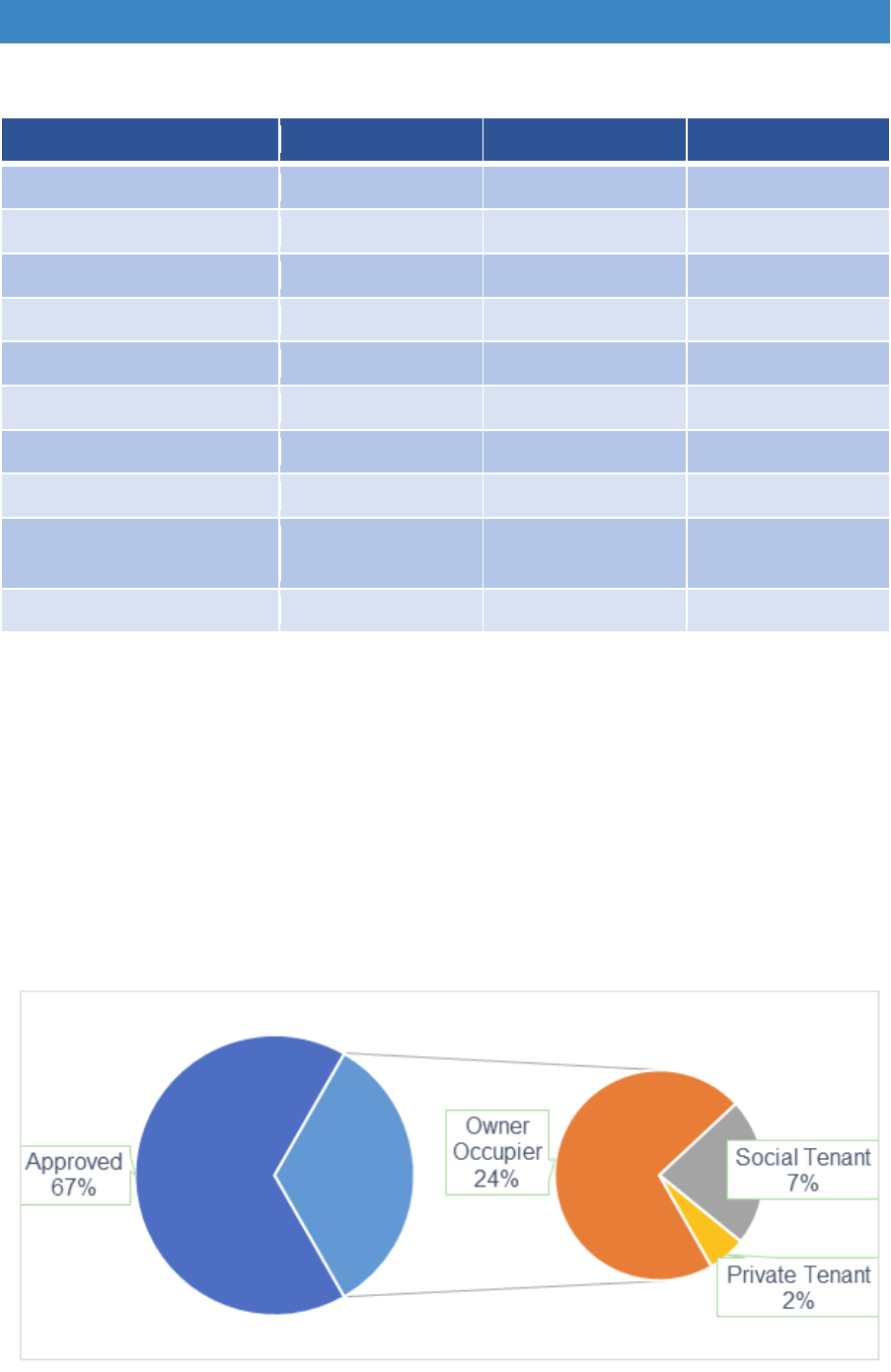
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Table 4.1 Regional differences in percentage of referrals closed by age 2016/17
Region
Under 19
19 64
Over 65
East Midlands
3%
30%
67%
East of England
3%
24%
73%
London
2%
40%
58%
North East
3%
30%
66%
North West
3%
28%
69%
South East
5%
27%
68%
South West
4%
31%
65%
West Midlands
11%
31%
58%
Yorkshire and The
Humber
3%
26%
70%
ENGLAND
4%
29%
67%
-
Source: Foundations FOI 2017
4.25 Overall, fewer owners seem to go ahead than tenants, particularly compared to
those from the social rented sector, presumably because more owners are
deemed able to contribute (Figure 4.11 and 4.12). But again, there are regional
differences. In the South West and North East more tenants drop out, while more
owners go ahead. Conversely, in the East of England and East Midlands more
owners are excluded (Table 4.2).
Figure 4.11 Closed referrals by tenure 2016/17
Source: Foundations FOI 2017
37
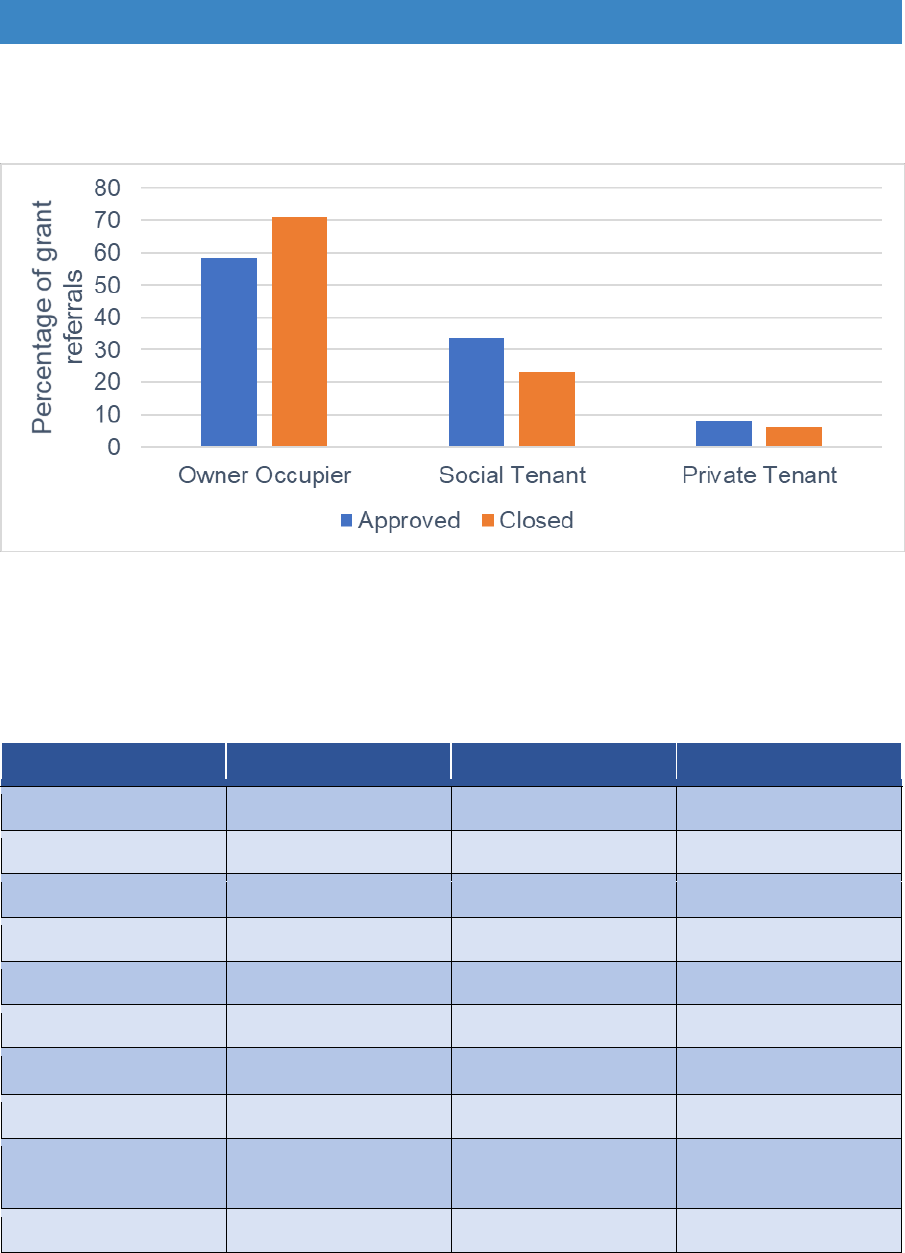
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 4.12 Approved and closed referrals by tenure 2016/17
Source: Foundations FOI 2018
Table 4.2 Regional differences in percentage referrals closed by tenure 2016/17
Region
Owner Occupier
Social Tenant
Private Tenant
East Midlands
79%
15%
6%
4%
4%
5%
7%
6%
9%
4%
5%
6%
East of England
77%
19%
London
66%
30%
North East
61%
33%
North West
72%
22%
South East
71%
23%
South West
63%
28%
West Midlands
76%
20%
Yorkshire and The
Humber
73%
21%
ENGLAND
71%
23%
Source: Foundations FOI 2017
38
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Reasons for exclusion
4.26 Reasons for exclusion are hard to identify, as so many fall into the categories
‘other’ or ‘insufficient information’. Many local authorities do not know, or do not
record, the reason why applicants do not proceed. This is of concern, as so many
seem to drop out in some areas. However, key points stand out about excluded
cases. There appear to be very few dropping out because the work costs over
£30,000 or because the work wasn’t reasonable or practicable given the state of
the home. Only a limited number decide to move rather than adapt the home.
Unfortunately, a small number die before they get the grant.
4.27 The biggest identifiable category, about a quarter of those who drop out, do so
because they have to make a contribution to the costs. It explains why more
owners drop out than tenants, as mortgage costs are not taken into account in
the means test. There is some regional variation, with drop-out due to
contributions appearing to be highest in the North East and Yorkshire/The
Humber and lowest in the South West (Table 4.3).
Table 4.3 Regional differences in percentage closed by reason 2016/17
Region
Contribution
Over
£30k
Not
reasbl/
pract
No Info
Moved
Died
Other
East Midlands
26%
0%
2%
18%
6%
9%
40%
East of England
24%
0%
2%
15%
6%
8%
45%
London
21%
0%
2%
15%
9%
13%
40%
North East
30%
0%
2%
7%
12%
11%
39%
North West
21%
2%
2%
20%
7%
11%
36%
South East
28%
1%
3%
13%
8%
8%
39%
South West
19%
0%
4%
4%
6%
7%
59%
West Midlands
28%
1%
1%
10%
6%
10%
44%
Yorkshire and
The Humber
30%
0%
1%
10%
7%
9%
44%
ENGLAND
24%
1%
2%
14%
7%
9%
42%
Source: Foundations FOI 2017
4.28 More detail about the reasons people drop out comes from other sources. Pooled
outcome data from one county authority adds weight to the findings from the
national FOI. The most important reason for people failing to proceed is because
their assessed contribution was more than the cost of work (almost a quarter of
39
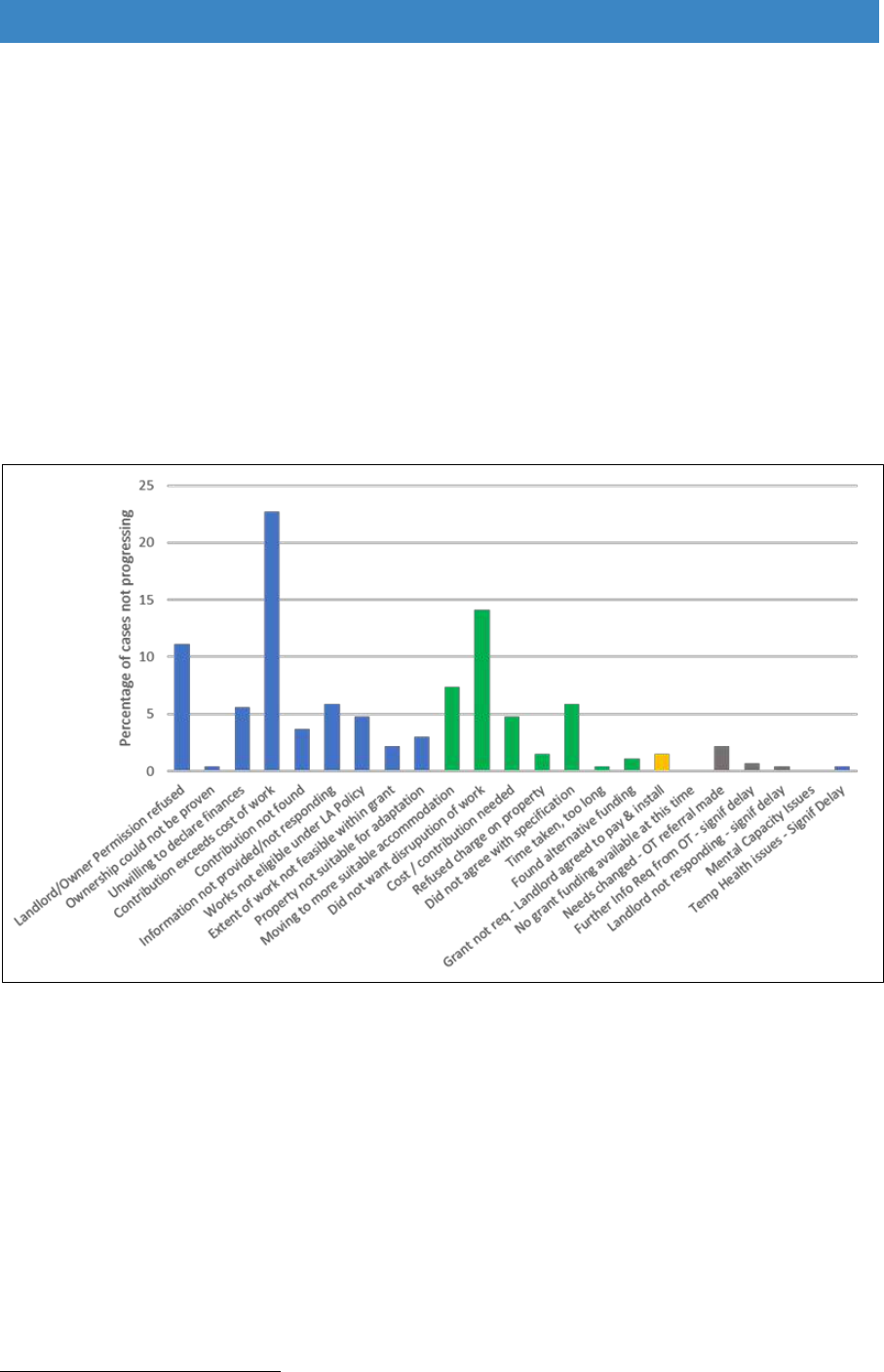
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
those dropping out) (Figure 4.4). The operation of the means test, and how this
might exclude certain types of people, is explored further in Section B.
4.29 These local data also revealed that almost 15% dropped out because they did
not want the disruption of work. Over 10% did not proceed because the landlord
or owner refused permission, reflecting some of the concerns about the private
rented sector outlined above. Data from the English Survey also shows that
adaptations for private rented sector tenants needing adaptations are refused in
30
10% of cases .
Figure 4.4 Cases that did not proceed by reason in one county authority 2017/18
Source: outcome data provided to the review by a county authority in April 2018
4.30 Authorities do not normally follow up on closed cases to find out what happens
to them afterwards. There is no way of knowing how many closed cases proceed
with work themselves or how many take no action and remain living in homes
that are un-adapted and potentially inaccessible or unsafe. How more people
might be helped using statutory funding and how to provide help for people
outside the DFG is discussed further in Section B.
4.31 Evidence about numbers who proceed or drop out according to ethnic origin is
limited. Any information collected locally is not aggregated at national level.
30
Ministry of Housing, Communities and Local Government (2016a) English housing survey 2014 to
2015 Adaptations and accessibility of homes report, ibid.
40

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
There is evidence of higher levels of limiting long-term illness in BAME groups
than in the White British population
31
. One academic paper analysed English
Housing Survey data to show that non-white households had fewer adaptations
than were needed and they were twice as likely as white households to have no
adaptations at all
32
. They may be less aware of what services are available.
Cultural differences may mean that home adaptations need to be implemented
in a much more personalised way to take account of ways of sleeping, washing,
bathing and preparing food or maintaining space in the home for religious
observance or for extended family to meet. There may be a lot of good practice
in different local authorities, but further research is required to evaluate and
disseminate this information.
Summary - who gets the DFG and who is excluded
Overall there are more disabled people of working age than in any other age
group, but the percentage of people with impairments rises significantly in later
life. The proportion of people in younger age groups receiving the DFG has
been rising, reflecting the increase in disabled people under retirement age.
Older people remain the group most likely to obtain a DFG and this is likely to
rise in the 2020s due to a bulge in the population of people with impairments
getting to retirement age.
The distribution of grants by tenure is dominated by owner occupiers as most
older people are home owners.
Registered providers continue to make significant use of the DFG. Registered
provider tenants have an advantage as they are clearly signposted to the DFG
while the grant remains hidden to most owners and private tenants.
The council stock remains outside the DFG, which does not help with strategic
planning of accessible homes for disabled and older people.
Private tenants are in a weak position, but private tenants will need more grants
as numbers in this tenure are increasing. They currently get far fewer grants
than registered provider tenants. Disabled children in this sector are a particular
concern.
Rural areas may need more resources due to their rapidly ageing populations
and the added cost of providing services to more scattered populations.
31
Bécaresyet, L. (2013) Dynamics of Diversity: Evidence from the 2011 Census, Manchester: Centre
on Dynamics of Ethnicity
32
Ewart, I. and Harty, C. (2015) Provision of Disability Adaptations to the Home: Analysis of
Household Survey Data, Housing Studies, 30:6, 901-923, DOI: 10.1080/02673037.2014.991379.
41

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
There is little information on use of the DFG by people from BAME groups and
whether they have different needs. This needs more research.
The high number of people who drop out of the DFG process in some
authorities is a cause of concern.
The biggest reason why people drop out is due to the need to contribute to
costs. This will be addressed later in this report in the review of the means test
to ensure that the test is a fair as possible.
What happens to people who drop out of the DFG process needs to be recorded
more consistently, and people should be signposted to appropriate advice,
information and support services.
42
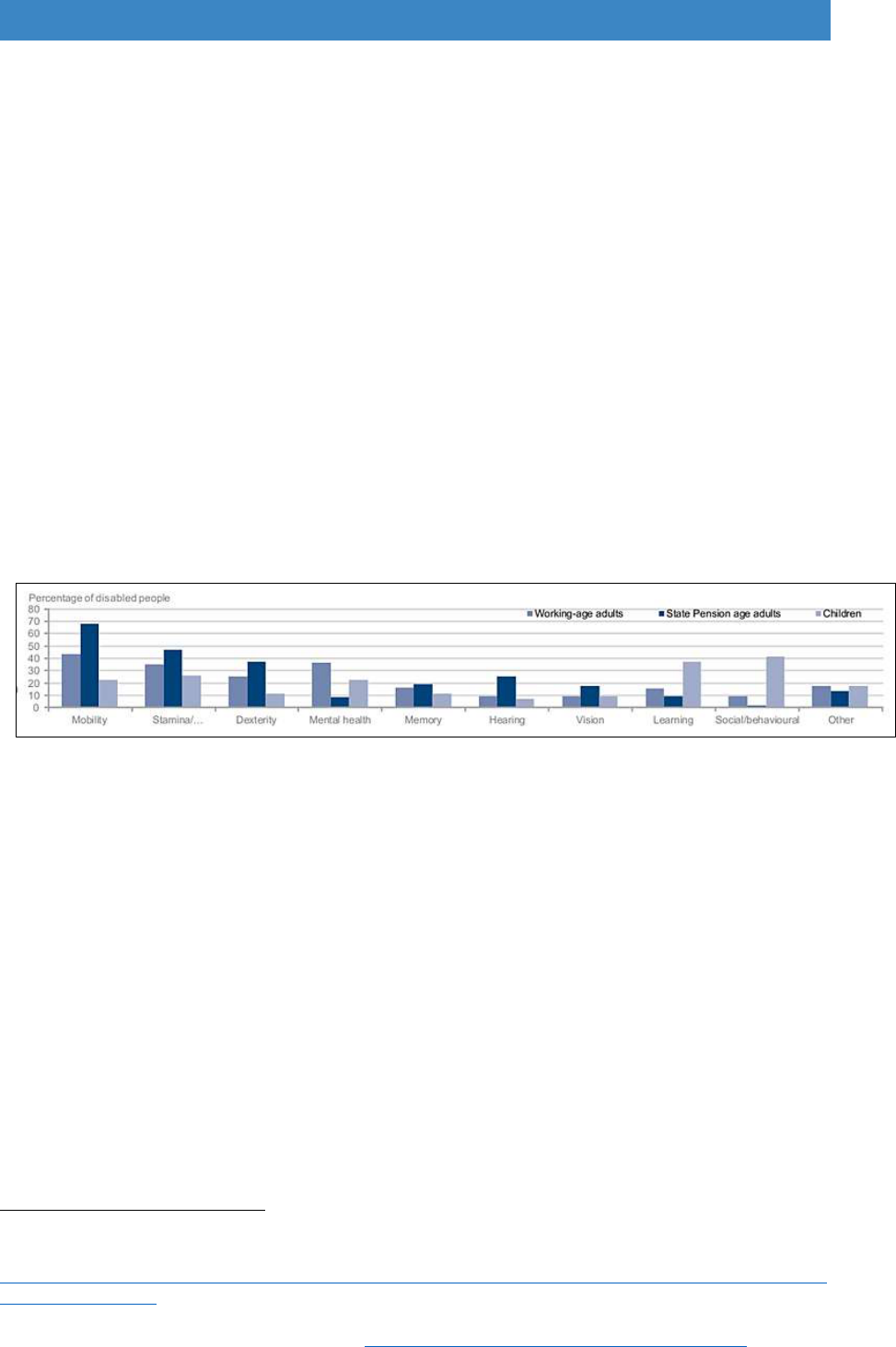
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 5. Types of adaptations and costs
Types of impairment
5.1 Prior to looking at the categories of work funded by the DFG, it is useful to look
at the types of impairment in different age groups and at how this is changing.
5.2 The types of impairment people are likely to experience vary by age. Mobility,
stamina and dexterity difficulties are the most common impairments in older and
working age adults. Learning difficulties and social/behavioural impairments are
more prevalent in children (Figure 5.1). Sensory impairment and memory
problems tend to increase with age. Mental health conditions are increasing in
people of working age, although long-term mental health issues, such as
depression, are known to be under-recorded in older age groups
33
.
Figure 5.1 Main types of disability by age
Source: Department of Work and Pensions (Mar 2018) Family Resources Survey 2016/17
5.3 Research shows that multiple conditions are also becoming more common,
particularly among women and people with low income, but that they are also
increasing in younger age groups. Those with multiple health problems are more
likely to be disabled. This research also shows that chronic physical conditions
are often found alongside mental health problems, particularly depression
34
.
Memory problems, particularly dementia, are also increasing. Most people
affected by these conditions remain living in their own homes and may need
specific types of adaptations.
5.4 Discussions with local authority staff and written submissions to the review
support the fact that the medical conditions DFG staff are dealing with are
becoming more complex. Due to austerity measures, social care services may
only be referring people with urgent, critical or substantial needs. The increased
33
Age UK (Oct 2016) Hidden in plain sight: The unmet mental health needs of older people, London:
Age UK.
https://www.ageuk.org.uk/brandpartnerglobal/wiganboroughvpp/hidden_in_plain_sight_older_peoples
_mental_health.pdf.
34
The Academy of Medical Sciences (Apr 2018) Multimorbidity: a priority for global health research,
London: The Academy of Medical Sciences. https://acmedsci.ac.uk/file-download/99630838.
43

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
complexity of cases may be a further reason why the average cost of work is
increasing. Staff may need additional training to deal with complex cases and
people with mental health issues. Cases may also take longer to process.
5.5 There is a strong relationship between low income, poor health, fewer impairment
free-life-years, and lower life expectancy (Marmot, 2015)
35
. There is also
evidence that frailty (loss of muscle strength, falls and confusion) occurs almost
10 years earlier in people that are in the lowest third in terms of wealth (Micra,
2017)
36
. In areas with high proportions of people on low incomes, people in their
60s may be experiencing health conditions that normally only appear in people
when they reach their 70s or even later. This may need to be better reflected in
the national allocation of resources. Frailty is an issue that health services are
very concerned about. An optimal pathway has been developed to try to ensure
that people with frailty are supported to remain living independently; adaptations
could play a much bigger role in this process
37
.
5.6 At local level, health and social care managers do not routinely work with DFG
teams to develop preventative strategies to adapt and improve homes before
people reach crisis point. Many home improvement agencies and DFG teams
have tried to link up with hospital discharge teams, GP surgeries, community
matrons, and care navigators to identify people needing help. There has been
some success, which will be discussed in Part B, but the referral pathways could
be improved.
Impairment of DFG recipients
5.7 The only information about types of impairment of DFG recipients at national level
comes from a FOI in 2017 (Figure 5.2). This gives a snapshot at one point in time
and does not provide much detail. It shows that most grant recipients had physical
disabilities as their primary impairment, and only 11% were recorded as having
another principal impairment. Of that ‘other’ group, dementia, sensory
impairment, and learning disability were the main issues identified. The number
of grant recipients who had multiple conditions and mental health issues was not
recorded.
35
Marmot, M. (2015) The Health Gap, London: Bloomsbury.
36
MICRA (2017) The Golden Generation: Wellbeing and Inequalities in Later Life, Manchester:
University of Manchester Institute for Collaborative Research on Ageing.
http://hummedia.manchester.ac.uk/institutes/micra/reports/golden-generation-report-2017.pdf
37
NHS England (2016) The variation between standard and optimal pathways - Janet’s story: Frailty,
RightCare scenario. https://www.england.nhs.uk/rightcare/wp-content/uploads/sites/40/2016/08/janet-
story-narr.pdf.
44
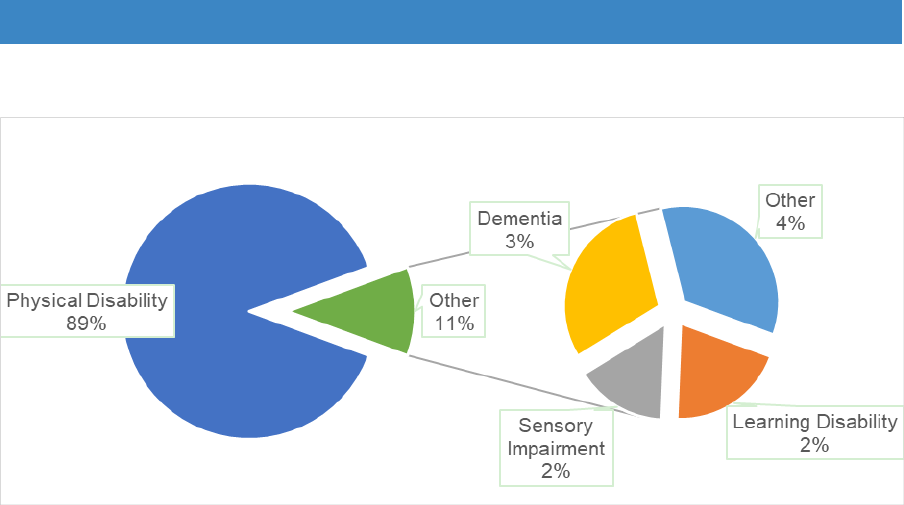
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 5.2 Primary impairment of DFG recipients
Source: FOI 2017
Type of work allowed
5.8 The types of adaptations that the mandatory DFG can cover includes:
a) Making it easier to get into and out of the dwelling by, for example, widening
doors and installing ramps;
b) Ensuring the safety of the disabled person and other occupants by, for
example, providing a specially adapted room in which it would be safe to leave
a disabled person unattended, or improved lighting to ensure better visibility;
c) Making access to the living room easier;
d) Providing or improving access to the bedroom and kitchen toilet, washbasin
and bath (and/or shower) facilities; for example, by installing a stairlift or
providing a downstairs bathroom;
e) Improving or providing a heating system in the home suitable to the needs of
the disabled person;
f) Adapting heating or lighting controls to make them easier to use;
g) Improving access and movement around the home to enable the disabled
person to care for another person who lives in the property, such as a spouse,
child or another person for whom the disabled person cares;
h) Facilitating access to and from a garden for a disabled occupant or making
access to a garden safe for a disabled occupant.
5.9 The items on the list focus on physical impairment and mobility, which reflects the
view of disability in 1989, when the grant was first introduced. In the original
legislation, there was little about dementia, mental health, learning difficulties or
the needs of children with autism spectrum disorder or social/behavioural
conditions. Regulation, orders and guidance have introduced more flexibility,
particularly the 2002 RRO and the updates in 2008, but this may need to be made
clearer. As the 2005 review pointed out:
45
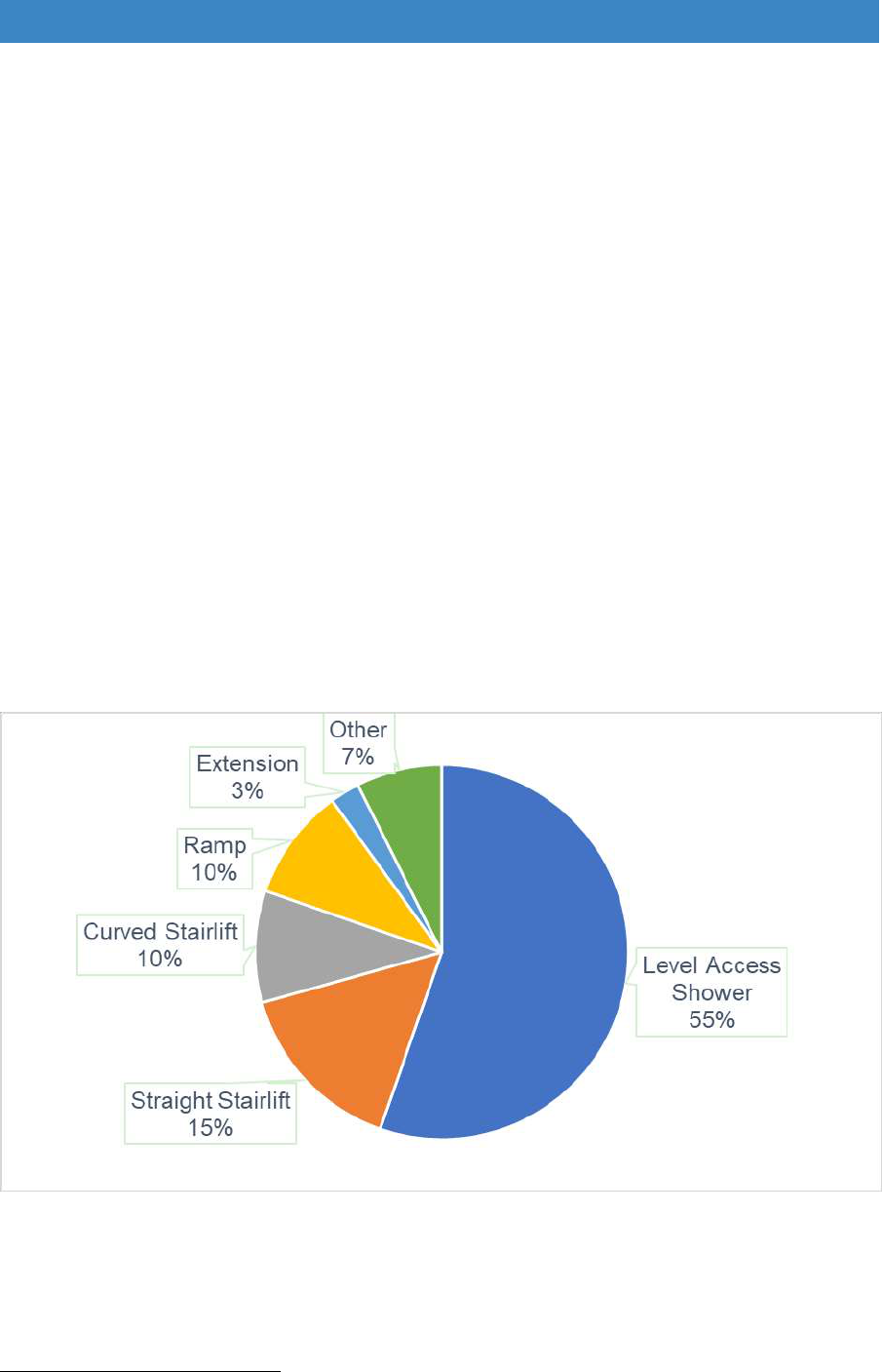
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
“The needs of disabled children and their siblings or other family
members, or of people with seriously challenging behaviour, are not
covered with unequivocal clarity in the provisions of the mandatory
DFG”
38
.
Type of work carried out
5.10 Figure 5.3 shows that the most common DFG adaptation is a level-access
shower (55%). Stairlifts (either straight or curved) make up a quarter of
applications approved and ramps 10%. Bedroom and bathroom extensions, the
most expensive adaptations for people with more severe impairments, only
comprise 3% of approvals. Often a DFG includes smaller adaptations in addition
to a shower or stairlift, such as grabrails, heating or lighting improvements, but
these are not shown in the figures. Discretionary DFG grants are starting to be
used to pay for a range of other work, such as home from hospital services,
repairs, decluttering and deep cleaning, but there are no national level data at
present.
Figure 5.3 Type of DFG applications approved 2016/17
Source: Foundations FOI Jan 2018
38
Heywood et al (2005) Reviewing the Disabled Facilities Grant Programme, Bristol: School for Policy
Studies, p. 6.
46
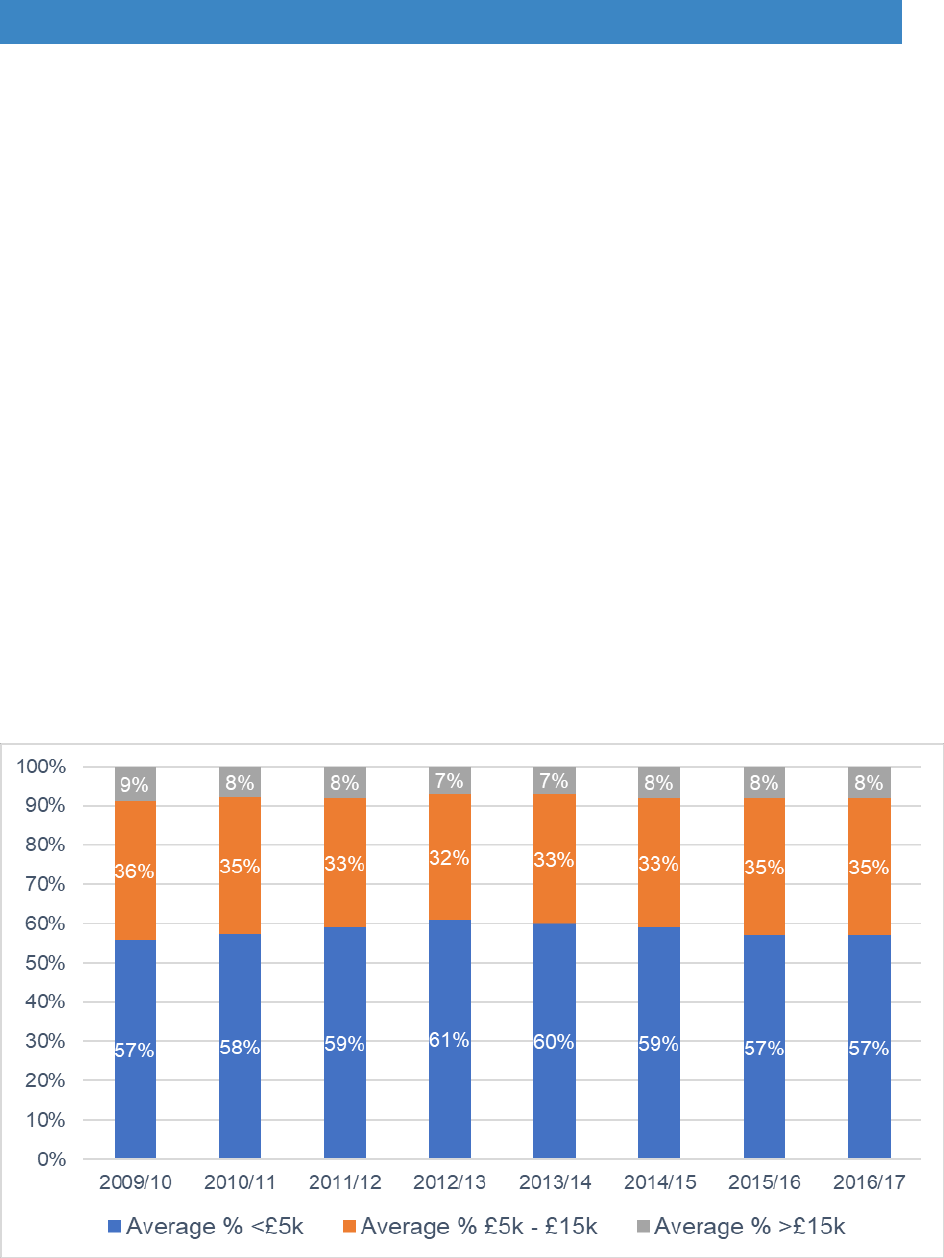
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
The cost of DFG work
5.11 Average costs reflect the type of DFG work that is most common: showers and
stairlifts. The majority of works (57% in 2015/16) cost less than £5,000, while a
further 35% were under £15,000. On average, only 8% of DFGs were over
£15,000 (Figure 5.4). The proportions by cost group have remained relatively
constant over the past eight years, although as was shown in Figure 3.4 (Chapter
3) the average cost of a grant has risen slightly from just over £7,000 in 2009/10
to nearly £9,000 in 2016/17. This might be due to a combination of two factors:
first, the increased complexity of cases, and second, specifications beginning to
take account of the rise in building costs, following the increase in overall levels
of funding.
5.12 However, there is considerable regional variation. Costs in London are
significantly higher, with only a third of work under £5,000, whereas in most other
areas between a half and two thirds is under £5,000. The North East has the
lowest costs, with three quarters of cases under £5,000 (Figure 5.5).
Figure 5.4 Trends in average value of works
Source: LOGASnet
47
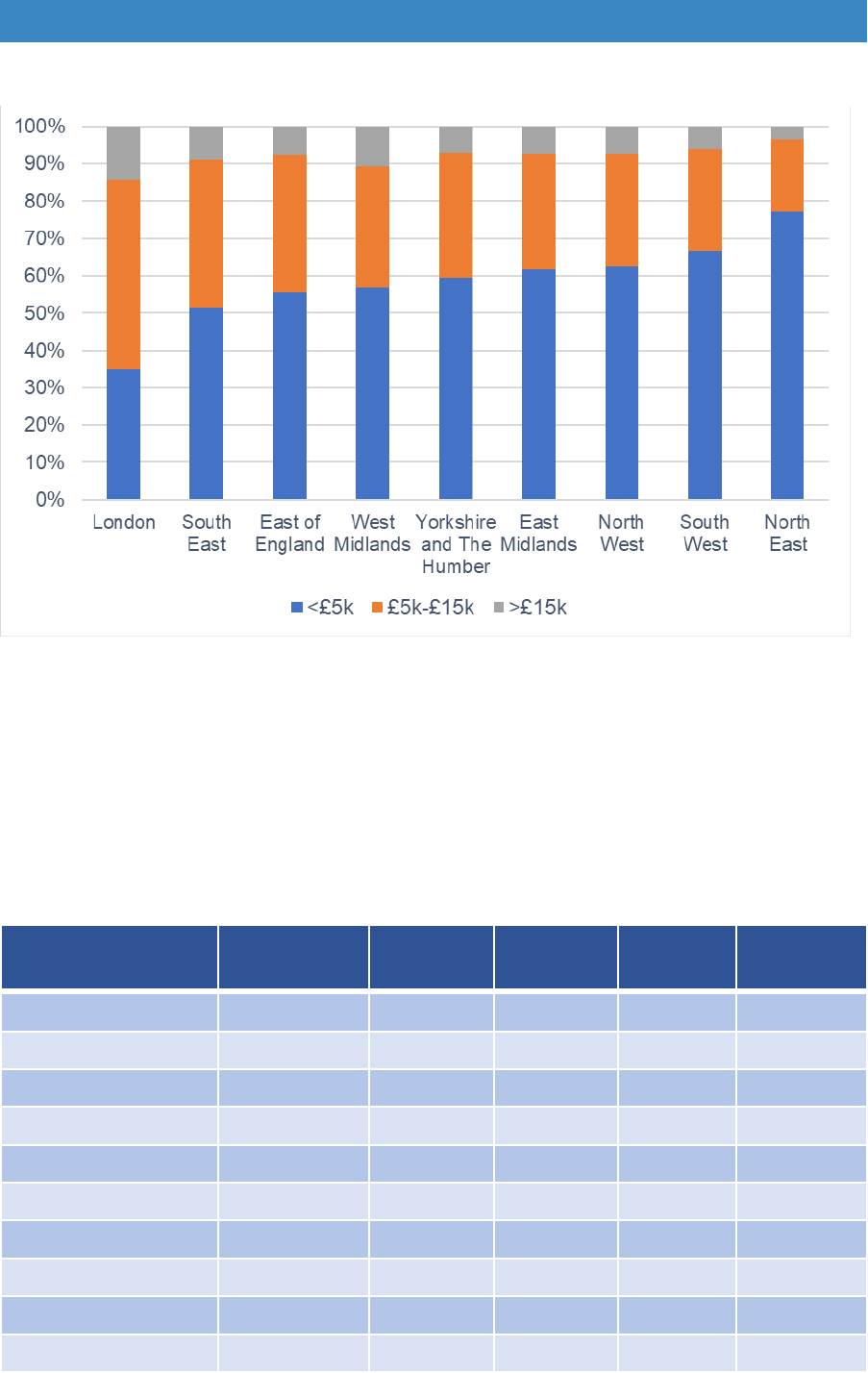
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 5.5 Average size of grant per region 2009-2017
Source: LOGASnet
5.13 Average adaptations costs by region for each of the main types of work is shown
in Table 5.1. Level access showers cost just under £5,000 on average, ranging
from £3,600 in the North East to £5,900 in London. The average stairlift cost is
around £2,400 for a straight stairlift and £4,500 for a curved stairlift. Ramps vary
more in price, partly reflecting topography as places with hills often need more
complicated ramping systems.
Table 5.1 Average adaptation cost by type of adaptation and by region 2016/17
Region
Level Access
Shower
Straight
Stairlift
Curved
Stairlift
Ramp
Extension
East Midlands
£4,601
£2,211
£4,211
£3,231
£28,269
East of England
£5,122
£2,617
£4,770
£4,421
£30,218
London
£5,911
£3,882
£5,109
£5,327
£55,243
North East
£3,617
£1,580
£3,801
£2,769
£27,667
North West
£3,967
£2,202
£4,380
£2,833
£29,362
South East
£4,979
£2,134
£4,697
£3,692
£32,870
South West
£4,290
£2,029
£4,126
£5,317
£34,642
West Midlands
£5,032
£2,635
£4,923
£4,270
£29,841
Yorks/Humberside
£4,440
£2,012
£4,267
£3,721
£30,107
ENGLAND
£4,755
£2,358
£4,495
£3,928
£31,939
Source: Foundations FOI 2018
48
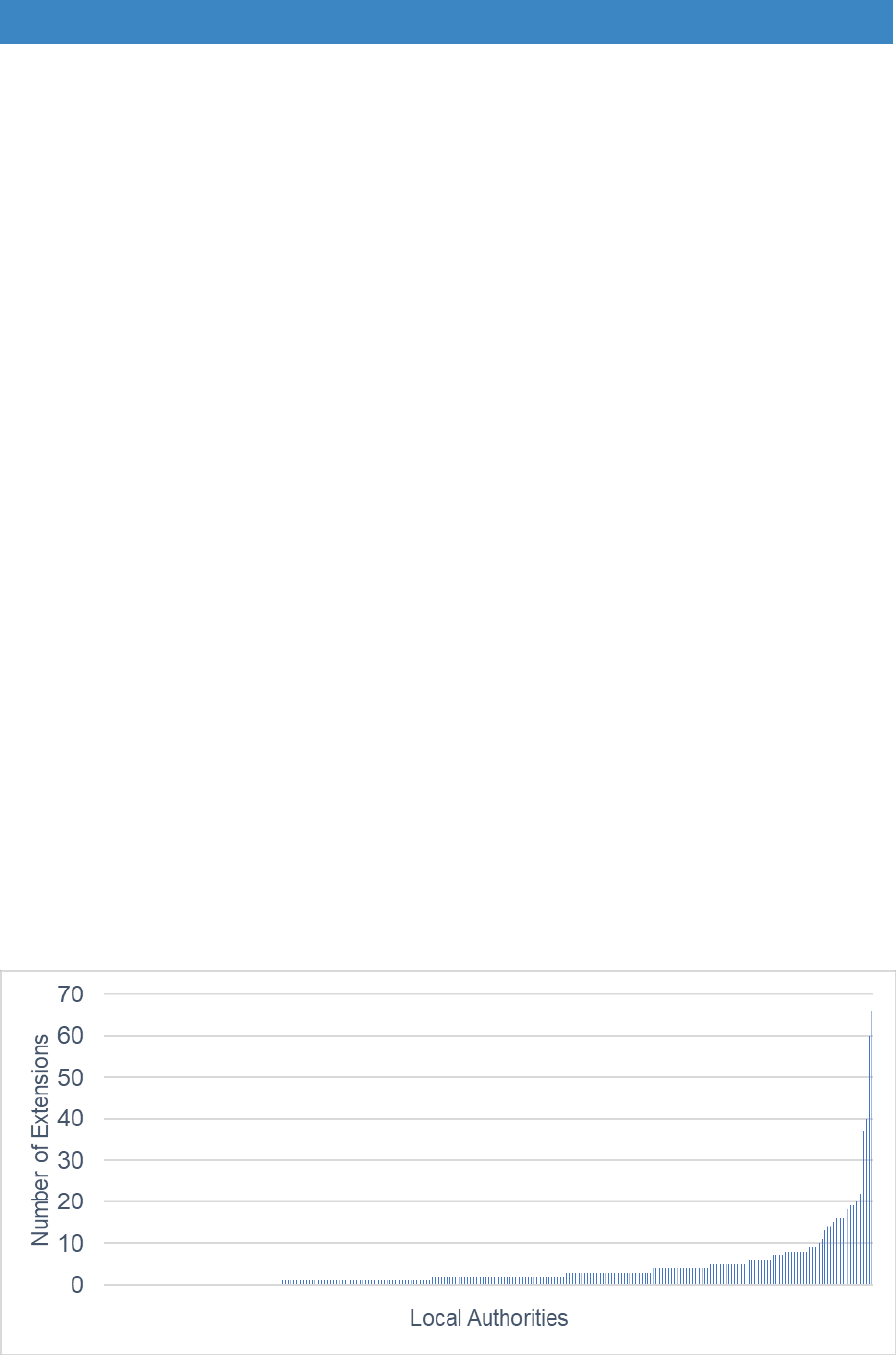
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
More expensive grants and those over the upper limit of £30,000
5.14 In all regions there are relatively few cases of works over £15,000; the figure
varies between 3% in the North East and 14% in London, with the average in
2016/17 being 8% (see Figure 5.5 above). Expensive grants are usually for more
complex cases, where people have severe impairments or limited mobility,
particularly wheelchair users. Children with learning disabilities, autism spectrum
disorder or social/behavioural problems may need additional space separate
from siblings. The work may include major reorganisation of the existing living
space and/or the building of a bedroom/bathroom extension.
5.15 The upper limit of the DFG is £30,000. It has not increased since 2008 and has
not kept pace with inflation. However, in London the average cost of an extension
is £55,000. Outside of London, build costs seem to be affected by what can be
achieved within DFG limits, as most seem to cost around £30,000 – although
costs in the South East and South West seem to be a little higher. The drive to
stay within the grant limits may affect the quality of what is achieved.
5.16 Not all authorities do extensions. Figure 5.6 shows that some do none, most only
do two a year, although at the other extreme a few do 20 or more. Small
authorities may have very few complex cases over a period of several years,
whereas some of the larger authorities may have high caseloads every year. The
average number of adaptations over £30,000 has been decreasing in parallel
with reductions in funding and does not seem to reflect changing levels of need
(Figure 5.7).
Figure 5.6 Variation in provision of extensions by authority
Source: Foundations FOI 2018
49
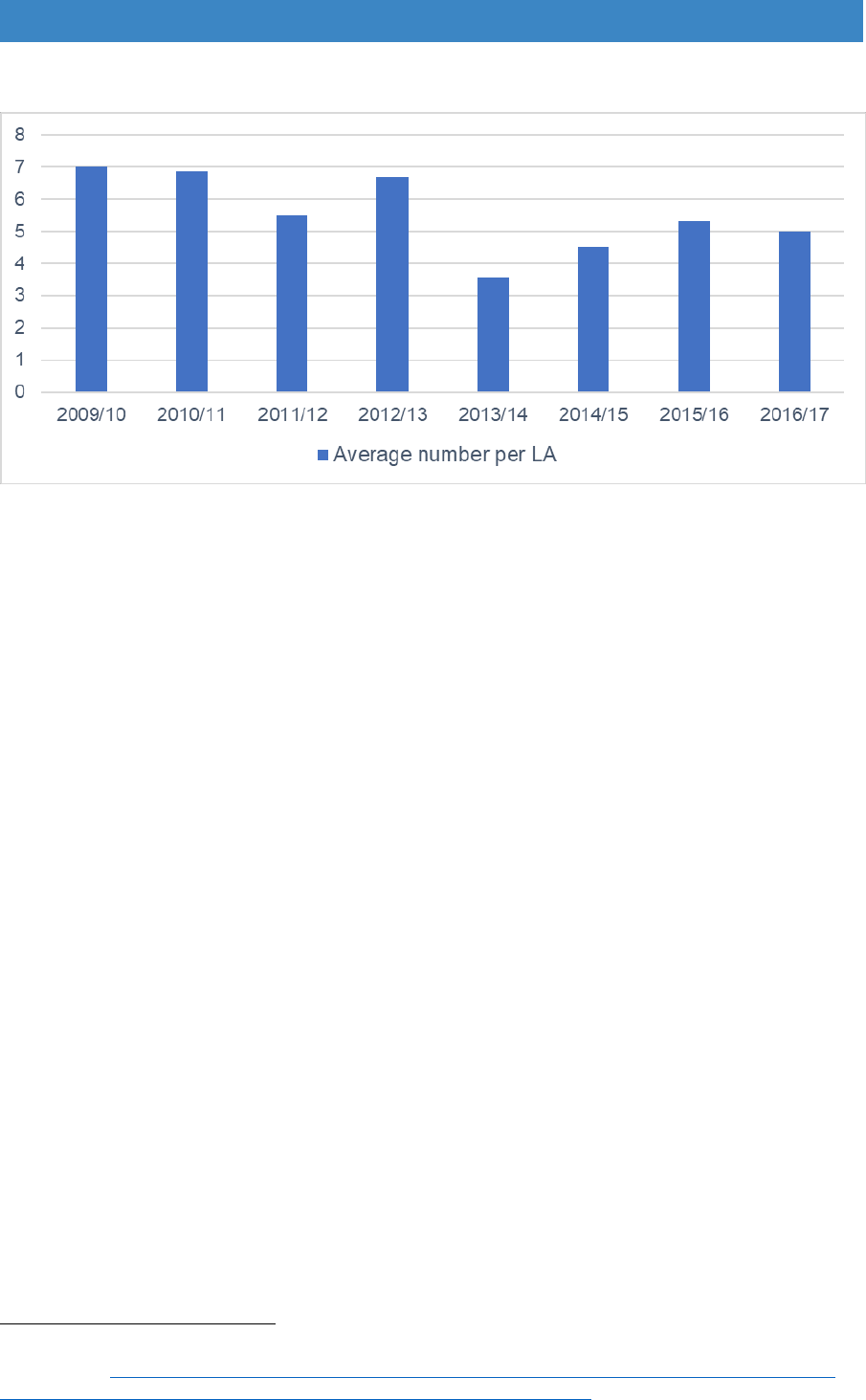
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 5.7 Trend in average number of £30,000 grants
Source: LOGASnet returns
5.17 Some authorities have specific policies not to do extensions, particularly those
with relatively small budgets – where just one or two expensive cases might use
a very high proportion of the funding available for all users. Instead, they require
additional reception rooms to be used as bedrooms, through-lifts or stairlifts to
be installed to give access to upstairs bedroom and bathrooms, or for internal
layouts to be reorganised. However, Ombudsman findings have shown that
these solutions are not always in the best interest of the grant recipient
39
. Loss
of reception rooms can be detrimental if they reduce the ability to socialise,
prevent children having quiet space for homework, or take away space used for
religious or cultural activities.
5.18 At a time when local authority finances are under serious pressure, managers
have no option but to stay within budget. Although payment for adaptations could
make enormous savings elsewhere in health or social care, in the absence of
integrated decision-making managers have little or no power to make effective,
joined-up decisions for the disabled customer, their family and carers.
Rehousing as an alternative to expensive grants
5.19 Rehousing is an alternative to adapting where a property is unfeasible or very
expensive to adapt, or where rehousing would provide a better solution and
providing the household is willing to move. People in private renting are most
keen to move, while home owners are the least keen (Figure 5.8). Almost 20%
of households under 55 were willing to move; however, desire declines with age,
with people over 75 being the least prepared to relocate.
39
Local Government Ombudsman (2016) Making a house a home: Local authorities and disabled
adaptations. https://www.lgo.org.uk/information-centre/news/2016/mar/delays-to-disabled-facilities-
grant-process-have-major-impact-on-people-s-lives-says-ombudsman.
50
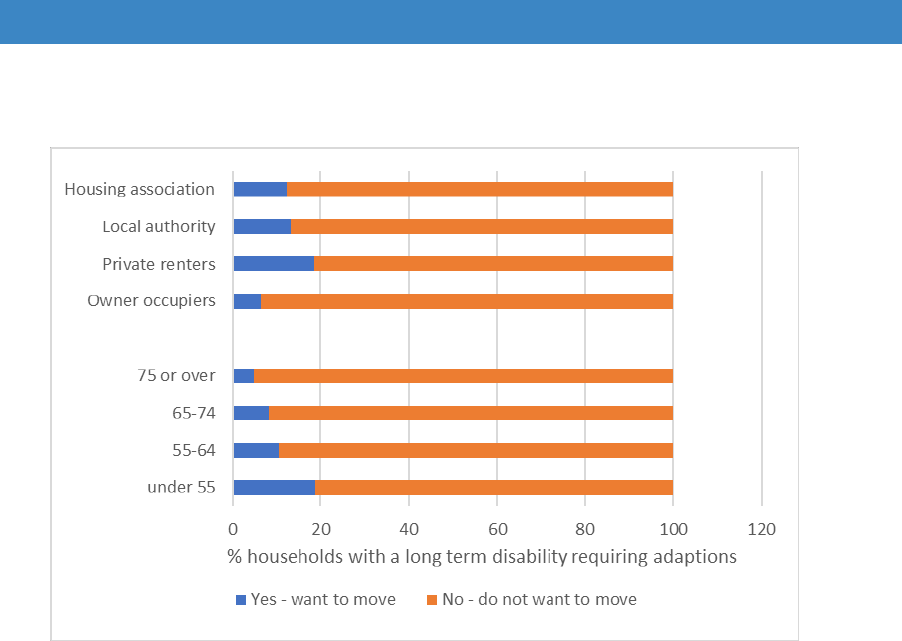
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 5.8 Households that required an adaptation wanting different
accommodation, by age and tenure, 2014-15
Source: MHCLG (2016) English House Condition Survey 2014/15
5.20 With pressures on local authority resources, many housing options services
have been discontinued. In 2015/16 only 20% of authorities provided support
for people to move rather than adapting, and only 268 individuals across the
whole country were helped to move (Foundations FOI, 2016). Given the
savings to DFG budgets, these services could pay for themselves in a relatively
short period of time, but better strategic management at local level is needed to
enable this to happen.
The Means Test
5.21 The means test is discussed in detail in Chapter 14. Only 14% of approved DFGs
required a contribution in 2016/17. The assessed contribution averaged £1,500,
which is worth £9.3m nationally. However, some people will have dropped out
before this stage, as was discussed in the previous chapter. A quarter of cases
that did not proceed dropped out because of the need for a contribution.
Contributions have also been kept down by keeping the most expensive
adaptations within the £30,000 upper limit.
5.22 A number of authorities have removed the means test for certain types of work
to speed up the delivery process. For example, Manchester and Dorset have
removed the test for grants under £5,000. With the help of additional CCG
funding, for an 18-month period Wigan removed the test for households
51
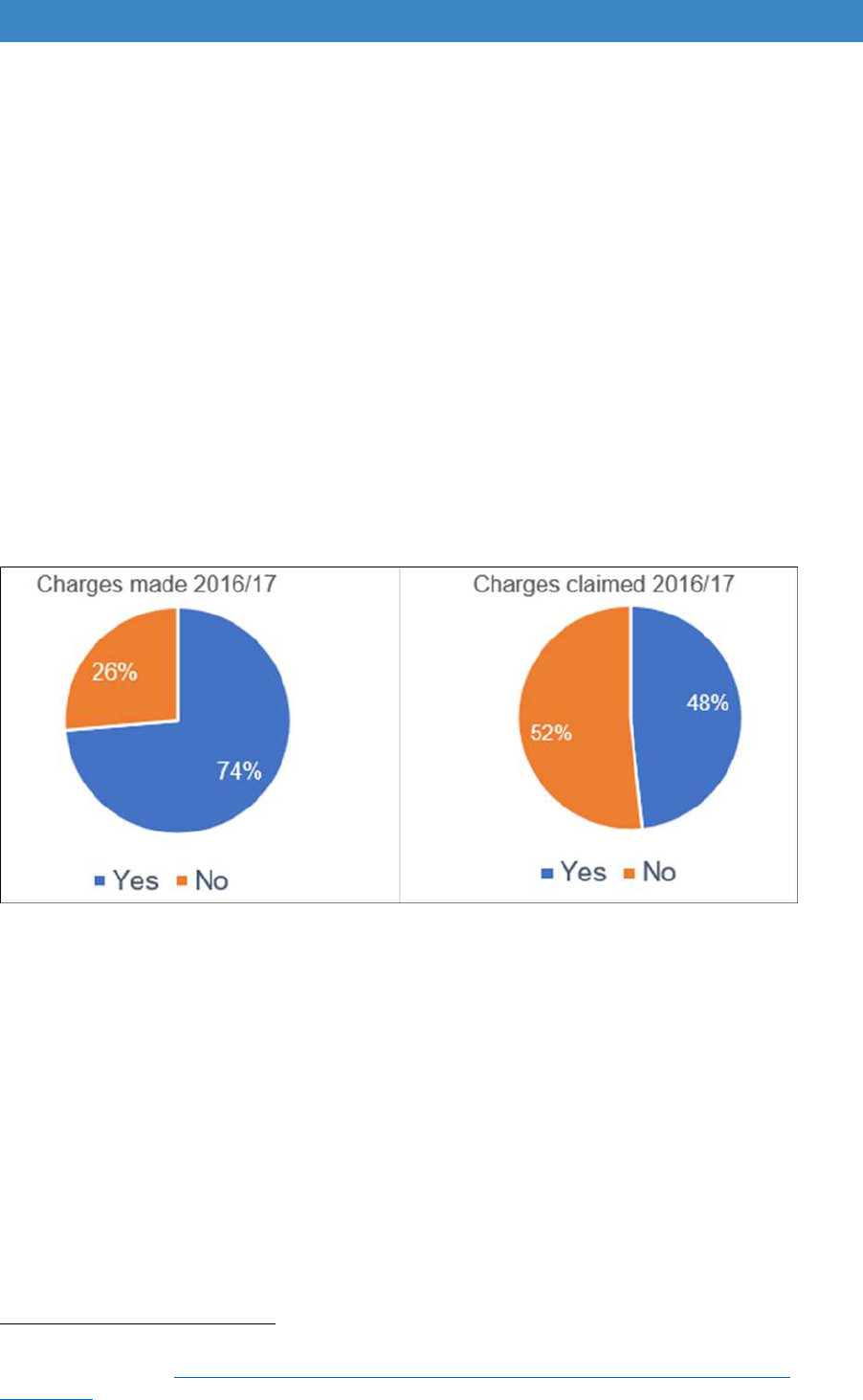
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
assessed by occupational therapists to be ‘at risk’ of going into hospital or
residential care
40
. These options are considered in Section B.
Land Charges
5.23 Local Authorities can place a local land charge if the cost of work is over £5,000,
with a maximum of £10,000 able to be claimed back. In 2016/17, three quarters
(74%) of authorities reported placing charges, with an average of 28 charges per
authority (Figure 5.9). In most cases there is a considerable delay before charges
can be reclaimed, as this is done when the house is sold. In 2016/17 only 48%
reported claiming charges (Figure 5.10). Among those that did, an average of
£31,600 per authority was returned. Some authorities get charges returned to
the DFG account, but others find the charge is simply absorbed into the local
authority general fund, meaning there is no direct benefit to future DFG
applicants.
Figure 5.9 DFG land charges 2016/17
Source: LOGASnet
Summary - types of adaptations and costs
Most grants (89%) are provided for people with physical disability issues and only
11% relate to dementia, sensory issues, learning disability or other impairments.
Cases are becoming more complex as higher numbers of people have multiple
conditions, including a mix of physical and mental health impairments. It indicates
that some may take longer to process, and staff may require more training.
40
Mackintosh, S. and Collingbourne, L. (2015) Home Adaptations for Disabled People Good Practice
Case Study: Wigan. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-
wigan1.pdf.
52

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
The DFG was originally devised to solve physical impairment problems. There
needs to be better guidance about the use of the DFG for mental health issues.
Better guidance is also needed for children’s cases, which are increasingly likely
to be about learning disability, autism spectrum disorders or behavioural issues.
Specific grants for sensory impairment, mental health issues and dementia may be
required, with small grants available for better lighting, deep cleaning and
decluttering to help improve living conditions. There is scope for these to be
delivered using the flexibility inherent in the RRO.
The average cost of a grant rose from just over £7,000 in 2009/10 to nearly £9,000
in 2016/17, reflecting increases in building costs that had been kept down through
strict approaches to value for money. Increased costs may also reflect a change in
the complexity of work.
The most common adaptations are showers (55%) and stairlifts (25%). The
average cost is just under £5,000 on average for showers, £2,400 for a straight
stairlift and £4,500 for a curved stairlift.
Overall 57% of DFGs cost less than £5,000, 35% were under £15,000 and only 8%
were over £15,000, but there is considerable regional variation. In London, only a
third of work is under £5,000, whereas in most other areas between a half and two
thirds is under £5,000. There are only about 8% of cases over £15,000 on average,
varying between 3% in the North East and 14% in London.
Some places do no extensions, most only do about two each year, with only a few
places doing more than 20 per year. Extension costs are highest in London –
averaging £55,000 – but in most other places average costs are kept around the
£30,000 upper limit. Some places with small DFG budgets avoid doing extensions
to keep costs down.
Reorganisation of internal space may be cheaper but may not provide adequate
solutions. Changes to the grant limit are required to deliver better outcomes.
Relocation support could provide better solutions for some of the worst housed, as
nearly 20% of those under 55 might be willing to move, but housing options
services need to be adequately resourced.
Three quarters of authorities use land charges to recoup some of the costs, but the
money is not always recycled back into the DFG.
53

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 6. Costs and benefits to local authorities
The benefits of adaptations and potential cost savings
6.1 The benefits of adaptations are numerous but are very difficult to quantify. Local
authorities have generally been good at recording outputs, such as grants
completed and amount spent, but much less effective at recording longer term
benefits to the individual or the impact on health and care spending.
6.2 Previous studies have shown the difficulties disabled and older people face when
their home becomes inaccessible and how much they value adaptations.
Heywood (2001), in one of the most comprehensive studies of both minor
adaptations and the impact of the DFG in England, said that “The evidence about
what was achieved by bath or shower adaptations was overwhelming. The
interviews showed how adaptations restored confidence, dignity and self-
respect, promoted independence and reduced stress” (p.11) and that, “Good
adaptations transform lives, improve health and keep people out of institutional
care” (p.1)
41
.
6.3 A review conducted in 2017 by the University of the West of England for the
Centre for Ageing Better found strong evidence about the benefits of minor
adaptations such as grab rails and removal of trip and fall hazards on the rate of
falls, improvement in activities of daily living and the impact on mental health
42
.
However, the evidence relating to the more common major adaptations provided
by the DFG, such as the replacement of baths with wet rooms or the provision of
stairlifts is much less robust. Most surveys are retrospective, asking people what
they feel after work has been carried out. There are few studies using objective
measurement of levels of independence, or the use of health and care services,
before and after an adaptation is completed.
6.4 Better evidence is beginning to be obtained. A pilot randomised control trial (the
BATH-OUT study) measured the impact and outcomes of replacing baths with
showers on disabled older adults and carers’ quality of life and on their use of
health and social care services
43
. The study compared the outcomes for older
adults receiving the usual local authority DFG service (the control group)
compared with a similar size group getting quicker provision (the intervention
group). Participants were followed up at three monthly intervals. Sixty
41
Heywood, F. (2001) Money well spent: the effectiveness and value of housing adaptations, Bristol:
The Policy Press.
42
Powell, J., Mackintosh, S., Bird, E., Ige, J., Garrett, H. and Roys, M. (Nov 2017) The role of home
adaptations in improving later life, London: Centre for Ageing Better. https://16881-presscdn-0-15-
pagely.netdna-ssl.com/wp-content/uploads/2017/11/The-role-of-home-adaptations-in-improving-later-
life.pdf.
43
Whitehead, P., James, M., Belshaw, S., Dawson, T., Day, M. and Walker, M. (2016) Bathing
adaptations in the homes of older adults (BATH-OUT): Protocol for a Feasibility Randomised
Controlled Trial (RCT) BMJ Open. 6, e013448. http://dx.doi.org/10.1136/bmjopen-2016-013448.
54
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
participants were recruited and randomised and the results are presented using
descriptive statistics
44
. Physical and mental wellbeing and people’s own
perception of their health improved after the shower was installed in both groups.
Ease of bathing also improved and fear of falling decreased. There was also a
reduction in the use of both informal and formal care. This study has
demonstrated “proof of principle” but was conducted in one local authority area
only. A larger study is needed to further evaluate the clinical and cost
effectiveness, including the effect of waiting times.
6.5 Determining the actual cost savings to health and social care is more difficult.
This is an international problem, not just one affecting the UK. Chiatti and
Iwarsson (2016) noted that there is a ‘paucity of systematic evaluations’ and ‘few
studies containing economic appraisals’
45
. The reasons they give for this are: the
heterogeneity of the client group; the variety of home environments; adaptations
not being easily standardised as they are customised to the needs of the client;
and the number and variability of outcomes. Most studies have tended to focus
on functional ability and/or falls.
6.6 Public Health England (PHE) has produced a toolkit to help local areas prevent
falls, and this estimates the impact of adaptations. Falls are a major issue for
health and social care, as a third of people 65 and over fall each year, rising to
half of those aged 80 and over, with about 5% of falls leading to fractures and
stays in hospital. Fragility fractures in older people cost the NHS and social care
about £4.4 billion a year, with about 25% of those costs attributable to social
care. Falls are not just costly to public services, but also have major negative
impact on the independence and quality of life of the person affected
46
.
Adaptations could potentially have a big impact as 75% of the deaths relating to
falls happen in the home, and falls represent 10-25% of ambulance calls to older
adults
47
. Older people represent the greatest pressure on hospitals, as they use
most bed days than other people once admitted in an emergency (65% of bed
days)
48
. Falls also often precipitate a move into residential care.
6.7 Using evidence from randomised control trials and systematic reviews, PHE
compared the impact of different interventions on falls, including exercise classes
and home adaptations. They estimated that adaptations produce significantly
higher returns on investment with £1 of investment in home assessment and
44
Whitehead, P., Golding-Day, M., Belshaw, S., Dawson, T., James, M. and Walker, M. Bathing
adaptations in the homes of older adults (BATH-OUT): Results of a Feasibility Randomised Controlled
Trial (RCT) Manuscript submitted to BMC Public Health March 2018.
45
Chiatti, C. and Iwarsson, S. (2016) Evaluation of housing adaptation interventions: integrating the
economic perspective into occupational therapy practice, Scandinavian Journal of Occupational
Therapy, 21:5. 323-333, https://doi.org/10.3109/11038128.2014.900109.
46
Public Health England (Feb 2018) A return on investment tool for the assessment of falls prevention
programmes for older people living in the community.
https://www.gov.uk/government/publications/falls-prevention-cost-effective-commissioning.
4747
Communities and local Government Committee (Feb 2018) ibid, p. 15.
48
National Audit Office (Mar 2018) Reducing emergency admissions. https://www.nao.org.uk/wp-
content/uploads/2018/02/Reducing-emergency-admissions.pdf.
55

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
modification saving £3.17 on health and care costs. If quality of life gains for the
individual are considered, savings rise to £7.34 per £1 spent. However, the cost
savings only apply to interventions for people who have been admitted to hospital
for a fall, they are mainly for minor adaptations and assume that qualified staff,
usually an occupational therapist, provide the assessment. The financial returns
are opportunity costs rather than actual savings, such as: reductions in pressure
on accidents and emergency departments and fewer hospital admissions.
6.8 BRE has calculated the costs associated with the most common Category 1
hazards in the homes of older people. These include excess cold (690,000
households); and falls on stairs and the level (467,000 households) and would
save the NHS £624 million in first-year treatment costs. The cost of remedying
excess cold is the most expensive, at almost £3 billion. The cost of remedying
falls is estimated to be around £982 per house for falls on stairs and £792 for
falls on the level. Providing handrails and better lighting is relatively cheap but
work to communal areas of flats may be much more expensive. Overall, work to
remedy Category 1 hazards would pay for itself in around 6.5 years for remedying
cold and 4.5 years for falls
49
.
6.9 PSSRU also looked at the cost of falls and estimated that the provision of
equipment and adaptations might result in a reduction in demand for health and
social care equivalent to £261 per recipient per annum, with quality of life
improvements valued at £1,379 per annum (using their more conservative
assumptions). Scaling this up to a client base of 45,000 individuals and an overall
expenditure of £270 million (equivalent to the total annual expenditure on
Disabled Facilities Grants in 2011 when the calculations were carried out) was
deemed likely to generate reductions in the demand for health and social care
services worth £156 million over the estimated lifetime of the equipment, and to
achieve quality of life gains of £411 million
50
.
6.10 A study of a broader range of adaptations in housing association properties in
Scotland showed that investment led to increased independence, confidence,
health, and autonomy for tenants. It also contributed to a shift in the balance of
care away from residential homes and hospitals by preventing accidents and
reducing care needs. It showed a total return on investment of £5.50 to £6.00 for
every £1 invested if benefits to tenants as well as those to health and social care
were included
51
. Using records about length of tenancy, they were able to
compare their sample with tenants who had not had adaptations. Findings
49
Garrett, H. and Burris, S. (2016) Homes and ageing in England.
https://www.bre.co.uk/filelibrary/Briefing%20papers/86749-BRE_briefing-paper-PHE-England-A4-
v3.pdf.
50
Snell, T. Fernandez, J. Forder, J. (2012) Building a business case for investing in adaptive
technologies in England, Personal Social Services Research Unit, Discussion Paper 2831, London:
School of Economics and Political Science.
51
Kempton, O. and Warby, A. (2011) Measuring the Social Return on Investment of Stage 3
Adaptations and Very Sheltered Housing in Scotland. https://www.hanover.scot/wp-
content/uploads/2015/11/SROI-VSH-and-Adaptations-full-report-final-Sept-2011.pdf.
56
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
showed that adaptations allowed tenants to remain in their sheltered housing unit
for an extra 2.7 years before needing residential care.
6.11 A survey of social care departments by Foundations attempted to link data on
DFG recipients with care data
52
. Only a few authorities were able to provide
returns due to the difficulties of linking datasets. The findings revealed that only
16% of people receiving a DFG had a domiciliary care package, and that there
was only a slight fall in the number of hours required a year after the DFG had
been completed. Most DFG recipients are likely to have either no care or informal
care from family and friends. However, as over a quarter of informal carers are
over 65, adaptations are likely to benefit them as well as the grant recipient
53
.
6.12 The Foundations survey used data from local authorities on the average age of
people taking up residential or nursing home places, age of death, and whether
they had previously received a DFG (Table 6.1). Results need to be treated with
caution as numbers were small; however, they indicate that people who lived in
homes adapted using a DFG had gone into care four years later than those who
had not had a DFG, and that they had only needed two, rather than six years, in
care. With residential care costs at around £28,000 a year, compared to average
DFG costs of around £7,000, this highlights the potential savings of providing
adaptations, but it needs further research.
Table 6.1 DFG and residential care
Average age
No previous DFG
Had DFG
Age moved into residential care /
nursing home
76
80
Age at death
82
82
Costs savings of adaptations for children and young people
6.13 Cost savings for younger people are likely to be higher. The costs of care are
greater and the benefits spread over a longer period. A study in Leeds of a small
sample of young people with Autistic Spectrum Disorders and challenging
behaviours showed the impact of providing adaptations on the ability of families
to continue their caring role
54
. In all cases, the young people’s behaviour carried
52
Foundations (2016a) Linking Disabled Facilities Grants to Social Care Data.
http://foundationsweb.s3.amazonaws.com/4210/foundations-dfg-foi-report-nov-2015.pdf
53
Department for Work and Pensions (2017b) Family Resources Survey, Carers data tables, Table
54
Clements, L. and McCormack, S. (2017) Disabled Children and the Cost Effectiveness of Home
Adaptations & Disabled Facilities Grants: A Small-Scale Pilot Study, Leeds: Cerebra, University of
Leeds. http://www.cerebra.org.uk/research/university-of-leeds-cerebra-legal-entitlements-and-
problem-solving-project/student-research-projects/.
5.2
57

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
a risk of serious harm to themselves and/or serious damage to property or harm
to other people if unsupervised.
6.14 Six families were interviewed by student researchers. Results showed that four
had had adaptions completed (or nearly completed) with the full costs being met
by a DFG ranging from £20,000 to £90,000 (average just under £60,000). Three
of the six families were certain that without the adaptations, their disabled son or
daughter would have become a ‘looked after child’ (LAC). The adaptations did
not fully solve the problems, and all the young people still needed substantial
care packages, but the changes gave much needed space in the home and
enabled the parents and the rest of the family to cope. In the other three cases,
one family thought they might have managed without the work, and in another
case the work had been on site so long that the family could see no benefit. At
the time of the interviews, the final family had experienced long delays and was
still waiting for work to start. They were concerned that they would not be able to
continue caring if something did not happen fast. The work was still not on site
when a few months later their child went into local authority care.
6.15 The study estimated that about 14 years of costs as a ‘looked after child’ had
been avoided by the adaptations. The costs of care at a weekly rate of £2,000
were estimated to be about £1.5 million compared to the average cost of the
adaptations of £60,000. However, this does not include the ongoing costs of care
at home and excludes any assessment of the impact on the wellbeing of the
disabled young people and their families.
6.16 The families had all experienced considerable delays in getting the work
approved and carried out. Even though the savings were considerable, the
research highlights the problems that arise for housing authorities trying to fund
high-cost adaptations from limited DFG budgets, when the savings relate to
social care and the NHS. Justifying such a high proportion of DFG expenditure
on a single case, particularly one that is not about physical disability, seems to
be a major reason why these cases take so long to be resolved.
“Some of the student researchers considered it extraordinary that a
grant of £60,000 might be refused even though the consequence was a
five-fold (or more) cost impact to the public purse”.
DFG outcome data
6.17 None of the research so far shows a definitive cost saving to the NHS or social
care, but they all show a very significant amount of cost avoidance. They also
show that adaptations deliver a health and wellbeing return that is worth far more
than the costs of the DFG in first year savings alone. Far more research is
needed to better quantify the outcomes of adaptations in terms of cost savings
to health and care.
58
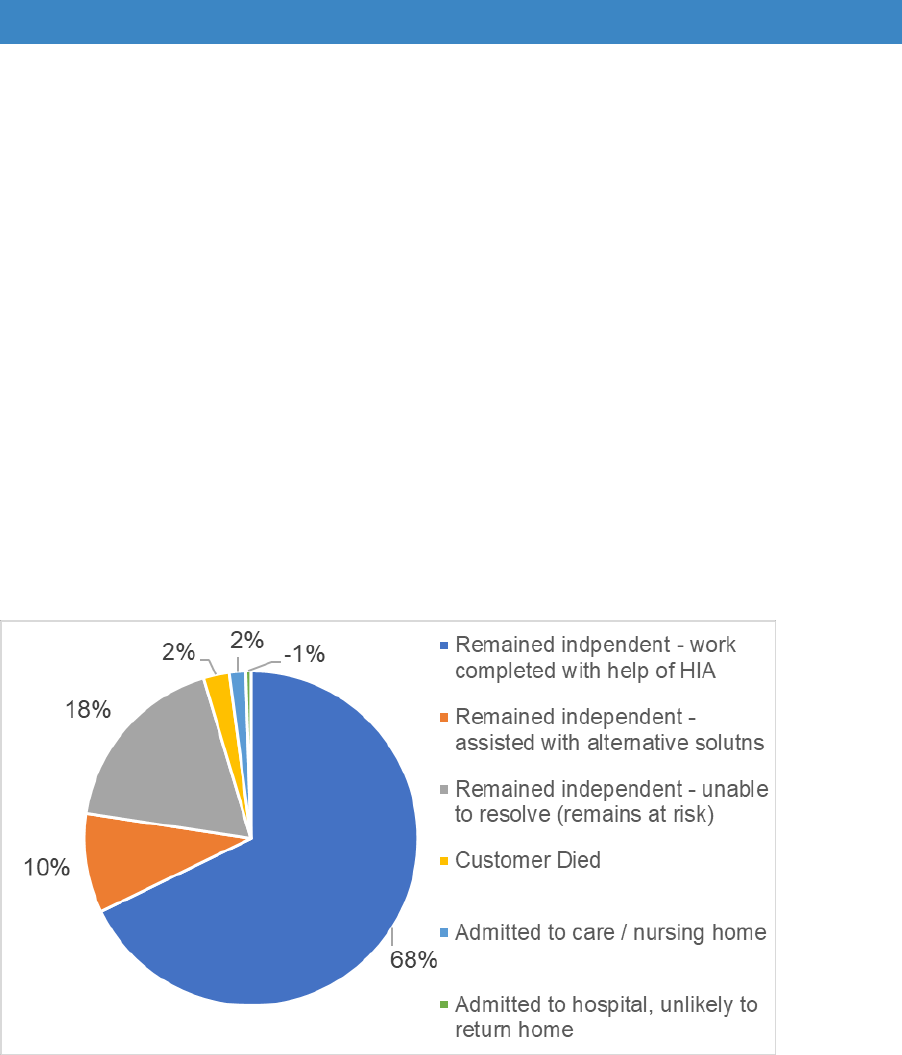
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
6.18 Some authorities are beginning to record what happens following adaptations.
However, it is hard for authorities with limited staff and large caseloads to spare
the time to revisit completed cases and record outcomes. The poor quality of IT
systems and lack of data sharing between health, social care and housing is a
further issue preventing good outcomes analysis. Despite the 2014 Care Act and
the BCF requiring use of NHS numbers on all case files, this is still not common
practice for DFG cases. The changes to data protection in May 2018 may further
hamper data sharing unless effective protocols are established.
6.19 One county authority with pooled data from all boroughs and districts was able
to show that most people (68%) had remained independent at home after work
was completed, while 10% had alternative solutions (possibly rehousing) (Figure
6.1). Only a small proportion had gone into residential or nursing care, been
admitted to hospital or had died. However, 18% remained at risk as the cases
had not been possible to resolve, but there are no details as to why.
Figure 6.1 Outcomes of completed cases – one county authority 2017/18
Source: outcome data provided to the review by a county authority in April 2018
The revenue costs of delivering the DFG
6.20 The revenue costs of delivering the DFG are not collected as part of LOGASnet
returns. The data are difficult to obtain as service delivery in most areas crosses
departmental boundaries. Occupational therapy staff are usually based in social
care and have other roles in addition to doing assessments and
recommendations for the DFG. The DFG team in housing authorities may be part
of a private sector housing or environmental health team, sometimes also with
additional duties.
59
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
6.21 Funding for most in-house local authority DFG services comes from the general
fund. Where occupational therapists are based in social care or children’s
services, their salary and overhead costs are from social care budgets, while the
revenue costs of most caseworkers, grants officers, technical officers and
administrative support are provided by housing departments budgets.
6.22 Although some authorities are trying to cover costs through fees, the evidence
indicates that is can only provide a proportion of the total amount. An example is
given in Table 6.2 of one local authority service in the North of England with a
DFG budget of over £1 million. They were expected to raise more than a third of
the revenue and overhead costs of £254,000 through fees charged as part of the
DFG but had only managed to raise a quarter of the costs. They had not received
any money from the BCF or social care to cover the service costs, despite
providing a home from hospital service and using an RRO policy to deal with cold
and damp homes to improve health. All revenue funding is from the district
council.
Table 6.2 Funding targets for a district council (excl occupational therapy costs)
2017/18
Expenditure
costs
£
Income
Target
£
Actual
income
£
Salary
169,000
Fees
Target %
92,500
36%
64,000
25%
Estimate of
accommodation
/services/supplies
85,000
District Council
contribution
161,500
190,000
Total cost
254,000
254,000
254,000
Source: written submission to the review
6.23 This is a common problem for Housing Authorities, that the benefits of
adaptations relate to both health and social care, but neither provide substantial
amounts of revenue funding, apart from covering the costs of occupational
therapists. In 2013 an Astral Advisory report based on surveys and interviews
with district councils concluded that services were under-resourced and
recommended that housing-related preventative work to delay or avoid hospital
admissions should be funded by CCGs
55
.
Independent HIAs
6.24 Most DFG services are within local authorities and there are now very few
independent HIAs. Those that remain do not always deliver the DFG, and where
they do, they often provide a range of other services. However, it is useful to look
55
Astral Advisory (2013) Disabled Facilities Grants in England: a research report, London: The
District Councils’ Network (DCN) and the Society of District Council Treasurers (SDTC).
60
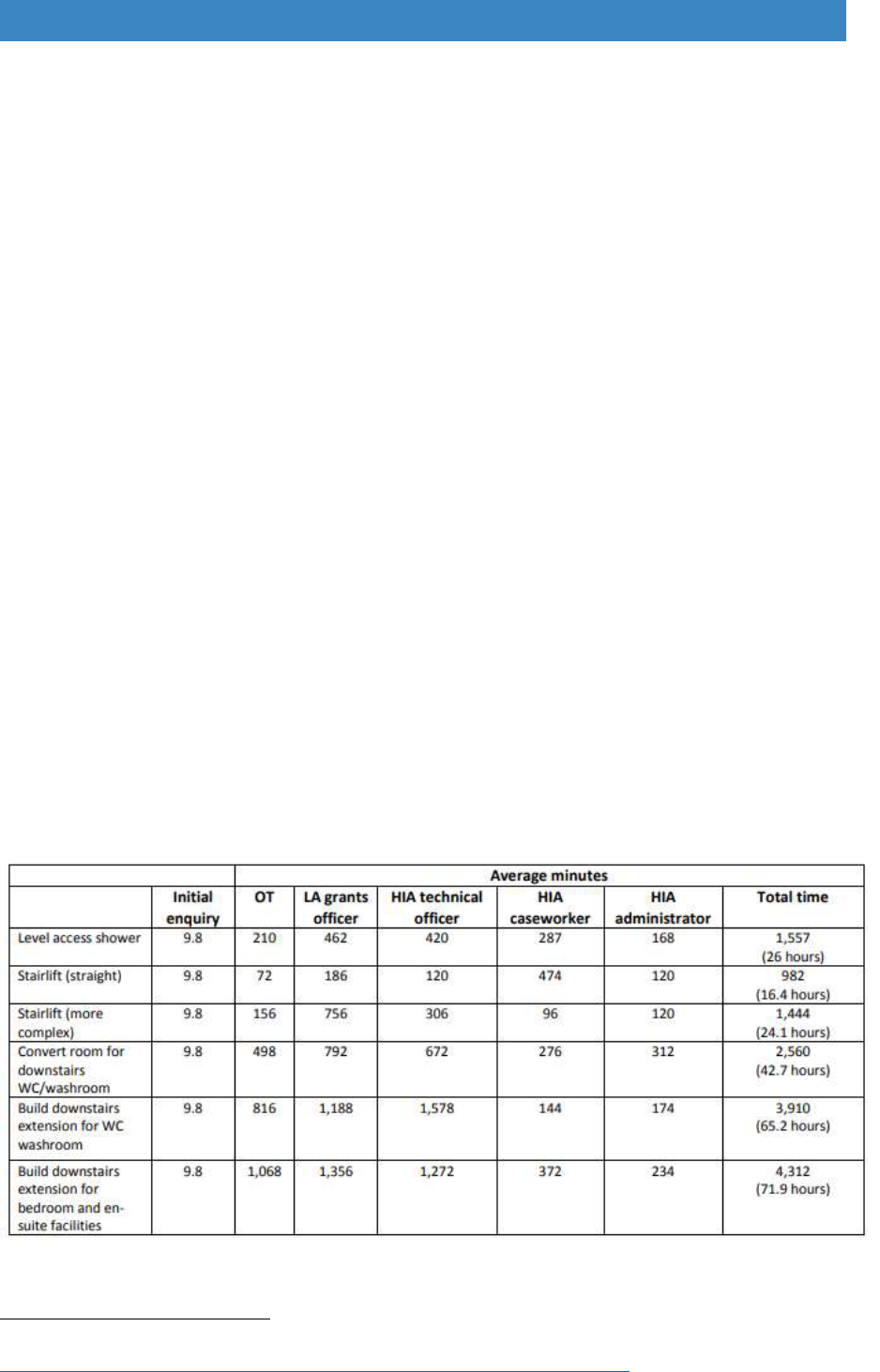
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
at their funding sources and compare them to those of internal local authority
agencies.
6.25 HIAs have a much wider mix of funding sources and it is very different from
internal DFG teams. Overall, three quarters come from health and social care,
with 29% from the BCF, 30% from adult social care and 15% from Clinical
Commissioning Groups (CCGs). Only a small amount comes from housing
authorities (7%). HIAs have a long history of charging fees but this only amounts
to 10% of the total, showing how difficult it is to rely on this for revenue funding.
Charitable funding is a source not available to local authorities, but only makes
up a very small amount of HIA resources (5%).
Staff costs by type of work
6.26 Staff costs are an important consideration when estimating the costs of providing
home adaptations. A study commissioned by PSSRU and undertaken by
Astral/Foundations identified the time inputs of staff involved in assessing clients
and in administering the process of supplying adaptations. Information was
received from 17 organisations (85% response rate). This included ten local
authorities, six Home Improvement Agencies (HIAs) and the British Association
of Occupational Therapists
56
. Table 6.3 shows the results. Level access
showers, the most common type of adaptation, take 26 hours of staff time to
process and deliver, excluding construction time. There may be efficiencies to
be gained by better use of staff time and better training of builders and
tradespeople to cut some stages of the process.
Table 6.3 Mean time inputs for staff involved in providing major adaptations
Source: PSSRU, Unit Costs of Health and Social Care 2017.
56
PSSRU (2017) Unit Costs of Health and Social Care 2017 [online].
https://www.pssru.ac.uk/pub/uc/uc2017/services.pdf?label=uc2017-services
61

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
6.27 Research by the Royal College of Occupational Therapists in 2013/14 involved
a survey of local authorities and home improvement agencies to obtain
information on the time inputs for staff for 18 commonly fitted adaptations
57
. The
results show:
Major adaptations - total mean cost £16,647 (range £2,474 to £36,681).
Staff costs were up to 24% of the total mean cost.
Minor adaptations - total mean cost £451. Average staff costs were 76%
of total mean cost.
6.28 Given the shortage of occupational therapists and the high proportion of DFG
delivery costs absorbed by outlay on staff, it is important to gain efficiencies so
that limited DFG resources can help more people. Part B looks at how better
routing of cases at the outset can make more effective use of more highly trained
staff, with more straightforward cases handled by trusted assessors. A tool is
provided to help work out what cases require occupational therapy input. RCOT
is also publishing a report on minor adaptations to show how they can be
delivered more effectively and efficiently
58
.
6.29 The reason why data on costs and benefits is so limited reflects a lack of
governance and oversight. LOGASnet has been an administrative tool, rather
than one designed to manage the service. At local level, the split in the way
services are managed between social care and housing means that there is
little data relating to the whole end-to-end DFG process. When the DFG
became part of the Better Care Fund, there was scope to develop better
measurement of inputs and outcomes, but no national metric was set about
independence in the home. As housing authorities are under-represented on
Health and Wellbeing Boards, no-one has clear responsibility to determine how
well the DFG is operating.
6.30 Staff at the operational end do not have a strategic view and do not have the
time or resources to follow up cases to determine the longer-term impact.
Without adequate data, operational staff find it very difficult to argue the case
for additional revenue funding, as they are unable to demonstrate the true costs
of the service and the benefits it delivers. Services have therefore remained
under-resourced even when central government funding has been increasing.
57
Curtis, L. and Beecham, J. (2018) A survey of Local Authorities and Home Improvement Agencies:
identifying the hidden costs of providing a home adaptations service. https://kar.kent.ac.uk/66433/.
58
Royal College of Occupational Therapists (In Press) Adaptations without delay: a guide to thinking
about and delivering adaptations differently. London: Royal College of Occupational Therapists.
62

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Summary - costs and benefits to local authorities
Analysis of the economic value of adaptations is difficult because of
heterogeneous disabled populations, differences in housing and care
circumstances, and the customised nature of many adaptations.
Benefits are also hard to measure because information on outcomes is not
routinely collected, data sharing is difficult and IT systems are poor.
Academic analysis is based on a limited number of systematic reviews, most
relating to the impact of minor adaptations on falls. However, these show
significant cost savings.
Cost saving for young people can be very high relative to the cost of adaptations
when it reduces numbers of ‘looked after children’.
There is little robust research relating to the outcomes of the type of major
adaptations provided by the DFG such as showers and stairlifts. However, the
BATH-OUT pilot shows a positive impact on health and wellbeing and a
reduction in the fear of falling. A larger study is needed to further evaluate the
clinical and cost effectiveness and the effect of waiting times.
Two small studies indicate that adaptations can delay entry to residential care
by nearly three to four years.
The costs of delivering the service are currently difficult to determine as
services straddle departmental and administrative boundaries. However, they
appear to be high, with occupational therapy costs alone being 24% of the costs
of an average DFG. Improved routing of cases would make more effective use
of the most highly skilled and expensive staff.
Without adequate data on costs and benefits it has been difficult to argue the
case for additional revenue funding. Services have therefore remained under-
resourced even when central government funding has been increasing.
Council-run DFG services get little support with revenue or capital costs from
health or social care despite the considerable potential impact of the DFG on
health and care outcomes. Independent HIAs have been better at obtaining
funding from a wider mix of sources.
Fees cannot address the shortfall in revenue costs and their use reduces the
amount of capital resources available for adaptations to people’s homes.
The paucity of data reflects a lack of governance and oversight. Despite the
DFG being part of the BCF, there are no national metrics about housing
outcomes or independence in the home. The need for better strategic oversight
is addressed in Part B.
63

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 7. Processing arrangements and waiting times
7.1 The legislation itself contains very little about how the grant process should work,
apart from saying that:
The grant cannot be approved if works have already started
There is a need to consult the social services authority
A decision notice is to be issued within 6 months of the date of application.
7.2 The process arrangements and delays are where there are significant concerns
about the current operation of the DFG. In 2016 the Local Government
Ombudsman said that “All too often in the cases we see, applying for and
receiving a Disabled Facilities Grant (DFG) is beset by delay
59
.
7.3 The Communities and Local Government Committee also commented that “Our
predecessor Committee considered the operation of the DFG in its inquiry on
adult social care, concluding that it was “slow and cumbersome”, so we were
interested to return to the issue. Once again, we heard that it was a “clunky
process” and that waiting times for implementation varied significantly between
local authorities, ranging from days and weeks in some places to two or three
years in others”
60
.
7.4 An FOI in 2015 by Leonard Cheshire got a 68% response rate from all 360
councils and revealed that almost 2,500 disabled people were waiting over a year
to get a DFG to make their homes accessible: “These delays are leaving disabled
people stuck sleeping in their lounge, washing at their kitchen sink or at risk of
falling down the stairs and needing hospital treatment”
61
.
Processing arrangements
7.5 When the DFG was first developed, the help provided by the local authority was
relatively limited. Applicants were given the application forms and asked to return
the completed paperwork with the requisite documentation and quotes for the
building work. Social care was consulted but the housing authority remained in
charge of the case. Figure 7.1 below shows that as the ‘minimal process’.
59
Local Government Ombudsman (2016) Making a house a home: Local authorities and disabled
adaptations, p. 1. https://www.lgo.org.uk/information-centre/news/2016/mar/delays-to-disabled-
facilities-grant-process-have-major-impact-on-people-s-lives-says-ombudsman.
60
Communities and local Government Committee (Feb 2018) ibid.
61
Leonard Cheshire Disability (2015) The Long Wait for a Home.
https://www.leonardcheshire.org/sites/default/files/Leonard-Cheshire-Disability-The-Long-Wait-for-a-
Home.pdf.
64

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
7.6 Over time, the main call centre for local authorities became based in social care.
This became the route into local authority services and calls about the DFG
ceased going direct to housing. This led to a new type of minimal process (termed
‘DIY’ in Figure 7.1).
7.7 Community occupational therapists began to play an increasingly important role
in the process. In 2003, the joint health and social care Integrated Community
Equipment Service (ICES) budget came into use and minor adaptations and
equipment became an alternative option to try before people were referred for a
DFG. For children’s cases there was often a separate call centre and a different
team of occupational therapists. The customer pathway evolved into the service
that is most common today: the ‘traditional process’. Social care (adults and
children’s) controls who is accepted as eligible for assessment and decides what
route to send people down. As social care has different eligibility criteria to the
DFG, some people are excluded from help or may not go down fast-track
pathways direct to the DFG leading to delays.
7.8 This traditional process also means that there can be different waiting lists.
There may be a wait for an initial assessment for aids, equipment or minor works;
another wait for a full occupational therapy assessment; and a further wait for a
DFG means test and grant approval. These handovers are confusing for
customers who may not know what department or member of staff is handling
their case. The 2014 Care Act said that service users should have a single point
of contact throughout the customer pathway, but this seems very difficult to apply
when service provision crosses departmental and administrative boundaries.
7.9 It is only recently that this traditional process has begun to change, as new
integrated teams have developed, comprising occupational therapists, casework
and technical staff. Teams can more easily work together, considerably
simplifying and speeding up the customer journey. This integrated model is
discussed in detail in Part B.
7.10 How processing arrangements work on the ground was explored at the
consultation events and in the online survey. Participants were asked to identify
which of the four different models they thought was closest to the way the DFG
service worked in their area. The majority said that their service was ‘traditional’.
However, when asked what service they would prefer, the majority opted for an
‘integrated’ service (Figure 7.1).
65
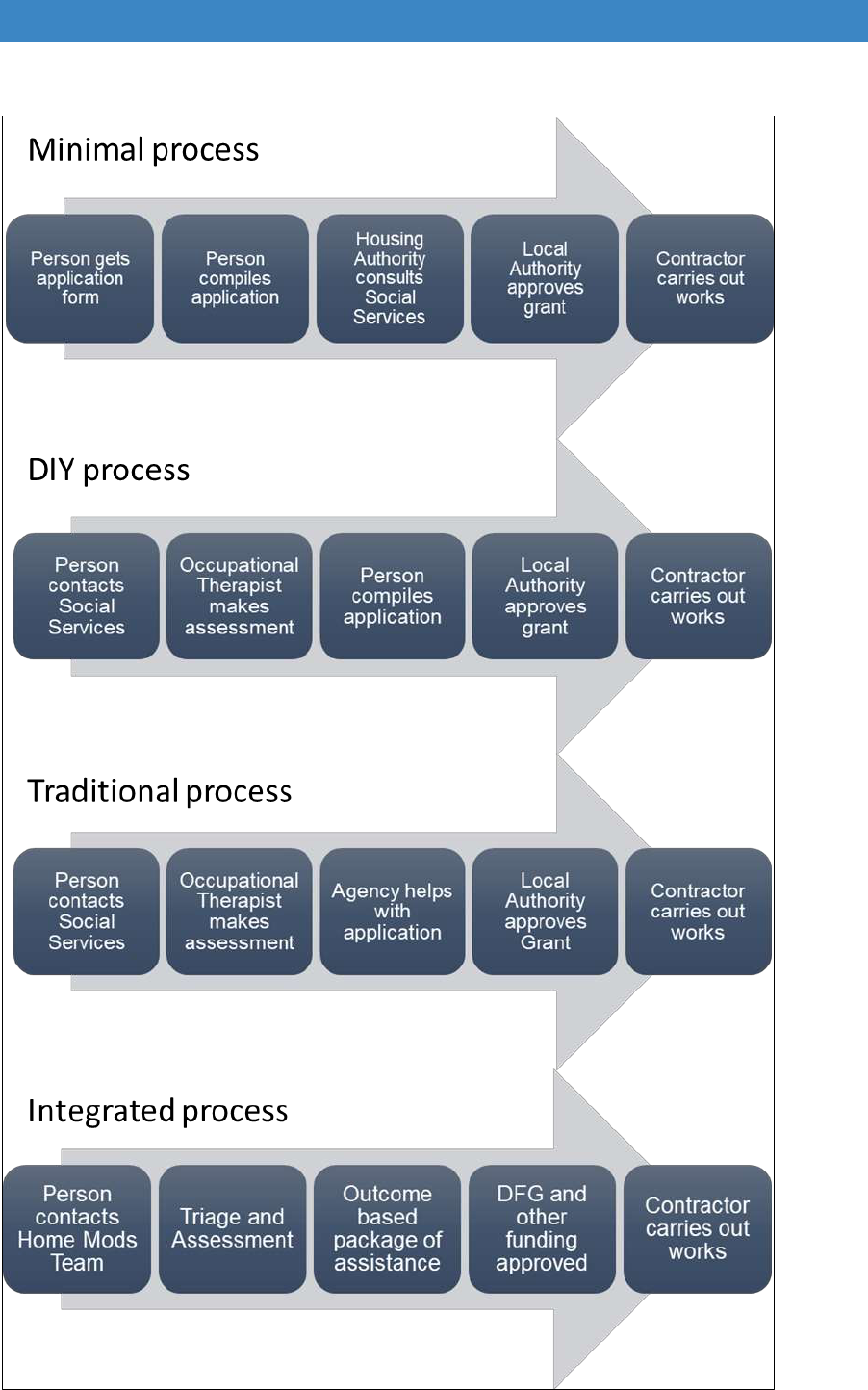
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 7.1 Types of DFG process
66
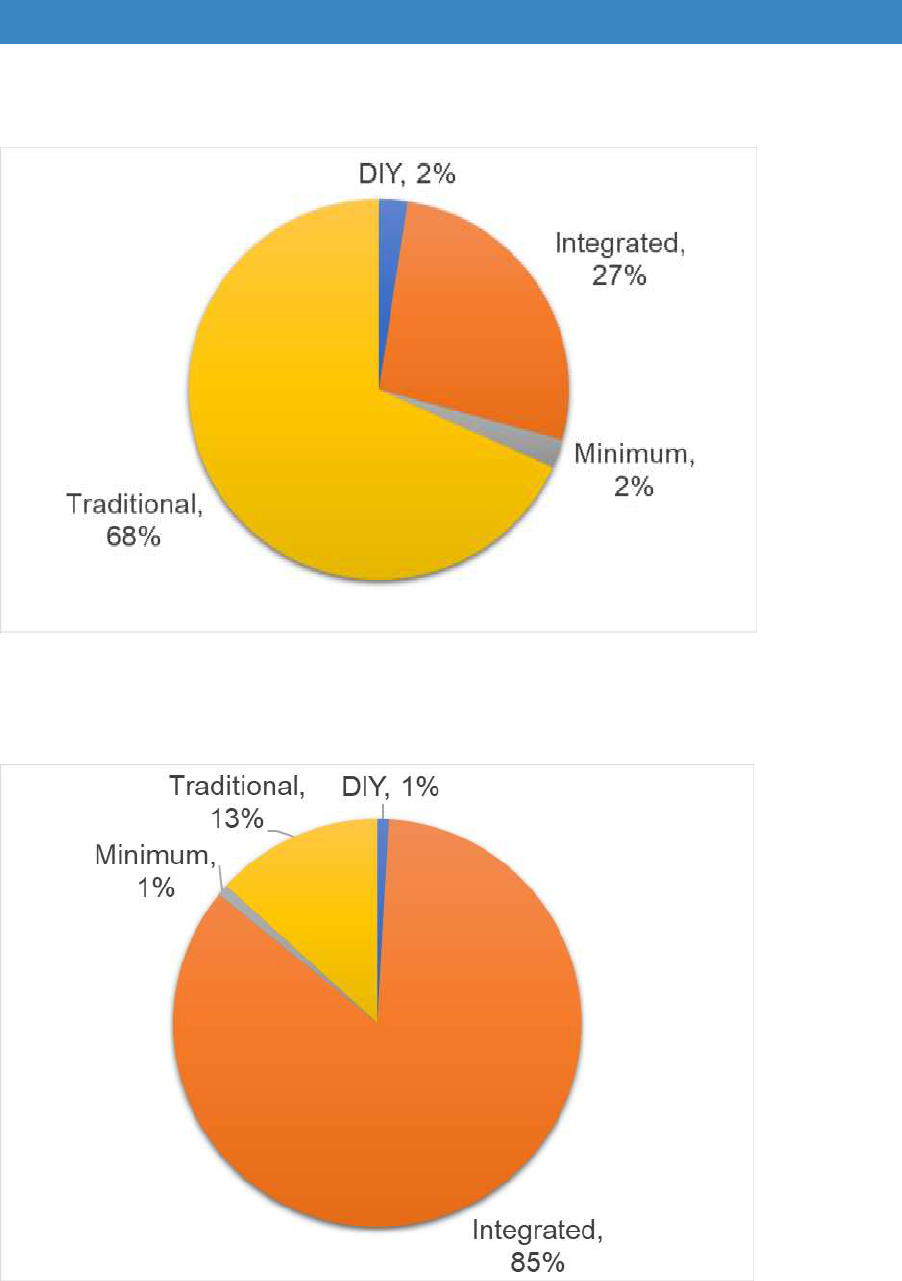
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Figure 7.2 Current DFG process
Source: voting at consultation events
Figure 7.3 Future DFG process
Source: voting at consultation events
Online survey: 76% integrated, 19% traditional, 3% minimum, 2% DIY
67
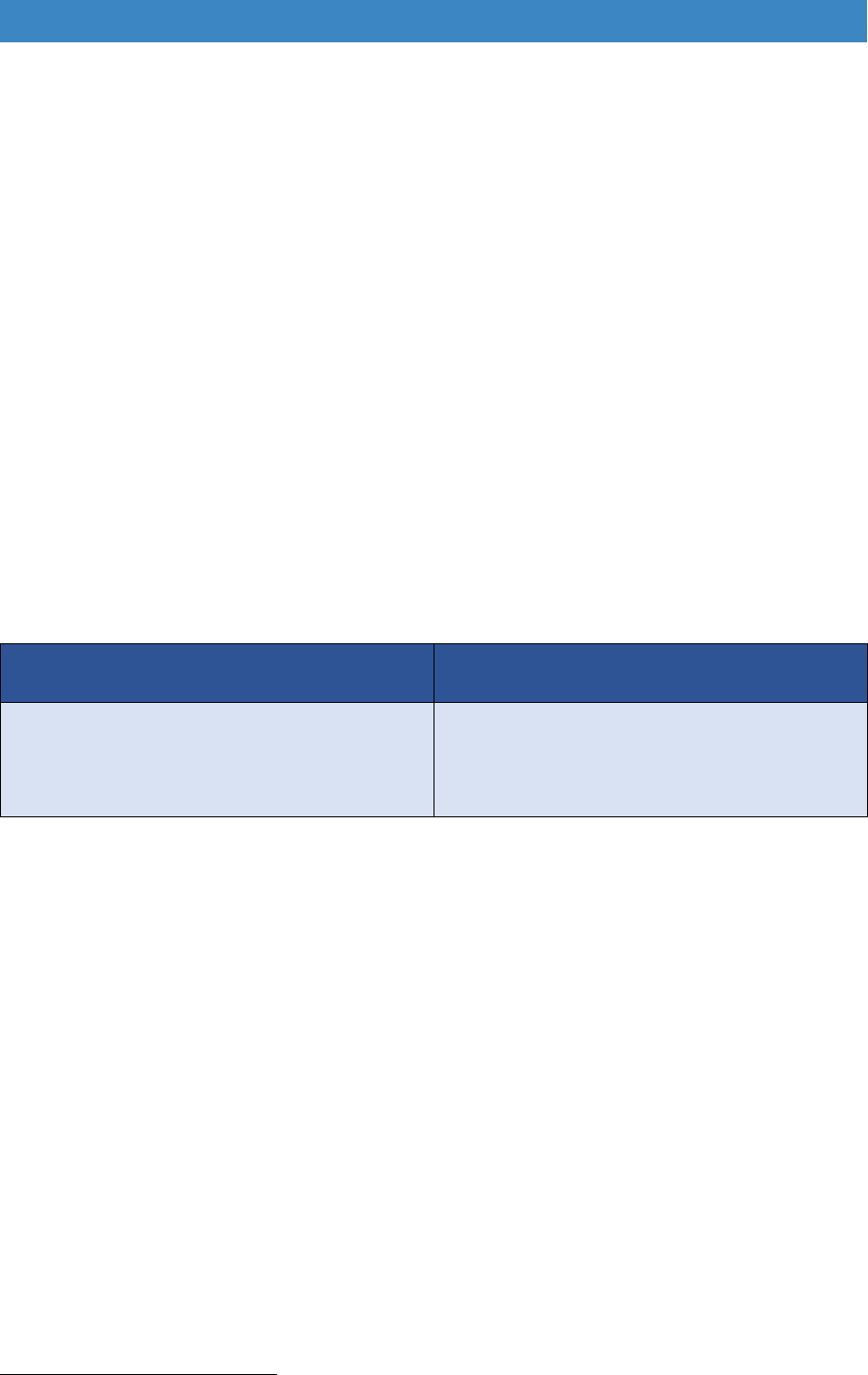
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Time taken to process grants
7.11 It is difficult to determine end-to-end processing times with any accuracy because
of the way services cross administrative boundaries. DFG teams with minimal,
DIY or traditional arrangements (where occupational therapists are in other
departments, or in county offices) often do not know the date of first enquiry or
how long a person has waited for an occupational therapy assessment. Housing
teams may not have access to social care IT systems to look this up. The only
comprehensive data collected by housing teams therefore relates to the end of
the customer pathway, when a DFG application has been submitted, often many
months after the first enquiry.
7.12 LOGASnet recorded some limited information on time periods for the first time in
2016/17. Table 7.1 shows that the average time from application to completion
of work is almost 7 months, but there is a huge range. As the CLG Committee
report indicated, some places appear to process work very quickly but in other
places it is extremely slow
62
. These time periods do not include the time spent
waiting for an occupational therapy assessment.
Table 7.1 time taken to process grants 2016/17
Average time between application
and approval (working days)
Average time between approval and
certified date (working days)
Nearly 10 weeks
(range: 1 day to over a year)
Over 17 weeks
(range: 3 weeks to 1 year)
Source: LOGASnet (Note - waiting time for occupational therapy assessment not included)
The effect of RRO policies on timescales
7.13 Since 2008, local authorities have been able to develop their own policy to
improve the delivery of adaptations. However, at the end of 2016 47% still had
no policy (Foundations FOI, Nov 2016). Some have been unwilling to take the
risk of spending mandatory money on discretionary schemes, while others have
so much demand for mandatory work, or are too short staffed, to be able to
explore more innovative ways of spending the money.
7.14 What is clear from more recent research is that those authorities with RRO
policies are, on average, delivering results faster, although some authorities are
very quick at delivering standard DFGs. Quicker services may be because they
have removed the means test or have some method of fast-tracking different
types of cases. Building work still takes the same amount of time (or longer if an
62
Communities and Local Government Committee (Feb 2018) ibid.
68
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
increase in throughput of cases cannot be matched by availability of contractors)
but the period from application to approval is more than halved (Table 7.2).
Table 7.2 Time taken to process cases for authorities using an RRO policy
Average
Application to
Approval
(working days)
Average Approval
to Completion
(working days)
Used RRO for more than 50
adaptations*
20.4
86.2
Did not use RRO at all
45.8
84.5
DFG Guidance (Non-Urgent)
See note**
80.0
Source: Foundations FOI 2017
*10 LAs reported that they completed 50 or more adaptations under RRO policies
**The 2013 Guidance has a target of 50 days from OT recommendation to approval
The effect of shortages of contractors on timescales
7.15 Regions with a shortage of contractors have longer delays between grant
approval and completion of work, particularly London, where it takes nearly six
months on average to get from approval of the grant to completion of work
compared to just over four months elsewhere (Table 7.3).
Table 7.3 Time taken from approval to completion by region
Region
Approval to Completion
(working days)
East Midlands
97
East of England
85
London
114
North East
84
North West
81
South East
85
South West
86
West Midlands
74
Yorkshire and The Humber
91
ENGLAND
89
Source: LOGASnet 2016/17
69

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Effect on disabled and older people, their families and carers
7.16 This analysis of how the DFG currently operate demonstrates how complex the
DFG system is for disabled and older people. If they are home owners or private
tenants, the first challenge is to find out about the grant, as in most areas it is not
advertised, and information is not freely available. Previous research has shown
that almost half of grant recipients found out about the DFG by word of mouth,
which does not seem a fair way to allocate public resources
63
. It means that those
who are less well-connected, more isolated, have mental health problems or
learning disabilities will be excluded, or only come to the attention of statutory
authorities at the point of crisis when adapting the home may be too late.
7.17 A study by Northumbria University and the Centre for Ageing Better found that
“People actually don’t know that these services are out there. And also how to
access them”. They added that “Navigating the route to getting the right
adaptations in place for the right person can be a challenge. If professionals
working in the field are unable to find their way through a system, then how can
we expect non-professionals to manage it?”. They recommend that local
authorities simplify the process of getting help and advice
64
.
7.18 Even when people get into the system, it is difficult to navigate. It crosses
administrative boundaries and few authorities have ways of ensuring that one
member of staff handles the case from end to end. There may be waiting lists at
each stage of the process. Few authorities or home improvement agencies have
online assessment systems which might speed up the process and allow people
to understand more about what the adaptation process entails.
7.19 The Lightbulb Project is an integrated adaptation service that is discussed further
in Part B. A customer insight project was carried out in 2015. This revealed that
health, housing and social care are not seen as separate services, and 95% of
respondents wanted a joined-up approach and less people to deal with.
7.20 In addition, filling in the application forms is not simple. Since 2008, LAs have
been able to develop their own more ‘user-friendly’ and less bureaucratic forms.
However, this has been very slow to change. In 2016, a Foundations FOI
identified that 45% of authorities were still using the old ‘prescribed form’. This
makes it difficult for those less able to deal with complex paperwork.
63
Mackintosh, S. and Leather, P. (2016) ibid.
64
Centre for Ageing Better (July 2018) Homes that help: A personal and professional perspective on
home adaptations. https://www.ageing-better.org.uk/sites/default/files/2018-07/Homes-that-help-
research.pdf.
70

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
The suitability of the six-month time limit
7.21 Cerebra and students from The University of Leeds explored the application
process
65
. The 1996 Housing construction and Regeneration Act, Section 34
requires housing authorities to approve or refuse a grant application as soon as
is reasonably practicable and not later than six months after the date of
application. Under Section 36 the actual payment of the grant may be delayed
until a date not more than 12 months following the date of the application.
7.22 The Cerebra evidence suggests that some local authorities frustrate this process
by: not making the forms available until social care departments have provided
supporting evidence; delaying the pre-application process by a shortage of
assessors; or advising potential applicants that the budget for the year has been
spent and deferring applications until the following year. The 2013 good practice
guide states clearly that the six and 12-month deadlines are the maximum, rather
than the norm, and that a delay of 12 months is exceptional and contrary to the
intention of the DFG programme
66
.
7.23 A report by Leonard Cheshire in 2015 found that a third of authorities had failed
to approve DFGs within the statutory period of 6 months and that about 4,000
people waited longer than they should have for a decision
67
. About 2,500 waited
more than a year for a decision, and almost half of councils had examples of
people waiting for more than two years.
7.24 The good practice guide points out that the legislation allows an individual to
complete and lodge an application themselves or with the help of a third party.
Authorities cannot put obstacles in the way of this process and must consider
any application that has been made.
7.25 Cerebra sent out a FOI in November 2017 to 54 local authorities comprising a
mix of district councils, metropolitan authorities, unitaries and London Boroughs.
By March 2018, they had received 43 responses. Just over half (53%) said they
made DFG forms freely available, but several said this was only after an
occupational therapy assessment, a referral, or a HIA visit. Only 7% had forms
available online. The difficulties in obtaining a form was indicated by the fact that
only 42% of the authorities sent a copy of the form to the researchers as directly
requested in the FOI. It was noted that several of the forms received appeared
‘inappropriately complex and demanding’.
65
Clements, L. and McCormack, S. (July 2018) The accessibility of Disabled Facilities Grant
application forms in England. Leeds: University of Leeds, Access Committee for Leeds.
66
Home Adaptations Consortium (2013) Home adaptations for disabled people: a detailed guide to
related legislation, guidance and good practice, Nottingham: Home Adaptations Consortium.
http://careandrepair-england.org.uk/wp-content/uploads/2014/12/DFG-Good-Practice-Guide-30th-
Sept-13.pdf.
67
Leonard Cheshire (2015) ibid.
71

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
7.26 The Cerebra research recommends that the Government provide explicit
guidance, or issue regulations under section 2(4) of the 1996 Act, to ensure local
authorities provide a statutory application form.
The impact of delays
7.27 Delays and complexity make the DFG process very frustrating for disabled and
older people coping with the inaccessibility of their homes and the indignity of not
being able to wash or use a toilet unaided. Where people are in pain or have
depression, their medical problems may be made worse. Problems are
particularly acute for people with life limiting conditions. Research by DEMOS for
the Motor Neurone Disease Association (MND) suggested that in many
authorities there was little understanding of the needs of people with MND, and
no fast-track process for people with rapidly deteriorating conditions
68
.
7.28 The results of the BATH-OUT randomised control trial suggest that physical
wellbeing slightly worsened while older adults were waiting for adaptations but
improved once the shower was installed
69
. There was also a difference in mental
wellbeing between those who had had an adaptation and those who were still
waiting. Fear of falling got slightly worse during the waiting period but decreased
once people had the shower fitted
70
.
7.29 On average, there was only a three-month delay between the intervention group
and control group in the BATH-OUT study. The delays that most people
experience before they get an adaptation installed in many local authorities is
considerably longer. The BATH-OUT findings indicate a potential decline in
physical and mental function during that waiting period, although this requires
further evaluation. Focussing on prevention and speeding up the process are
therefore key recommendations of this review.
Summary of issues - processing arrangements and waiting times
Most DFGs are delivered using a ‘traditional’ process. This is complex, slow
and difficult to understand from a user’s perspective.
There is seldom a single point of contact for the service user despite this being
an obligation in the 2014 Care Act.
Services cross administrative boundaries which make it difficult to determine
end to end times.
68
Vibert, S. (2017) MND Costs: Exploring the Financial Impact of Motor Neurone Disease, London:
DEMOS. https://www.mndassociation.org/wp-content/uploads/DEMOS-FULL-report.pdf.
69
Whitehead, P. et al. (2018 in press) ibid.
70
NB – confidence intervals were wide and non-significant as this was a pilot study and the sample
size was small.
72

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Customers do not understand these administrative divisions and want services
that are simpler, quicker, more joined-up and with fewer people to deal with.
The time from approval of grant to completion of work varies considerably
between authorities. Those authorities using an RRO policy appear to be
processing cases more quickly.
Some authorities seem to be manipulating the application process to manage
waiting lists and demand and very few have simple application forms that are
easily available.
Delays appear to have a detrimental effect on health, mental wellbeing, and
fear of falling, even over a three-month period, although this needs further
research.
A quarter of authorities responding to the consultation have developed more
integrated processes and most authorities see this as the way forward.
73
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Part B
How the DFG should change
“With a bit of courage and innovation, we have a chance to
improve a system that, when it works, dramatically changes
disabled and older people’s lives for the better.”
Papworth Trust 2012.
74
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 8. Introduction to Part B
8.1 In 1994, not long after the DFG was introduced, Heywood said that “the difficulty
in writing about adaptations is that the systems for arranging them are so
complex; many people are involved, working for different organisations, with
different budgets and practice varies greatly from area to area”
71
. Unfortunately,
this is still true.
8.2 This is a practical review that aims to simplifying the process for the customer.
The intention is to make recommendations that will work in all areas, despite the
fact there is a huge range of authorities from small districts to large unitaries,
each starting from a different baseline.
8.3 It must be emphasised at the outset that the review confirms the need for the
DFG to remain a mandatory grant. It is essential that disabled and older people
everywhere can get the help they need to remain living in their own homes.
8.4 During the course of this review we met a lot of very committed people delivering
home adaptations but having to work around outdated regulations. There is a
need to bring the regulations and guidance up to date, and to ensure that the
flexibility given by the 2002 Regulatory Reform Order (RRO) is used to provide
people with a more holistic service. It is no longer just about the delivery of
showers, stairlifts and ramps, but joining up a range of services to give disabled
and older people a more independent life.
8.5 In Scotland, a working group was established in 2011 to review adaptations
practice and propose recommendations. In the 2016 report ‘Adapting for
Change’
72
, they set out core principles for developing the adaptations service of
the future. Altered slightly and expanded, these principles also apply to England:
The person and their carer(s) should be placed at the centre of service
provision and be in control.
Support for adaptations should have a prevention focus.
Adaptations should promote enablement.
Access to assessment and provision should take account of need and be
fair, consistent, reliable and reasonable and take a holistic view of a
person’s life.
Assessment and access to financial and other non-financial support for
adaptations should be equitable, fair, anti-poverty and complement systems
for personalised support.
It is essential that housing services are coordinated with health and social
care to achieve joined-up, person-centred approaches.
There should be strategic oversight and a focus on outcomes that feed back
into continual service improvement.
71
Heywood, F. (1994) Adaptations: finding ways to say yes, Bristol: SAUS Publications, p.5.
72
Scottish Government (2017) Evaluation of Adapting for Change, Edinburgh: Scottish Government.
http://www.gov.scot/Resource/0052/00524668.pdf.
75

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
The structure of Part B
8.6 The first section of Part B looks at the context in which the DFG is now operating.
Proposals are made for a new form of strategic oversight to drive forward
changes in the way the DFG and adaptation services are delivered in both unitary
and county authorities. It links the governance of adaptions more firmly into the
Better Care Fund (BCF), or any new funding system that replaces the BCF, and
gives a clearer role for Health and Wellbeing Boards (HWBs).
8.7 The customer journey is very much faster in places that have joined up elements
of service delivery. Evidence from good practice examples is used to
demonstrate how the process could be improved in both unitary and county
authorities. There are also recommendations about new ways for staff to work
together to provide person-centred and consistent solutions and for the DFG to
be better linked to health and social care to provide a more preventative and
holistic service for disabled and older people.
8.8 The distribution of DFG resources nationally does not always relate to need, with
budgets under greater pressure in some areas than others. Options are
presented about how the national allocation formula can be updated to provide
a more equitable distribution. It looks at how risk can be shared better between
authorities, particularly for more expensive adaptation cases. There is a role for
other funding sources where adaptation work relieves pressure on health and
social care. There is also a need for better integration with social care budgets,
such as the Integrated Community Equipment Service (ICES).
8.9 The regulatory framework is also part of this review. The current £30,000 upper
limit needs adjusting to account for inflation and to better reflect the cost of work.
The means test also needs to be updated. Options are given to show the effect
of taking into account changes to benefits or matching the DFG means test to
that for social care. Other aspects of regulation and guidance are discussed such
as developing an RRO policy or including warranties in the DFG.
8.10 Linked to changes in the way services are delivered is the need for
transformation in the design of adaptation solutions and the use of more
innovative products for the next generation of disabled and older customers.
There are opportunities for DFG spending power to be used to shape the market
and drive innovation. This leads into a discussion of how people who are not
eligible, or chose not to use the DFG, can be helped with advice, information and
support and how it might be delivered.
8.11 The last section gives recommendations for improving adaptations delivery in
different tenures and looks at the impact of the introduction of Section 36 of the
Equality Act 2010 for people living in accommodation with communal areas.
76
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
Chapter 9. The bigger picture
“Fundamental reform is the only way that the preventative benefits of
home adaptations can be achieved nationally and the long-term cost
savings for health and social care realised. Anything less than major
reform, we believe, would just be a ‘sticking plaster’ on a failing system.”
Papworth Trust 2012
73
9.1 As Section A has shown, although there are pockets of good practice, the
process of grant delivery is not working effectively in most areas. A high
proportion of disabled and older people do not know about the grant; it is split
between administrative organisations, it is too slow, and too many people drop
out of the process (about 35% of applicants on average), often without recourse
to other forms of assistance. What people want is an easy to access, simple
understand, responsive service where they can get advice, information, funding
and practical help within a reasonable timeframe.
The Disabled Facilities Grant - a hidden service
9.2 A key reason for the difficulties in the operation of the DFG is the split in
responsibilities. Housing authorities have the mandatory duty for the DFG, but
social care has the ultimate duty for disabled and older people as well as disabled
children. The DFG legislation requires the housing authority to consult the social
care authority, resulting in occupational therapists in social care handling the first
part of the customer journey with a handover to the housing authority to complete
the work. There is no service with overall responsibility. This means that in many
areas the DFG is effectively hidden, as there is no single senior strategic
manager speaking up for it, and it has become so complex that people outside
of the service do not understand it.
9.3 Joining up services was recommended in the 1996 circular on private sector
renewal and in the 2005 review. It is time it actually happened. Disabled and
older people deserve a better service, and it requires stronger strategic oversight
to drive reform.
9.4 It has been difficult for central government to reorganise DFG services over the
last decade. Policies such as localism and devolution have put the focus on
place-based decision-making and reduced the ability of central government to
provide strong guidance.
73
Papworth Trust (2012) Home solutions to our care crisis, Cambridge: Papworth Trust.
https://www.housinglin.org.uk/_assets/Resources/Housing/OtherOrganisation/homesolutionstoourcar
ecrisis.pdf.
77
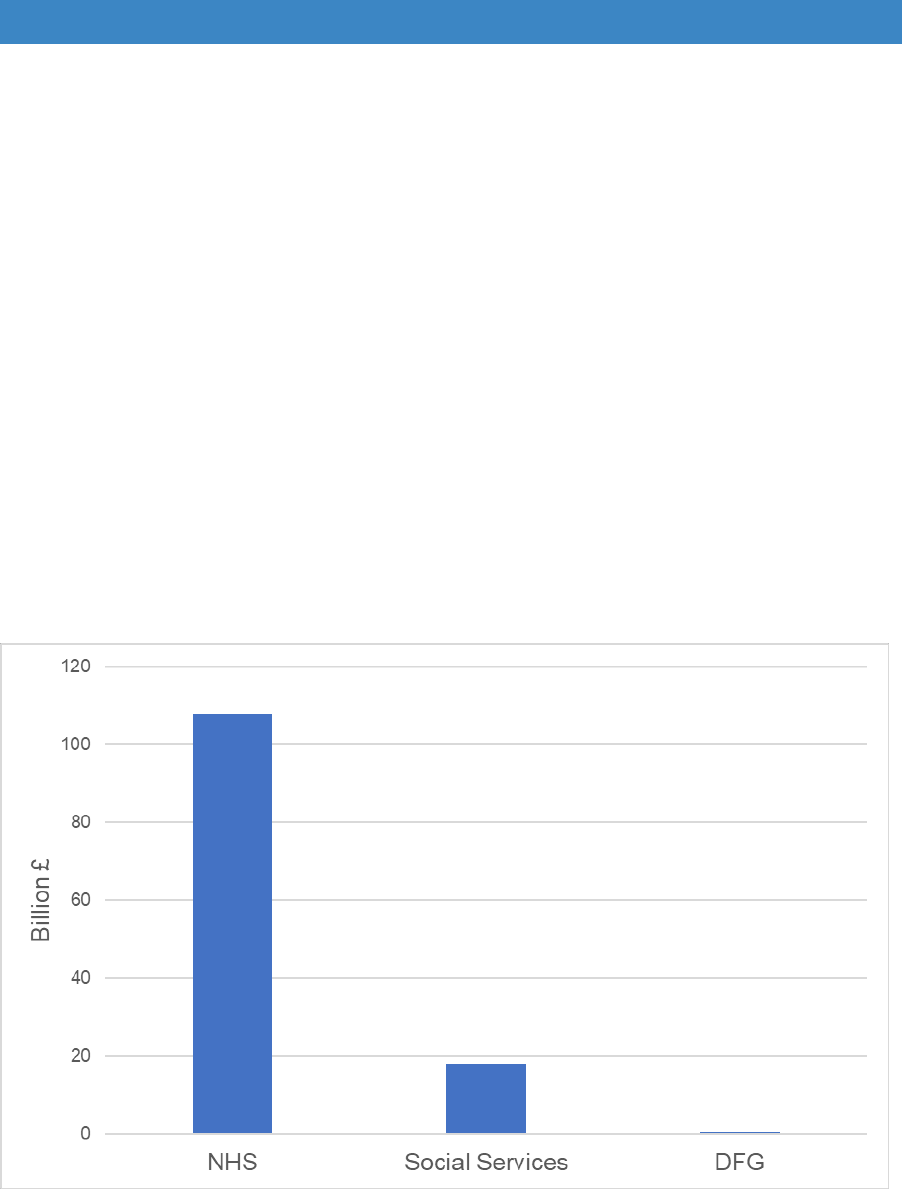
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
9.5 In the media, the discourse about housing and local policy-making tends to be
dominated by new-build and development issues. Few people understand what
a small proportion new-build adds to the stock each year, or that disabled and
older people are mostly in the existing stock (over 90%) not in specialised
accommodation. These misconceptions further disadvantage the DFG in the
policy arena.
9.6 Integration planning for health and social care might have been expected to give
greater prominence to safe and accessible homes, but Figure 9.1 shows that the
DFG is dwarfed by the funding available to health and social care. As it is a
comparatively small budget, it has been all too easy to ignore its importance,
especially when social care and health services have been under so much
pressure. It has not been enough to provide more funding for the DFG. To create
fundamental change in the way that it is delivered requires much stronger
strategic oversight to give more importance to the role of housing in the delivery
of health and care services.
Figure 9.1 The comparative size of health, social care and housing budgets 2018/19
DFG and the Better Care Fund (BCF)
9.7 The DFG has been part of the Better Care Fund (BCF) since it first began in April
2015. This seemed like a better home for the grant and a way of bridging the
boundaries between housing, health and social care. But, perhaps inevitably, the
78
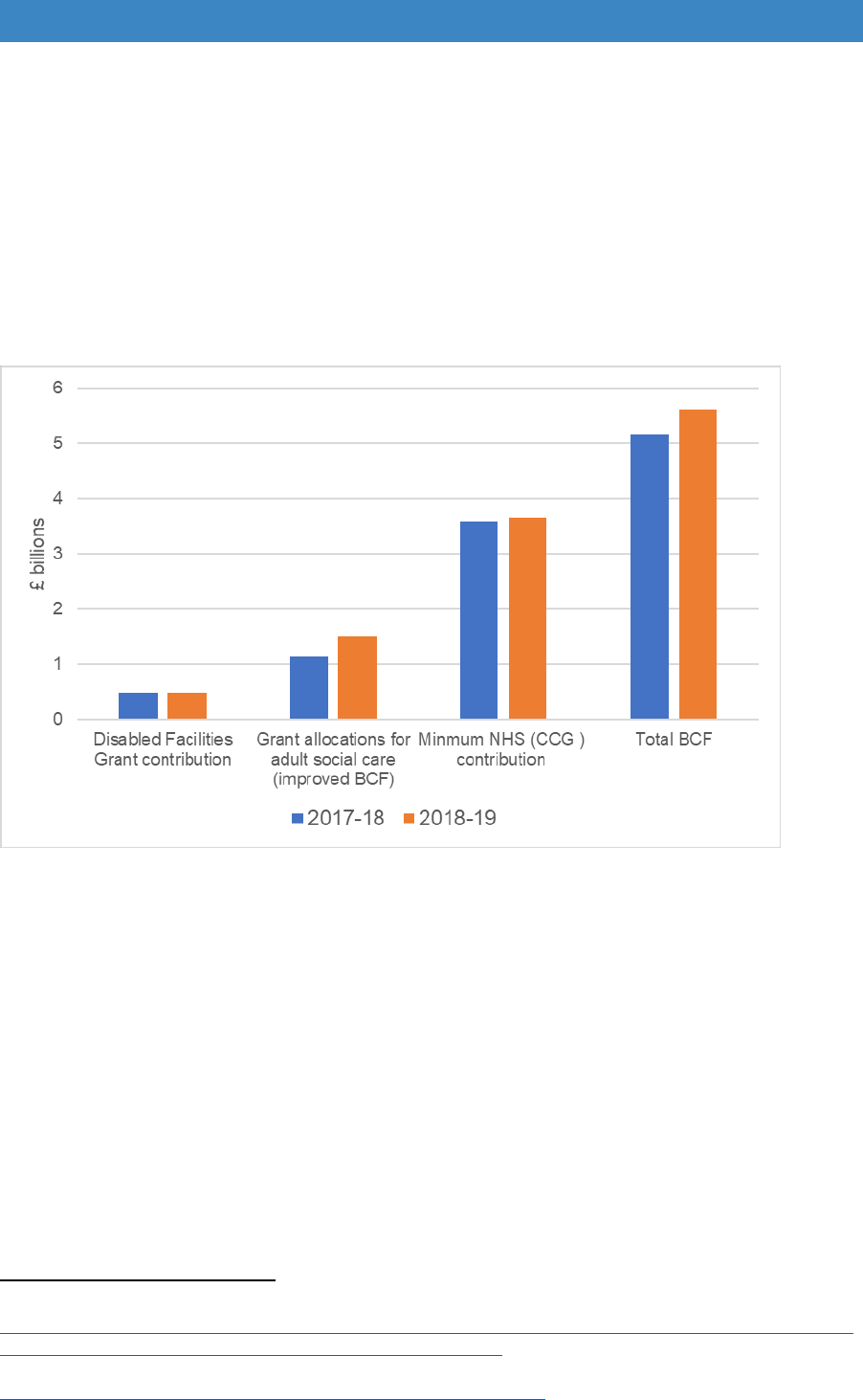
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
focus of the BCF has been on short-term health and social care interventions to
speed hospital discharge, or to reduce accident and emergency attendance and
admissions to care homes. Although the DFG can be delivered fast, it is mainly
about prevention and medium to long-term solutions. Added to that, it is only a
small part of the fund and the BCF did not require statutory reporting of housing
outcomes, which gave it little prominence in health and care planning (Figure
9.2).
Figure 9.2 DFG as a proportion of the Better Care Fund 2017-19
Source: Department of Health (2017) 2017-19 Integration and Better Care Fund: Policy Framework
74
9.8 A report by the National Audit Office in 2017 said that although the BCF was the
principal integration initiative, it had still not achieved its potential to produce
substantial cost savings or reduce acute hospital activity. Where the BCF had
delivered the greatest success was in incentivising local areas to work together,
although local authorities’ engagement in planning and decision making was
variable
75
.
9.9 Each county and unitary authority has a Health and Wellbeing Board (HWB)
which brings together key health and social care commissioners with the local
Healthwatch. They have responsibility for signing off BCF Plans. The BCF
planning documents say that “Housing authorities should be involved in the
74
Department of Health (Mar 2017) 2017-19 Integration and Better Care Fund: Policy Framework
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/60
7754/Integration_and_BCF_policy_framework_2017-19.pdf.
75
National Audit Office (2017) Health and social care integration.
https://www.nao.org.uk/report/health-and-social-care-integration/.
79

Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
development of the BCF plan elements related to housing and DFG”
76
. However,
there appears to be little representation of housing on HWB boards, or on the
BCF committees that feed into these boards, which has made it very difficult for
the role of the DFG to be fully understood and appreciated.
9.10 A further complication in the original structure of the BCF is that it did not include
the already well-established, joint health and social care budget: the Integrated
Community Equipment Service (ICES) which funds equipment and minor
adaptations. This seems a significant oversight. It is very difficult to develop joint
working without the DFG and ICES being considered by the same oversight
body. Reablement services were included in the BCF, but they do not typically
use the DFG; instead, they use ICES funding to supply the short-term needs of
people coming out of hospital.
9.11 In contrast, community occupational therapists rely on both ICES and DFG
funding, as most disabled people needing their home adapting require a range
of services including: equipment, such as specialist beds, perching stools, or
walking aids (ICES budget); minor adaptations such as grab rails or stair rails
(ICES or part of DFG budget); alongside more major works, such as showers
and stairlifts (DFG budget). A few areas chose to include ICES in the BCF to
provide more integrated services (such as Worcestershire, Warwickshire,
Camden, and Norfolk) but it was not a statutory requirement.
9.12 The Audit Office report agreed that that ‘place-based planning’ was the way
forward but that local areas were not on track to achieve the target of integrated
health and social care by 2020. The BCF will remain in place until 2019-20 and
it will be reassessed at the next Spending Review. Local partnership working in
some form seems set to continue. The aim of this review is to ensure that,
whatever funding and organisational structure is in place, there is a clear focus
on helping people to live well for longer in their own homes.
Strategic oversight
9.13 A new strategic oversight structure is needed to provide clear responsibility for
planning adaptation services, setting priorities and making services accountable
for performance delivery and outcomes. The best way of delivering this is through
a formal partnership between the local housing authority, health authority and
social care, as has happened in Scotland and has been proposed in Wales.
“When the partnership approach works well, and in particular where all
the necessary services are round the table and are engaged and
committed participants, the approach not only supports positive change
in the field of adaptations but can radiate out and have a positive effect
across a range of housing, social care and health functions. Building new
working relationships and an increased understanding of others’ roles
76
NHS England (Aug 2017) ibid.
80
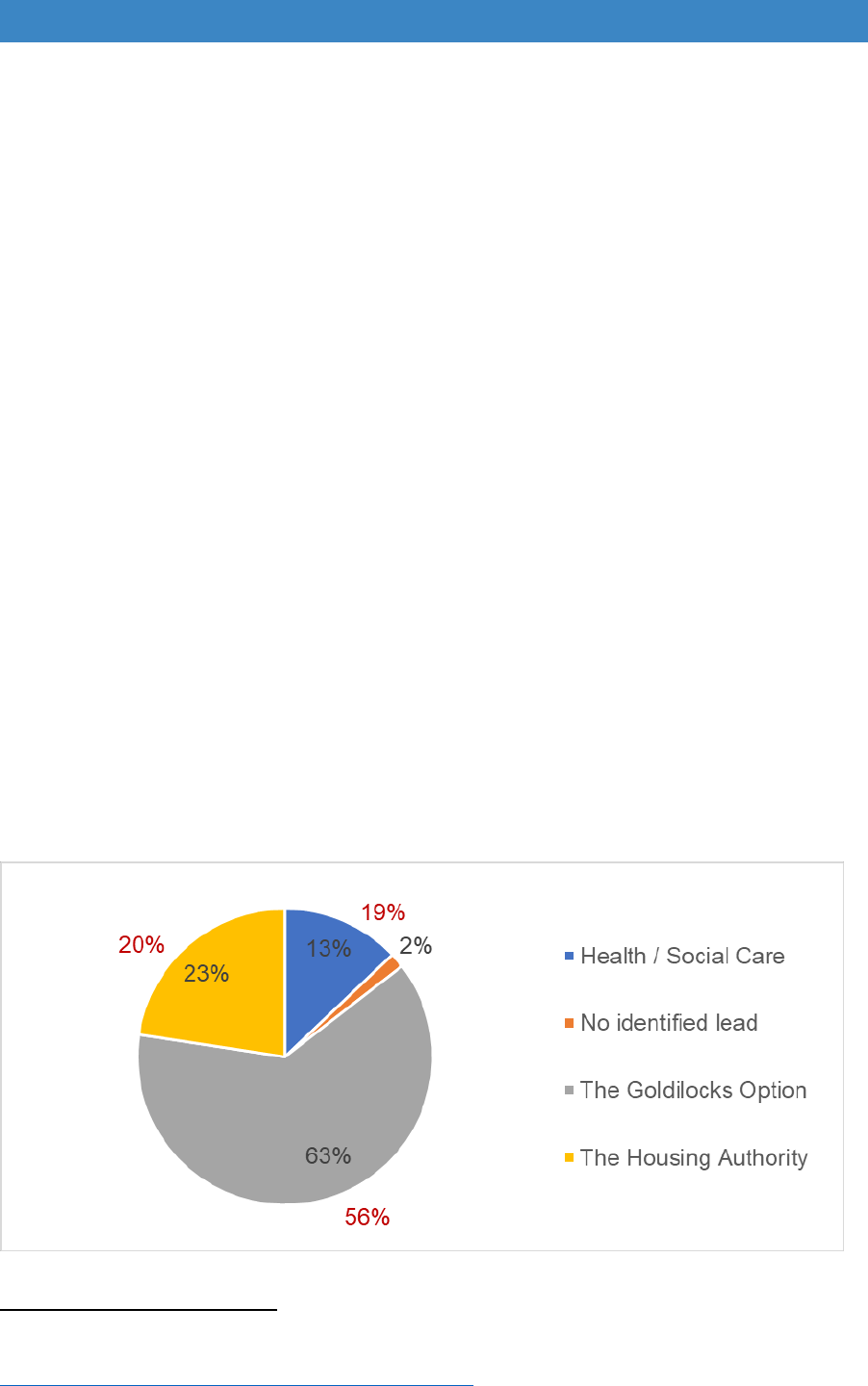
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
was at the heart of this very positive outcome”. Scottish Government
(2017) Evaluation of Adapting for Change, p.18
77
.
“Effective partnerships allow delivery organisations to make the best use
of their resources to maximise impact and value for money. To be truly
effective, organisations should therefore seek to align activity and work
in partnership.” Wales Audit Office (2018) Housing Adaptations
78
.
The options for strategic oversight
9.14 The consultation process for this review focussed on four options for strategic
oversight: having no identified lead as now; the housing authority being the lead;
health and social care being the lead; or a partnership of housing, health and
social care. This latter option was termed the ‘goldilocks’ option because it
appears to be the only one that brings all the key players together. In the
goldilocks story there were three bowls of porridge, one that is too hot, one too
cold and another that is ‘just right’. In this situation, if housing or social care take
the lead, it could perpetuate service divisions. However, bringing in health
creates a more balanced ‘just right’ solution.
9.15 Almost two thirds (63%) of those at the workshops thought the ‘goldilocks’ option
should be the way forward, although slightly fewer (56%) of those providing
returns online favoured this option. The other alternatives were either housing or
social care as the lead, with slightly more favouring the housing authority,
particularly at the workshops (23% for housing compared to 13% for social care)
(Figure 9.3).
Figure 9.3 Options for strategic oversight
Source: voting at consultation events / online survey
77
Scottish Government (2017), ibid.
78
Wales Audit Office (2018) Housing Adaptations, Cardiff: Wales Audit Office.
http://www.audit.wales/publication/housing-adaptations.
81
Disabled Facilities Grant (DFG) and Other Adaptations: Main Report
9.16 Table 9.1 outlines the advantages and disadvantages of each option. There were
a lot of written comments in response to the online survey about the issue of
strategic oversight, with the majority (118 responses) commenting about the
‘goldilocks option’. Most respondents said that housing and social care need to
work together to facilitate integrated solutions alongside health. There was a
strong feeling that housing must be the key partner at strategic and operation
level, and that the housing authority needs to be a statutory member of HWBs.
However, many respondents added the caveat that it was not always easy to get
joint working and that it requires strong leadership.
Responses to the online survey about partnership working
“In our authority, a specialist service was created 20 years ago where housing and
social services were brought together to work together on adaptations. This has
proved hugely successful. We all now sit under Social Care and will be integrating
further with the NHS from 1st April 2018.”
“I accept (as a Housing Authority) that Social Care have a huge part to play in the
system. Bringing the two tiers together in this way (and at an operational level too) has
great benefits.”
“Collaboration and an integrated service are the only way to streamline the process.”
“No one department has statutory responsibility for, or knowledge of, all parts of the
process of providing housing and adaptations that are fit for purpose. Collaboration
and effective strategic partnership is only effective way forward.”
“No single organisation has all the necessary skills to oversee this - a partnership
approach if managed effectively works very well - although it has its challenges and
relies on individuals to make it work”.
“It seems like a fairy tale that such an approach could be possible because of everyone
protecting "their own" budgets but actually if the decision makers/budget holder’s
hands were forced to work together by a change to the strategic oversight then in the
longer term I think this would be the best outcome for all parties.”
“There needs to be a holistic, whole house approach to assessing a person's needs
and so we cannot get away from the need to involve both the housing and social care
sectors in strategic oversight.”
“Goldilocks solution is best as it encourages consideration of the most appropriate
solution to meet needs. In some cases rehab/re-ablement/equipment/rehousing would
be a more appropriate way to meet presenting need.”
“I've worked in a two-tier authority and currently for a unitary managing the DFG
programme. Neither system appears to work properly, there are still silos. The
Goldilocks Solution appears in principle to be a way forward, subject to Management
"buy in" and accountability.”
“This option has the potential to be confusing though and will need very clear roles
and leadership if it is to be successful and improve upon current processes and
timescales for delivery. The devil of this will be in the detail and that could benefit from
very much more unpicking and consultation.”
82
Table 9.1 Four options for strategic oversight
Lead
authority
No identified lead
Housing authority
Health and social care
Partnership -
‘goldilocks’ option
Continue as at present with
no oversight of the whole
DFG process.
Advantages
Has the statutory duty for the
DFG and already oversees
home adaptation
programmes.
Care Act responsibilities for
disabled and older people -
and under the Children Acts
for disabled children
Formal strategic partnership
between housing, health and
social care
Retains link to other housing
services - housing options,
private housing,
homelessness and planning.
Link to equipment and minor
adaptations provided by
ICES funding and to other
aspects of care in the home
Oversight and co-ordination
of adaptations, equipment,
housing options, planning
etc.
Directly benefits from
investment in adaptations
and could more clearly
develop a business case for
expensive adaptations.
Recognises the knowledge
and expertise that each
contributes
Already covers county areas
- would not require another
layer of strategic
management
Maintains the housing
authority as the lead with
statutory duty for the DFG
but involves all key players
Disadvantages
Complex process, varies
between authorities, high
drop-out rate and often slow.
More difficult to develop links
to equipment, minor
adaptations, telecare and
care services for disabled
and older people.
Would not have such clear
links to housing and
planning policies
It involves the creation of a
new layer of strategic
oversight
Although the housing
authority provides the
investment it does not
receive any direct financial
benefit
Health and social care under
considerable financial strain
– have more pressing
concerns than the DFG.
Concern that DFG budget
would be ‘swallowed up’.
Would require housing to
have a more major say in
the BCF and HWBs.
9.17 Consultation with the national organisations representing local authorities gave
a largely positive response to joint working. A County Council’s Network
representative said that they would like to see a single policy across county and
unitary authorities based on the needs of locality with the policy reviewed
annually to ensure flexibility and adjustments of budget allocations and priorities.
The Association of Directors of Adult Social Services (ADASS) referred to the
Secretary of State for Health’s seven principles for reforming adult social care
which includes ‘whole person integrated care’ and said that, “delivering a
seamless service that wraps around the individual requires greater coordination
and strategic leadership across social care, health and housing across every
local authority area.
9.18 The Local Government Association added that “councils must have the flexibility
to ensure that funding can be directed towards meeting the health and care
needs of their residents, without overly prescriptive national requirements which
might adversely affect local impact and innovation.” Councils will want to ensure
that BCF plans support housing as a central component in improvements in
people’s health and wellbeing with a shift to a more preventative approach, and
HWBs need to be fully involved in shaping, approving and monitoring plans.
9.19 The only organisation not in favour of a ‘Goldilocks’ partnership option was the
District Council’s Network (DCN). They were supportive of models which
increase the efficiency of the DFG locally and were person centred. However,
they felt that the housing authority was best placed to take the lead on
preventative action because of their statutory duty, the range of housing services
they deliver and their role in community leadership. If districts were to be part of
a county-wide body, there was “potential for funding to be subsumed into the
acute end of social care.” They felt that oversight sitting with HWBs would not be
appropriate, as they covered much larger areas and would not be able to respond
to the needs of each locality. They were also concerned about adding another
layer of bureaucracy and about the potential burden on staff of having attend
meetings and deal with the administration.
Making partnerships work
9.20 The transformation work relating to home adaptations in Scotland shows that any
partnership approach is not easy, and that it is hard for partners to let go of the
way things have always been done.
“The need to improve adaptations services is a longstanding one, but
also an area in which truly transformative change has been very
difficult to deliver. The need for sustained partnership working
between a range of key services was generally seen as being the
single greatest challenge”. However, “even when progress has been
slow, there have been some signs of attitudes changing even in the
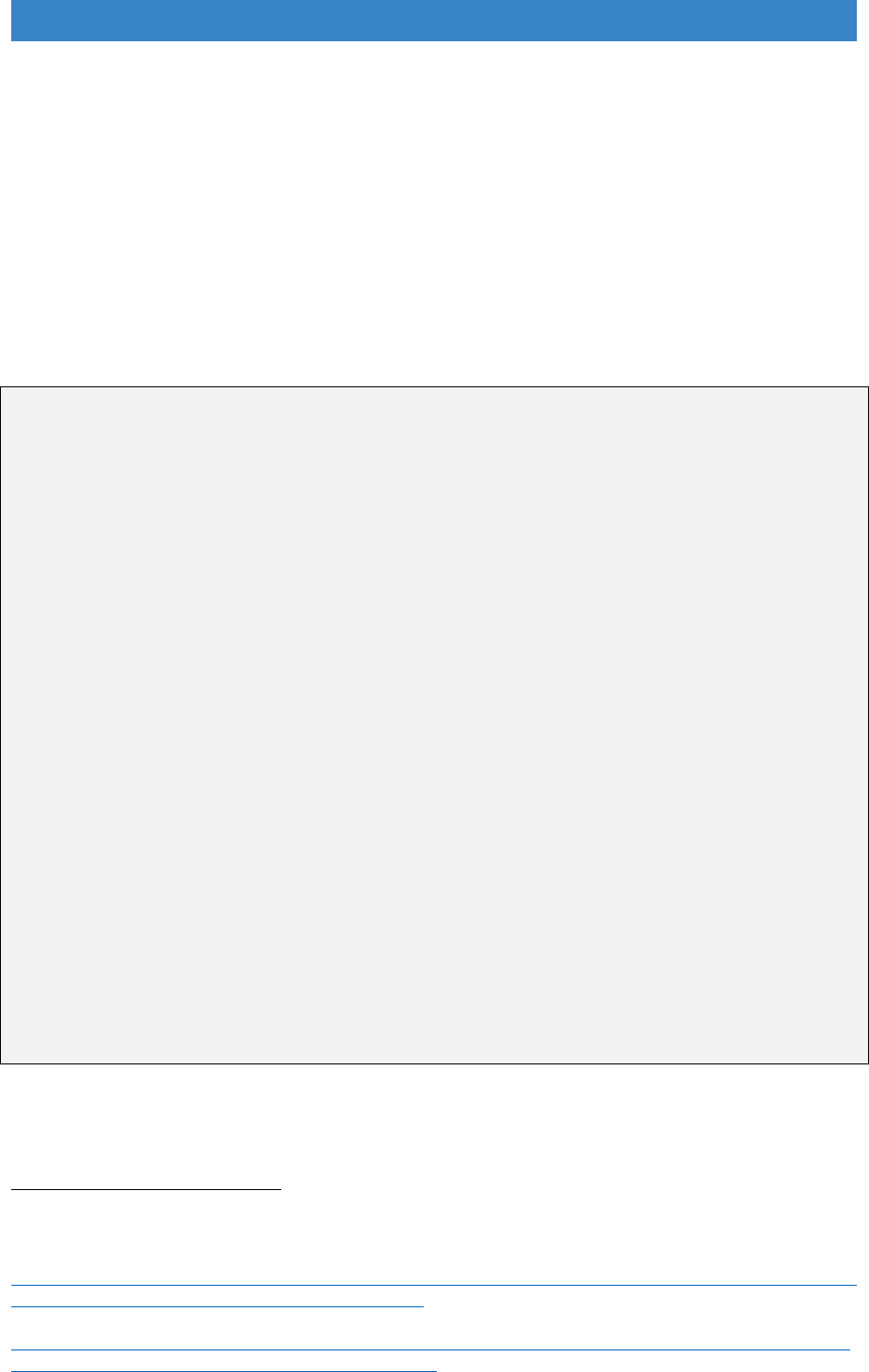
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
latter stages of the AfC initiative” Scottish Government (2017)
Evaluation of Adapting for Change
79
.
9.21 Some areas already have a form of partnership board such as Leicestershire,
Lincolnshire and Worcestershire. A national requirement for these types of
partnership arrangements, perhaps called a ‘Housing and Health Partnership
Board’ would encourage their development and strengthen the functioning of
these boards.
Existing partnership boards
Leicestershire Lightbulb Programme – is managed by the Lightbulb Programme
Board and a Steering Group made up of stakeholders from district, borough and
county councils
80
. In the pilot phase, employees were managed by Blaby District
Council, but the full service includes an integrated locality team in each district.
Funding is pooled, and a central hub provides management support, performance
monitoring and service development. The Programme Board and Steering Group were
critical to developing the model and funding approach across all the partners.
Lincolnshire Housing Health and Care Delivery Group is a county-wide formal
partnership between housing, health and care and reports to the HWB. This provides
strategic oversight of DFG policy. It has already had successes in improving the
delivery of DFG's and would be the most appropriate way of moving forward.
(Response to online survey).
Worcestershire Strategic Housing Partnership – is a county-wide board
responsible for co-ordination, commissioning and securing funding for new projects
and supporting business as usual. Its priorities are to: a) improve homes and,
“transform places”; b) drive the growth of the right type of homes; and c) create a
partnership approach to enable people to live as independently as possible through
prevention and early intervention. It is supported by five delivery groups, one of which
is about independent living. The partnership is underpinned by a local Housing
Memorandum of Understanding
81
.
79
Scottish Government (2017) ibid.
80
Moran, A. (Jul 2017) The Lightbulb Project: Switched on to integration in Leicestershire, London:
Housing LIN.
https://www.housinglin.org.uk/_assets/Resources/Housing/Practice_examples/Housing_LIN_case_stu
dies/HLIN_CaseStudy_135_Lightbulb_Project.pdf.
81
Worcestershire Housing Partnership Plan 2017
http://moderngovwebpublic.redditchbc.gov.uk/documents/s27809/170322%20Final%20Worcestershir
e%20Housing%20Partnership%20Plan%2011d.pdf.
85

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
9.22 One option for the establishment of Housing and Health Partnership Boards
would be to use a similar structure to Local Safeguarding Children’s Boards
(LSCBs). This would need to take account of the findings of the review of LSCBs
and look at the flexibility in their composition
82
.
National level oversight
9.23 To make partnership working a reality, central government will need to ensure
that a new strategic structure is established as a requirement of DFG funding.
The Ministry of Housing, Communities and Local Government and the
Department of Health and Social Care will also need to work together to issue
guidance about the role of the DFG in the BCF or any successor body after 2020.
9.24 Governance arrangements should be aligned to the process of setting BCF
budgets and plans, with Clinical Commissioning Groups, District Councils and
County Councils as signatories, ultimately signed off by the HWB.
9.25 Requiring the BCF and HWBs (or any successor bodies) to report on a metric
that relates to DFG outcomes such as ‘the number helped to remain
independent at home’ would focus attention on the importance of adaptations
and ensure that more weight was given to the DFG in both strategic planning and
in reporting of outcomes and impact.
Cultural change
9.26 It is not just about new strategic structures and government regulation. It is as
much about cultural change. There are key people in housing authorities and in
occupational therapy roles who have spent their lives delivering the DFG. They
are some of the most dedicated staff working in the public sector. But it is hard
to let go of well-established ways of working. There has already been a lot of
reorganisation in local authorities due to austerity, and no additional revenue
funding was provided when DFG capital resources were increased.
9.27 Staff will need support to understand what will happen and to be involved in
developing new ways of working. However, it is unrealistic to expect them to
maintain day to day DFG delivery while at the same time moving to new, more
integrated ways of working. Transformation funding and strong leadership
support will also be required. Transformation funding is discussed further in
Chapter 13.
82
HM Government (Mar 2015) Working Together to safeguard children: A guide to inter-agency
working to promote the welfare of children, Chapter 3: Local Safeguarding Children Boards.
http://www.workingtogetheronline.co.uk/chapters/chapter_three.html.
86

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Recognising the broader role of the DFG
9.28 A partnership board could also allow more holistic, person-centred decision-
making. Up until now, the DFG has been largely about fitting showers, stairlifts
and ramps. Minor adaptations under £1,000 are delivered separately through the
ICES budget, and additional needs, such as telecare, done by other
organisations. Decision-making relating to more complex and expensive cases
has been hampered by a cost of ceiling of £30,000 that has been too low to
deliver effective solutions.
9.29 A stronger focus on helping someone be as independent as possible, wrapping
services around the individual and reducing strain on carers, can result in new
combinations of work and has the potential to draw in other sources of funding
alongside the DFG. Drawing together DFG and ICES budgets into the same
funding pot (either the BCF or its successor) will be essential.
Wider prevention – this includes determining local needs, working with other
organisations to ‘Make every contact count’ to identify people struggling with
their homes before they get to crisis point and looking at the whole situation in
the home to provide holistic services.
Short-term interventions - rapid response services to enable someone to
come out of hospital or to prevent someone in crisis having to go into residential
care by fixing trip and fall hazards, installing minor adaptations, repairing the
heating system and providing an immediate deep clean and declutter.
Medium-term solutions – typical DFG provision such as stairlifts and showers,
but with a range of integrated services to maintain independence which might
include: minor adaptations such as grabrails, key safes; a personal alarm
system; other improvements such as repairs or a new heating system; and links
to an exercise class or befriending service to improve health and wellbeing.
Solutions for people with long-term needs – may require different solutions
and joint working could provide a business case to consider likely health and
care savings and draw in funding from other sources including the ICES,
wheelchair and telecare budgets.
The need for person-centred services
9.30 As Heywood said in 1994 “’good practice’ means ‘good’ from the point of view of
those who need adaptations; the users”
83
. It is not just about what is expedient
from the vantage point of policy makers and service commissioners; it needs to
be seen from the customer’s perspective.
83
Heywood, F. (1994) Adaptations: finding ways to say yes, Bristol: SAUS Publications, p.7.
87

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
9.31 There is some use of focus groups and a few authorities involve users in
meetings. However, during the discussions in this review, it was noticeable that
very few authorities have carried out service transformations using co-production
techniques with the client groups they aim to serve or have user scrutiny groups
to drive further service improvements. In addition, few have a policy to directly
employ people with impairments who can bring a different perspective to the
service. Middlesbrough is an exception; their handyperson team is made up of
disabled people
84
.
9.32 The place that we are aware of that went through the most comprehensive
consultation with disabled and older people prior to transforming services is
Knowsley
85
. This resulted in the establishment of a one-stop shop for all services
related to disabled and older people including: assessment facilities for adults
and children; equipment supply, recycling and repair (including wheelchairs);
demonstration space, and the DFG, minor adaptations, HIA and handypersons
services for all tenures all under one roof. They also set up a user board which
continues to operate. Many of the places that have developed integrated services
discussed in the next chapter, such as Leicestershire, have included consultation
as part of service planning.
9.33 It is recommended that as part of the process to decide which options in this
review might be best to take forward, that disabled and older people, their
families, carers and organisations that represent them, are fully consulted.
Guidance needs to be issued about co-production and consultation techniques
to develop integrated local services.
Providing more choice by engaging with housing providers
9.34 At present the DFG is mostly about providing adaptations to a disabled person’s
existing home. However, moving might provide a much better solution,
particularly where extensive adaptations are required or where a home is in poor
condition. A new partnership board should bring in other housing providers and
planners. This would improve local development and customisation of new
accessible homes. It would also improve rehousing options by developing
adaptation strategies with landlords, aid the establishment of accessible housing
registers, and provide more effective matching of disabled people to existing
adapted properties. It could also bring more funds into the DFG if registered
providers contributed more to DFG funding. This is discussed further in Chapter
17 on tenure.
84
Mackintosh, S. and Collingbourne, L. (2016) Home Adaptations for Disabled People Good Practice
Case Study: Middlesbrough. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-
of-good-practice-middlesbrough-staying-put.pdf.
85
Mackintosh, S. and Collingbourne, L. (2016) Home Adaptations for Disabled People Good Practice
Case Study: Knowsley. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-of-
good-practice-knowsley-centre-for-independent-living.pdf.
88

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
What should the grant be called?
9.35 During many conversations we had in carrying out this Review, it became clear
that the term DFG is synonymous with the function of funding the installation of
ramps, stairlifts and level access showers. This was often unhelpful when trying
to develop discussions about more person-centred support and more flexible use
of the grant. In addition, potential recipients of the grant do not always want to
be labelled ‘disabled’, they don’t necessarily understand the word ‘facilities’ and
even the word ‘grant’ may have paternalistic connotations.
9.36 In the 2005 review it was suggested the name be changed to the ‘Accessible
Homes Grant’ which got considerable support. However, the name Disabled
Facilities Grant is defined in legislation which means that changing it is not easy,
and it was not taken forward at that time
86
.
9.37 A number of authorities have used the opportunity of developing their RRO policy
to change both the name of the grant and their service. But there is little
consistency. Accessible Homes, Lightbulb, Home Solutions, At Home, Healthy
Housing, Safe at Home, Care and Repair and Staying Put are just a few of the
options in use across the country.
9.38 If we want services to be preventative, we need to ensure that disabled and older
people and their families and carers are aware that advice, information and
sources of funding are available to help them modify their home. There needs to
be more consistency in what services are called. A new national advice service
is also needed which should use the same name and branding so that all services
dealing with adaptations and accessible homes are instantly recognisable. Home
Independence Fund/Grant/Service or Home Adaptation Fund/Grant/Service are
just two possible suggestions.
9.39 Services should not just be aimed at older people but recognise that there are
more people with disabilities of working age than there are in later life, and that
families with disabled children are also in need of help. Giving services a more
youthful image will also appeal to the generation of people aged 50-70 who do
not think of themselves as being ‘old’.
9.40 The lack of a national brand makes it very difficult for relatives based in other
local authority areas to know where to turn to help family members who are
struggling with their homes. It is also very important for other professionals in
health and social care to know where to signpost patients and service users.
Many of these professionals do not know about or understand the DFG, which
means that prevention opportunities are being missed.
86
Department for Communities and Local Government (2008) Disabled Facilities Grant: Package of
changes to modernise the programme, London: DCLG.
http://www.communities.gov.uk/documents/housing/pdf/dfgpackagechange.
89

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
9.41 Choosing a new name is much more than renaming and rebranding; it underpins
an entirely new approach to adaptations and integrated service delivery to help
people live independently at home. It needs to be focussed on prevention and
have a youthful image which is immediately recognisable and well-known.
Recommendations - strategic oversight
A Housing and Health Partnership Board to be established in each area as a
requirement of DFG funding with representatives from housing, health and
social care.
Each BCF and HWB to report separately on DFG funding and on a new metric
on ‘the number of people helped to remain independent at home’.
Housing and Health Partnership Boards to have a similar structure to Local
Safeguarding Children’s Boards.
The DFG and ICES budgets to be in the same funding pot (the BCF or its
successor) to join up DFG services with equipment provision and minor
adaptations.
A single adaptations policy to be developed for each area, based on the
needs of the locality, reviewed annually and signed off by the HWB.
A new name for the grant, the services that provide it and the national advice
organisation, and for that name to be used consistently across the country.
90

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 10. Local delivery
10.1 The aims of this chapter are to look at how local DFG delivery can change, and
to give practical examples of places that demonstrate ‘what good looks like’.
Services are continually evolving and, although no area can be said to have got
everything right, some now have very effective services.
10.2 Most services have not had access to transformation funding, they have had to
adapt services at the same time as continuing with business as usual.
Sometimes restructuring has been fragile when the integration of health and
social care services, with their vastly bigger staffing numbers, has unwittingly
undone changes made to improve the much smaller adaptation service.
Austerity and loss of staffing resources have compounded these problems.
10.3 Despite the constraints, many areas show that you can make substantial
changes to improve the customer journey. By using the flexibilities given by the
Regulatory Reform Order 2002, it is possible to provide a much broader range
of services. These comply with the 2014 Care Act, Better Care Fund targets
and the overall requirements of the integration agenda, while most importantly,
giving consumers the streamlined, fast and flexible service that they require.
The need for integrated teams
10.4 As Section A showed, most authorities operate ‘traditional’, non-integrated DFG
services. In the ‘traditional’ process, referrals come into social care call centres,
assessment is carried out by social care occupational therapists, before cases
are passed to the DFG team in the housing authority for the means test, grant
application, preparation of specifications and plans, and practical help with
building and installation work. In the shire authorities, social care services
usually sit at county level and housing at district level. But even in unitary
authorities, the social care call centre and occupational therapy service are
often in different departments from the DFG housing team. In some areas, part
or all of the process is handled by an independent home improvement agency.
10.5 At the consultation events, 85% wanted an integrated service. Slightly more of
the online respondents wanted to keep the traditional service (most of these
were based in housing authorities), but even online, three quarters (76%) voted
for an integrated process (see Chapter 7, Figure 7.3).
91
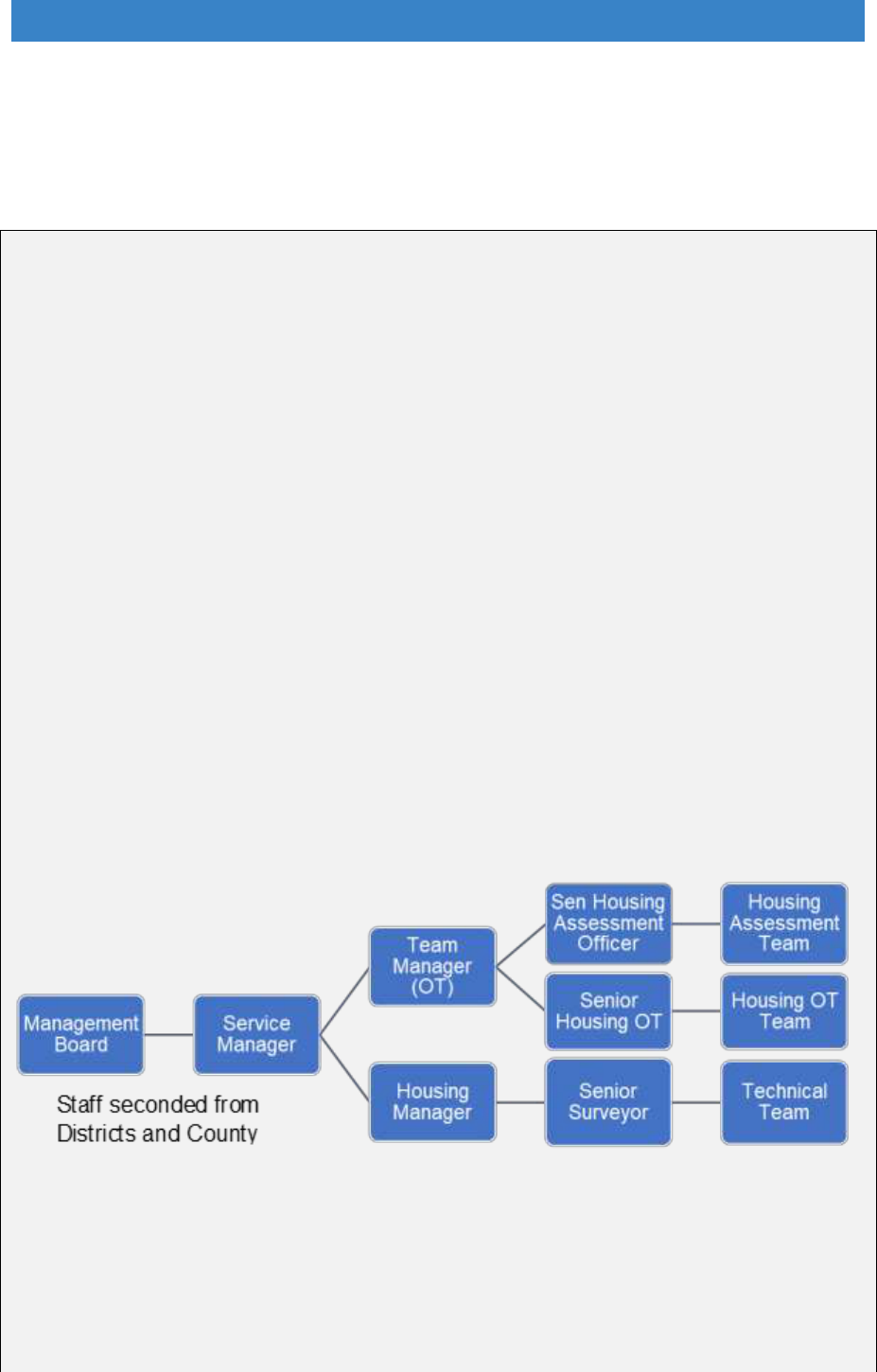
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
How an integrated team works
10.6 To illustrate what integration means in practice, the simplest way is to show
some examples.
HEART - The Home Environment Assessment & Response Team
The Home Environment Assessment & Response Team (HEART) in Warwickshire is
a partnership between the county and district councils.
Five years ago, the county and districts had competing priorities for the DFG with no
overall control of the process. The result was multiple teams all with their own
managers, with numerous access points and waiting lists. They mapped the customer
journey and found that it was a 220-step process where 35% of people dropped out
along the way.
The new service was originally set-up as a pilot in one of the districts, but it is now
operating county-wide. Staff have been seconded from district and county authorities
into two teams, one operating in the south and one in the north of the county, each
with a similar structure (Figure 10.1).
There is an overall service manager, a team manager who is an occupational therapist
supporting a housing assessment and occupational therapy team, and a housing
manager supporting a technical team. The housing assessment officers are trained to
combine the skills of a caseworker, occupational therapy assistant and grant officer
which means only one person is needed to follow straightforward cases through from
enquiry to completion.
Figure 10.1 Integrated team structure
Five years since the first pilot they have a 22-step process, a fully integrated team and
a drop-out rate of just 3% (Table 10.1). There is a shared understanding of what they
are trying to achieve and a strategic direction. A single access point means enquiries
and referrals come directly into the service and can be routed to the person with the
right skills. More complex cases are directed to senior members of the team, but the
92
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
majority are handled by the housing assessment team. Time from first enquiry to
completion has reduced significantly and the average completion time is now six
months. In benchmarking against similar authorities, they were the fastest (Figure
10.2).
Table 10.1 Results of integration
Prior to integration
After integration
Multiple teams, managers, offices,
access points, waiting lists
Single access point and one contact
throughout the customer journey
Use of multi-skilled workers makes
single contact easier to deliver
Competing priorities, no overall
ownership
The team has a shared vision, goals
and strategic direction.
220 step customer journey
22 step customer journey
35% drop out rate
Dropout rate fell to 3%
Quicker end to end completion times
than equivalent authorities
Figure 10.2 Benchmarking end to end times - enquiry to completion
The aim is not just to provide standard DFGs, but to give advice and assistance to
deliver disabled adaptations and home improvements that keep people safe, secure
93
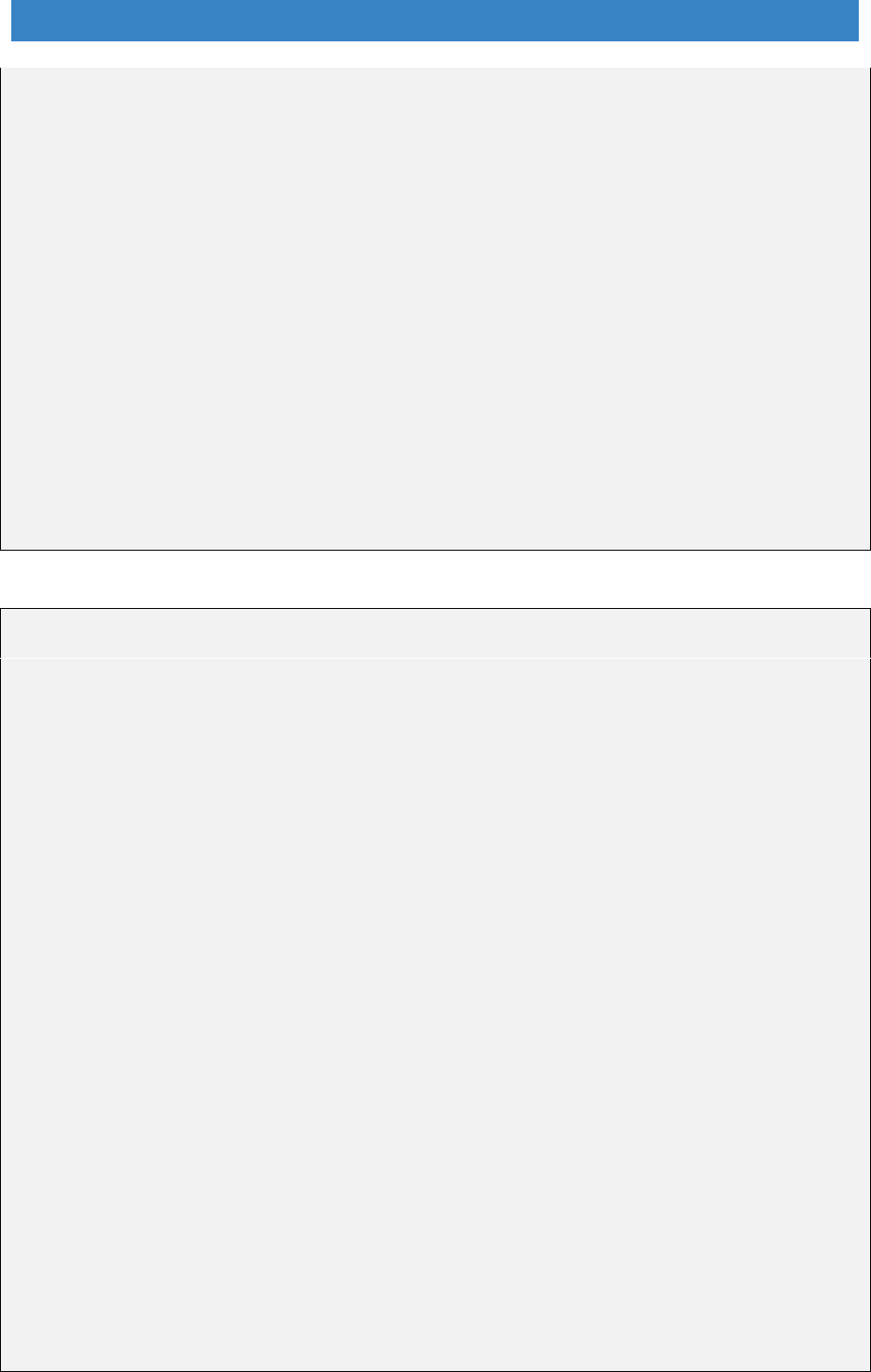
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
and warm in their own homes. HEART provide smaller equipment and adaptations,
like bath boards and stair rails, help with general repairs, and advice and support to
move where this is a better alternative. They recognise that the DFG is a part of a
patchwork of funding and services that people need, and that a ramp or a stairlift in
isolation is unlikely to deliver the best outcomes.
In terms of revenue costs, the new approach appears to be cost neutral, but as 30%
fewer people drop out they are delivering more cases for the same money. The
result is that Warwickshire, as a county authority, is now far more integrated than
many unitary authorities.
Transformation lessons:
Disagreement is inevitable - there will be disagreement in any partnerships -
senior leadership teams recognised that working together was the only way to
meet the needs of residents.
It takes time - to pilot new processes, train staff and embed the changes.
Dorset Accessible Homes Service
Dorset is a rural county with an ageing population. They realised that services
needed to change to meet the demographic challenges and went through a two-year
process of consultation and restructuring. Their integrated service went live in April
2015 covering six districts and two boroughs. The urban area of Bournemouth and
Poole has retained its own separate service.
The Dorset service is delivered by co-located teams from two offices in Dorchester
and Blandford Forum. It combines the ICES and DFG budgets to provide: advice and
information, alternative accommodation options, assistive technology and telecare,
minor repairs and adaptations, major adaptations, a handy van service and a safer
home initiative. There is also a fast track service to facilitate hospital discharge.
The benefit is a seamless, joined-up approach to service delivery between partner
agencies. It is preventative as people can self-refer into the service. They get a
choice of options at an early stage, the support to exercise that choice, quick
delivery, a single point of contact, and good feedback about progress.
The service has two ‘Mi-life centres’ where people can see and try bathing and
shower products, a stairlift, an adapted kitchen, furniture, home equipment, mobility
equipment, telecare and assistive technology products. This is complimented by
frequent pop-up events across the county to raise the visibility and awareness of the
service and what solutions are available - delivered by a mobile demonstration
vehicle with clinical staff.
A bespoke IT system provides secure data transfer and allows staff to see the whole
customer journey. It also allows effective outcomes and performance measurement.
94
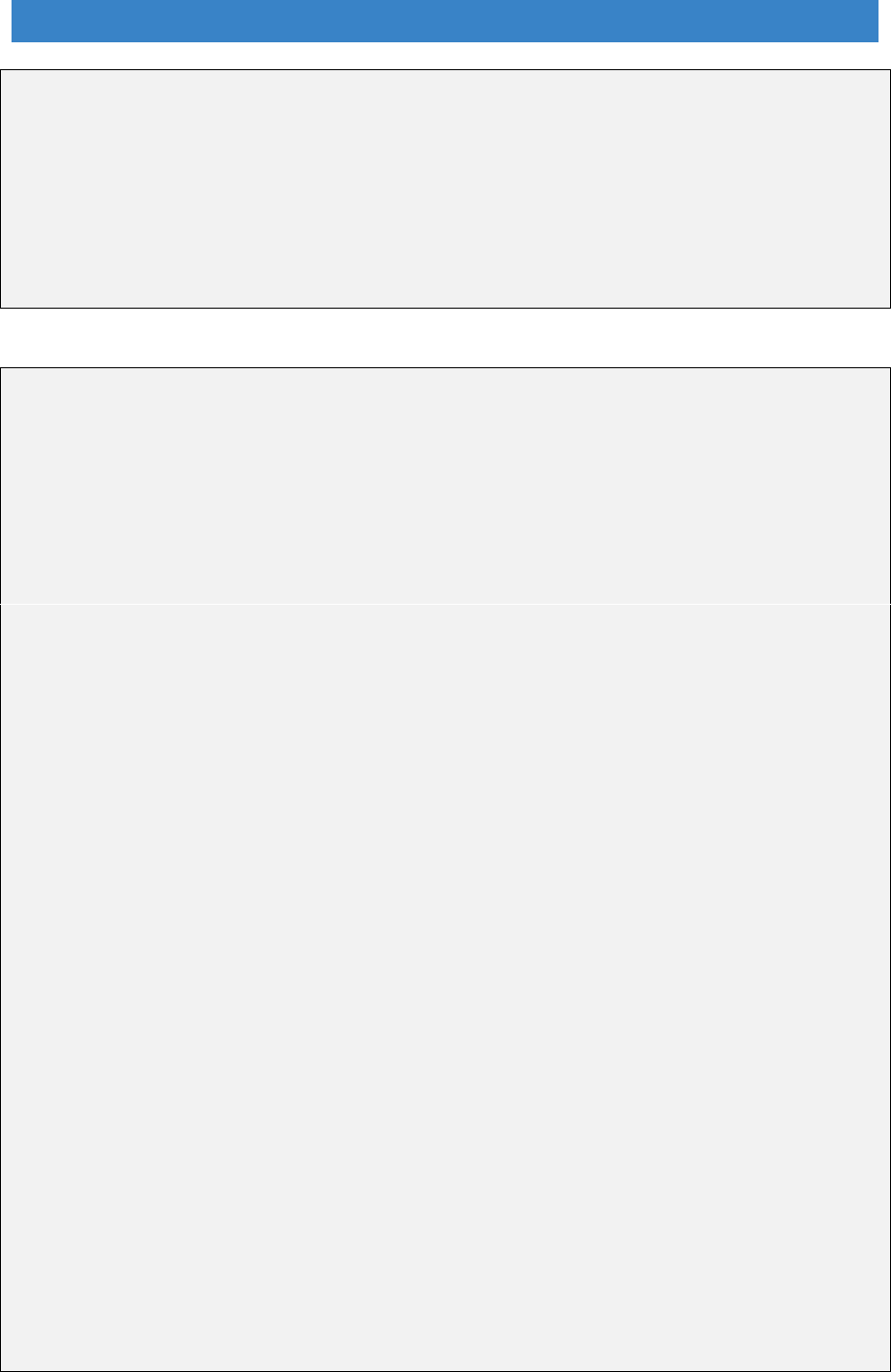
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Transformation lessons:
Communication - with so many organisations involved it is important to check
that messages are reaching everyone and that those messages are understood.
Cultural change - new ways of working, pooled budgets and use of trusted
assessors may all be resisted.
Understand partner’s needs and motivations - and be aware of other changes
going on elsewhere as part of the integration of health and social care.
The Leicestershire Lightbulb project
The Lightbulb model aims to save time for customers and provide efficiencies for all
the organisations involved. The original process for assessing and installing a stairlift
had 24 stages with 8 handoffs which is now 9 stages with only 2 handoffs. Assessing
and installing a level access shower had 27 steps and 9 handoffs which has been
reduced to 13 stages and 5 handoffs.
They obtained a £1m Transformation Challenge Award from MHCLG which allowed
development of pilot projects which have now been rolled out across the county. It is
delivered through a ‘hub and spoke’ model:
Each district council has an integrated locality team offering: minor adaptations and
equipment, DFGs, other housing support such as warmth, energy efficiency and
home security, assistive technology and falls prevention, housing options advice,
and other housing related advice, information and signposting.
A central hub provides management support, performance monitoring and
development support.
Similar to HEART they created a new role of Housing Support Co-ordinator
combining technical and casework skills to provide one point of contact for
customers.
A ‘Housing MOT’ provides customer focussed assessment and solutions.
They also work with other organisations such as community fire and rescue who
carry out home safety checks.
A Hospital Housing Enabler Team based in acute and mental health hospital
settings helps resolve housing issues that are a potential barrier to discharge and
provide low level support with the transition home.
A ‘Lightbulb funding pot’ combines existing resources across adult social care and
district councils, including the DFG. Staffing levels are based on analysis of need
across the county and assumptions about any increase in demand relating to the new
service offer. Delivery costs, including the Hospital Housing team, are approximately
£1m per year compared to a potential £2m per year saving to Leicestershire and the
wider health economy.
Transformation lessons:
Clear communication – this is vital
95
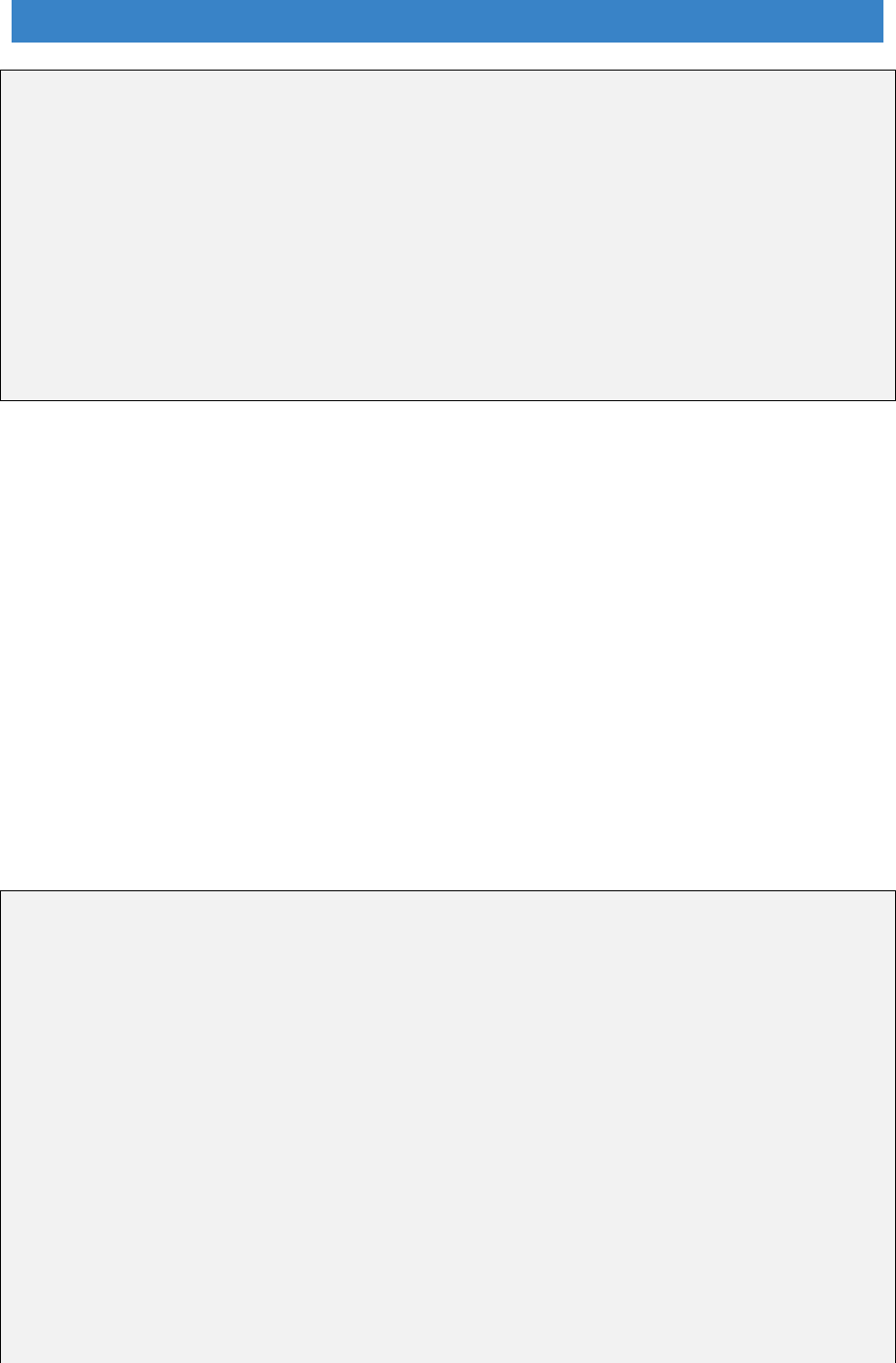
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Be prepared to work across boundaries - structural, administrative and
geographical.
It needs active leadership from partners who should meet regularly to oversee
the project, provide strategic direction, sort issues and remove barriers.
Get agreement on information sharing and how to deploy IT
Robust performance monitoring and reporting is essential to demonstrate the
impact of the project, generate ‘buy-in’ and help obtain secure funding.
Everyone needs to be flexible
It takes time and tenacity - once people begin to see results and benefits the
new service can really start to develop.
10.7 The examples above are all from county authorities and show what can be
achieved when DFG services that were originally split at district and county level
are brought together. The transformation process should be easier in unitary
authorities, but there are still barriers when services are divided between social
care and housing.
10.8 It is useful to look at how this has been achieved in Salford because it illustrates
what can happen as health and social care become more aligned. Here the
adaptation service was already integrated as it was based in social care, but it
has now moved to health. This has allowed different services supporting
disabled people to be brought together in a way that makes much more sense
for the customer. This is a model that may work in other areas going through a
similar process of merging of health and social care.
Salford Accessible Accommodation Team - transformation and
integration
Salford Care Organisation - part of the Northern Care Alliance NHS Group
Background: In July 2016 Salford City Council Adult Social Care (ASC) services
transferred into Salford Royal NHS Foundation Trust to integrate health and social
care. This included the Accessible Accommodation Team (AAT) responsible for
managing and delivering adaptions for disabled people.
The AAT has been managed within ASC for several years and has a single Head of
Service responsible for Social Work, Adaptions, Community Services and Therapy.
The Principal Manager for AAT also manages the Occupational Therapy Service,
Equipment Services, Wheelchair Services and Care on Call Service.
There are other services co-located in the building alongside ATT. These are the
Sensory Team, Intermediate Home Support Service, Paediatric Services,
Community Rehabilitation Team, the charity Disabled Living and a private retailer
96
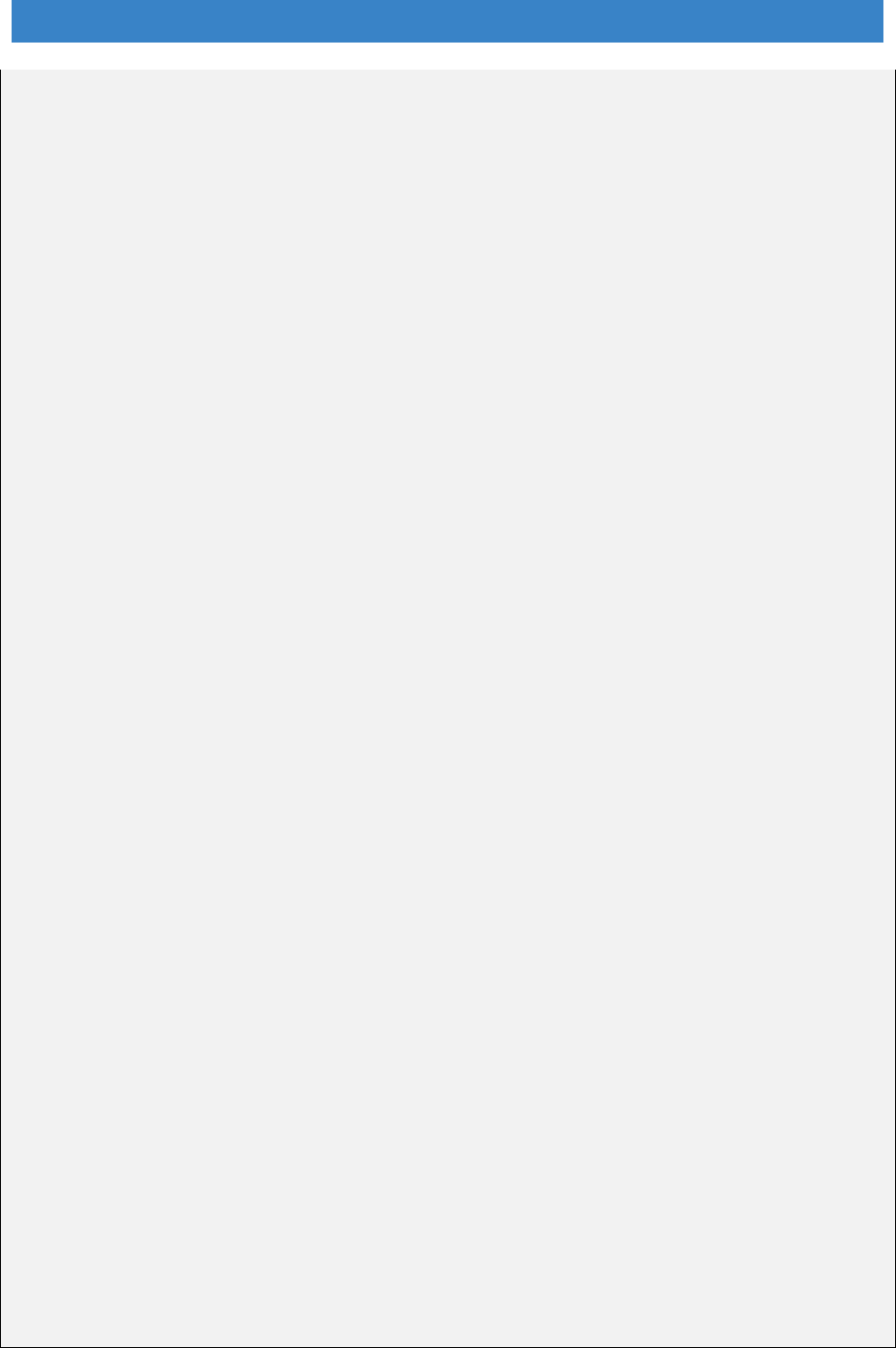
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Ableworld. This ensures closer working arrangements so that people with disabilities
have improved service provision and clearer pathways.
The ATT service works in partnership with a number of agencies including the local
handyperson service which installs grab rails and banister rails along with minor
home repairs and building maintenance works. Affordable warmth and heating
replacements are referred to the Local Energy Advice Program. The ATT can also
help residents access loan assistance through a commissioned provider regulated
by the Financial Conduct Authority.
Customer pathway and outcomes: The adaptations pathway has been
streamlined. Adult Social Care has developed a Centre of Contact ‘open referral
model’ supported by Customer Care Officers, Social Workers, and Occupational
Therapists. Health professionals such as District Nurses and Intermediate Care
Clinicians will eventually be included in this team. They provide information and
advice on the complete range of services. Adaptations are considered at the earliest
opportunity. The AAT service provides more specific advice and information on
adaptation work, specifications and suitable contractors.
The AAT is team is looking at their systems and processes to ensure the service
continues to be person centred. The prevention agenda is very important, and they
are working to improve outcomes for people that promote independence. They know
they need to capture more about health and wellbeing outcomes post intervention
and work is going on to develop a new outcomes model.
To ensure that people with disabilities have a voice, their views, aspirations,
strengths, problems and issues are discussed during the assessment process to
establish an accurate picture of their circumstances. This also involves talking to
carers, significant others and professionals. People also have access to an advocacy
service if needed.
Powers provided under the Regulatory Reform Order are reviewed periodically to
ensure assistance is flexible enough to deliver better outcomes for individuals and
supports the priorities of the Health and Social Care prevention agenda. A recent
example has been to increase access to adaptations to prevent falls.
Strategic management: Budgetary responsibilities are overseen by the Head of
Service who has a remit for a wide range of funding streams. This allows for other
funding beyond DFG to be considered when required, including community care
provision such as equipment, home support services and personal budgets.
There is a governance framework in place that ensures accountability and
transparency. This covers consistent management, cohesive policies, guidance,
processes, decision-making responsibilities and proper oversight by relevant
managers. The AAT service is governed by the Integrated Care Division Provider
Board, which is overseen by the integrated advisory board and committees from
Salford City Council, Salford Royal NHS Foundation Trust, Salford Clinical
Commissioning Group and relevant stakeholders.
97

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Key elements of integrated services
10.9 The key finding from these examples is that service integration, even across
large rural county authorities, is possible. There are different models, but they
have many elements in common including:
A strategic partnership board and a strategic plan.
Linked services using the ICES and DFG budgets, but with the potential to
include additional funding.
A single access point.
Integrated teams under a single manager which includes staff with
occupational therapy and technical skills.
A new cross-trained staff role combining trusted assessor, grant officer
and casework skills to provide better customer support.
An RRO policy to provide fast, flexible DFG solutions tailored to the needs
of the locality (this is discussed further in Chapter 15 Regulation)
Preventative services providing advice, information and housing MOTs.
A range of wrap-around services for the customer including: alternative
accommodation options, assistive technology and telecare, minor repairs
and adaptations, major adaptations, a handyperson service, energy
efficiency, a safer home initiative and a fast track services for hospital
discharge.
Effective end-to-end IT systems using bespoke systems and/or NHS
numbers and data sharing protocols.
Effective reporting on outputs, outcomes and impact and use of this
information to continually improve the service.
10.10 The results show that fewer people drop out, there are less steps in the
customer pathway, handovers are minimised, and services are much quicker.
Customers don’t get lost in the system but have a single point of access and a
contact person to call if they have a query.
10.11 It should be noted that the legislation still provides the right for people to make
an application in their own right. While this is a small minority, this right would
still remain.
10.12 Figure 10.3 shows the types of services that have been linked and given
strategic oversight to deliver more effective health and care outcomes.
98
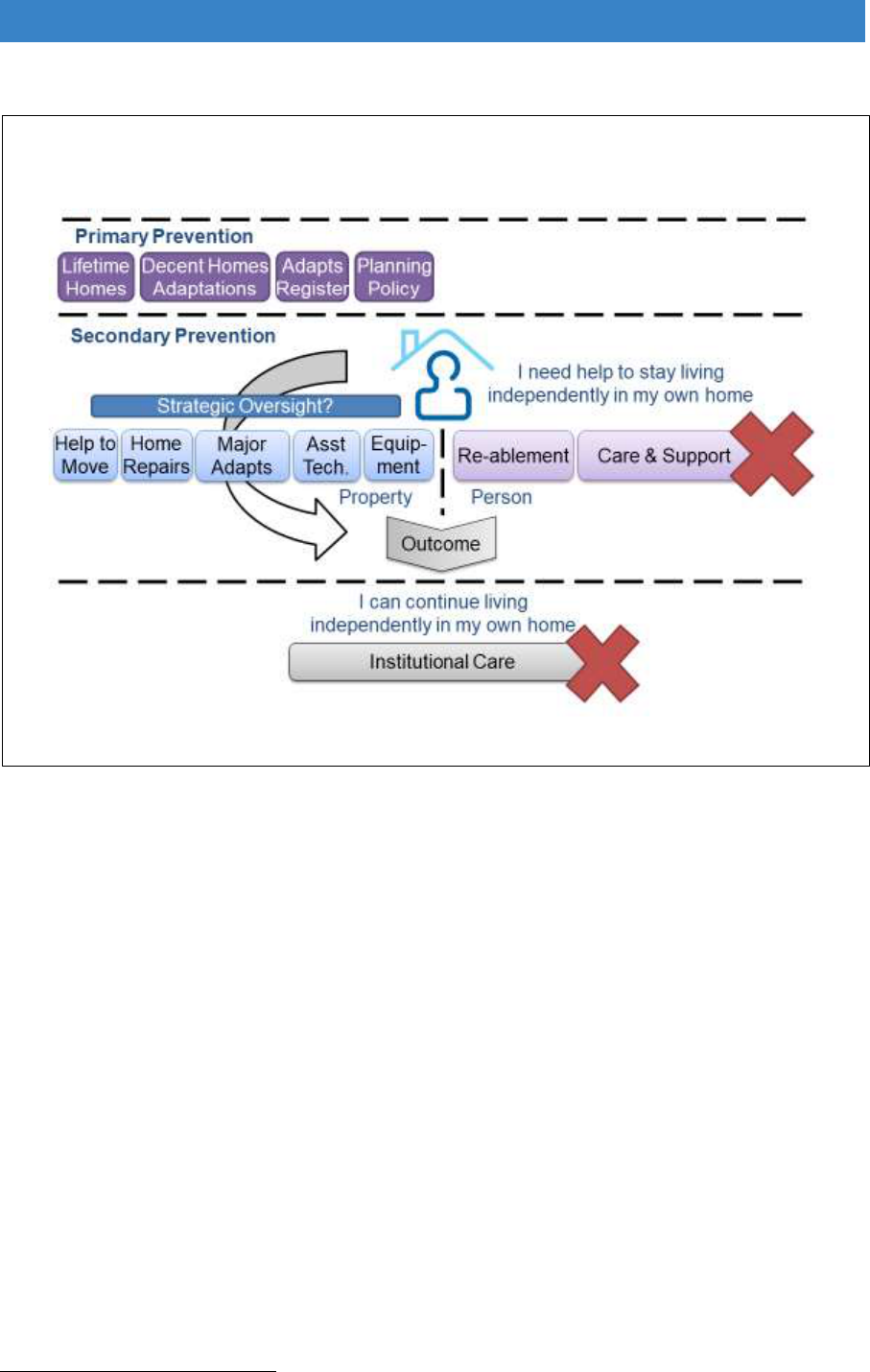
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 10.3 The outcomes of effective service redesign
National transformation fund
10.13 At the moment, integrated services are still the exception rather than the rule.
To drive change across the whole of England will require additional resources
for transformation. The limited number of staff currently providing DFG services
cannot be expected to deliver transformation while at the same time trying to
process more grants. There has got to be a way to allow business as usual to
continue while changes are made.
10.14 Integrating services is not an easy process. The transformation work in
Scotland showed that “The test sites have tended to find the change process to
be both more challenging and requiring a longer overall time period than
originally anticipated”
87
.
10.15 The pioneers such as Leicestershire’s Lightbulb had £1m in transformation
funding and they know they could not have changed the service without this
injection of resources. There is now a lot of learning to draw from, so the
87
Scottish Government (2017), ibid.
99

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
process may not be as hard for those just beginning to restructure. Costs should
also be less in smaller counties or small unitaries.
10.16 The LGA runs a Housing Advisor programme designed to support councils
seeking to innovate in meeting the housing needs of their communities. The
programme will fund adviser support for up to £14,000 to each council. This has
been calculated on the basis of 20 days at a set day rate of £700
88
. To provide
a similar level of support to all 326 housing authorities would cost £4.564m,
around 1% of the current national DFG funding allocation. Not every council
would necessarily need external support, but it does provide an indication of
the level of investment required to support the transformation of DFG delivery.
10.17 There is scope for secondments to allow the learning from areas with
successfully embedded integrated services to be passed on. There also needs
to be better guidance to allow effective service design to be copied in other
areas. The following chapter looks in more detail at different elements of
integrated service delivery.
Recommendations – local delivery
That integrated teams are established in all areas to simplify and speed
up customer journeys.
That a Home Independence Transformation Fund equivalent to 1% of the
national DFG allocation is provided to develop integrated services in all
areas.
88
Local Government Association (2018) Housing Advisors Programme 2018/19.
https://www.local.gov.uk/topics/housing-and-planning/housing-advisers-programme-201819.
100

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 11. Working better together
11.1 This chapter looks at the detail of integrated service delivery. It is divided into
a number of parts:
Establishing local need and handling referrals
Effective working
Delivering health and care outcomes
Data collection and reporting
Establishing local need and handling referrals
Finding people needing help with their homes
11.2 Most adaptation services do not look in detail at local needs, but simply base
forecasts on the previous year’s throughput of cases. Research with local
authorities across the UK found that most were unaware of unmet need for
adaptations. When setting the annual budgets, 78% of local authorities relied
on the previous year’s spending, and only 14% carried out surveys of need
89
.
This was an expedient policy to avoid the build-up of long waiting lists when
funding was limited but should not apply now that resources have increased.
11.3 A different approach is needed if the aim is to work better with health and social
care and be more focussed on preventative policies. There is a need to
intervene before people get to crisis point, by targeting people at risk,
preventing falls and accidents, and improving health and wellbeing.
11.4 Better strategic planning is required with the need for adaptations to be part of
Joint Strategic Needs Assessments (JSNAs). Lower income groups are more
likely to be disabled, have fewer years in good health in later life and may
experience frailty earlier. This requires good local data and mapping to show
where resources might be better targeted. It is then possible to work with
specific GP surgeries, community health providers, Fire Service home safety
check teams and local voluntary groups to find people who have had falls or
might be living in poor conditions.
11.5 However, people needing help with their homes are also scattered across local
authorities and other ways are also required to find those who need help before
they get to crisis point. Many will not be known to health and care services, as
most people have informal care or just struggle on for as long as they can.
Advertising has been minimal up to now. But once services are integrated and
able to deliver adaptations quickly and efficiently, there is more scope to
89
Zhou, W., Oyegoke, A.S. & Sun, (2017) Service planning and delivery outcomes of home
adaptations for ageing in the UK, M. J Hous and the Built Environ. https://doi.org/10.1007/s10901-
017-9580-3.
101
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
publicise the service. The following examples show different approaches to
finding people who need the adaptations service.
Oxford - Raising awareness of DFG services
Local authority in-house home improvement agency
Background: The service has a strong commitment to equality of access to a range
of services under its local assistance policy which includes support for home
adaptations. A broad-based campaign was enacted to raise awareness of available
services, both to the public, and a range of organisations and services in health, care
and the voluntary and community sectors.
Nationally there has been a reluctance to “advertise” support via Disabled Facilities
Grants as, until recently, the level of funding was insufficient to move beyond
managing demand for mandatory assistance. Recent increases in budgets through
the Better Care Fund has facilitated local service providers, including Oxford, to
develop forms of Added Value assistance for older and disabled people that support
independence in the home.
Promoting local services: The campaign in Oxford to encourage increased
referrals to the expanded range of services included the following:
Appointment of a caseworker to coordinate the awareness raising programme
Meetings with key Social Care staff including triage staff in the Independent
Living Centre
Awareness raising with blue light services - especially Fire Services
Contact with key personnel responsible for hospital discharge and Better Care
Fund plus GP consortium groups
Use of media including local newspapers
A series of meetings and presentations with a wide range of relevant community
groups and their representative organisations
A portable stand including a banner for promotion events in significant public
spaces such as shopping centres. The banner is in a prominent place in the main
council office when not used elsewhere
Presence of an OT at meetings who can directly respond to queries, demonstrate
simple items of equipment and initiate referrals immediately.
Key Learning:
The awareness raising campaign had a very limited budget, but different
approaches have been used to maximise impact through low or no cost methods
Older people reported wanting good quality, easily understandable information in
hard copy form so a range of colourful leaflets have been designed and produced
that reflect the services potential customers indicated were important to them
Having a caseworker leading on delivering the programme of events was of
critical importance in being effective as is a visual logo for the home improvement
agency
102
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Being viewed as a rapid reliable problem solver for other services especially in
the health and care sectors was a key to success (for example in falls prevention
and hospital discharge)
Operating on a basis of accepting self-referrals as well as referrals form a range
of partner organisations and services has successfully increased the number of
enquiries for assistance
Local political support can be very useful
Maintaining a long-term commitment to engage with local people and
organisations to identify and respond to existing and emerging priorities in the
area
Results: Average DFG referrals rose from 38 in Q1 & Q2 last year, to 51 in Q3, 64
in Q4 and the increase is continuing.
Disseminating Practice: The Oxford City Council experience of advertising and
reviewing/broadening a range of assistance services has been shared with other
councils in Oxfordshire via its Benchmarking Group. There appears to be an appetite
from other local authorities in Oxfordshire to consider how such an approach could
be adopted in their respective areas. Oxford’s home improvement agency is also
keen to share their experience more widely.
Peterborough City Council - Forecasting the need for accessible
housing
Background: In 2015 the local authority was keen to demonstrate what their
interventions achieved for the local community. This would be used to inform a
strategic plan for future service arrangements and resource planning. A key element
to meet that challenge was to commission the Building Research Establishment (BRE)
to provide an estimate of the amount of accessible housing required in the city, what
proportion of homes could be made accessible through DFGs, how much through
other funding sources, and how much new build housing would be required.
The Model: The work undertaken by BRE was based on a national model produced
for the Ministry of Housing, Communities and Local Government which was then
adapted to provide a local model specific to Peterborough, in part using local datasets
including population projections. The forecast period was 2015-2030.
The model forecasts both the housing stock at different levels of accessibility, and the
expected number of householders broken down by their level of accessibility need:
namely wheelchair users, ambulant disabled and ambulant disabled (no aids).
The modelling also took account of stock characteristics (including Wheelchair Homes
and Lifetime Homes, plus those meeting or not meeting Approved Document M) as
well as funding sources including DFG and Social Care.
103
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Headline findings:
The model estimates that, based on 1,268 dwellings being built per annum and
1,480 being adapted, 33.8% of the total need of the population will be met in the
baseline year (2015).
Provision is poor for wheelchair homes and lifetime homes with only 4.5% and
16.5% of expected provision being met by the stock respectively.
A properly administered new build programme makes a major contribution to
meeting assessed need over the forecast period.
Increasing the rate of DFG provision would have to be substantial (multiplier
highest for wheelchair needs) to have an impact on the extent to which provision
has parity with/is equal to need.
Using the Findings: Whilst the conclusions were not necessarily a total surprise it
was useful to have independently derived data that enabled a more prominent position
for the DFG service in strategic planning and partnership working. The team used this
understanding of the future demand for adaptations to inform the Council’s Capital
Programme Board and Capital Strategy to ensure that the maximum DFG funding was
secured to meet the needs of the city’s residents. This ensures that those residents
can remain living in their homes safely and independently for longer, giving them a
better quality of life and therefore impacting favourably on demand management for
other higher cost services provided by the Council.
11.6 Better information about local needs will help services understand what staffing
resources are required, where they should be located and what capital
resources will be needed. Detailed mapping of current services and analysis of
county-wide need was one of the drivers of the Lightbulb project and helped
secure buy-in for reorganisation. This type of information-gathering and
analysis should be a key responsibility of the new strategic Housing and Health
Boards.
Information, advice and routing people down the right pathways
11.7 The 2014 Care Act places a clear duty on local authorities to provide advice
and information and to be able to signpost people to appropriate services.
Learning from DFG service reorganisation shows that there should be a single
access point. That access point needs to be adequately staffed to provide
advice and information and to route people effectively towards the right
pathways. The front-line service dealing with adaptation calls is a very skilled
role and one that should not be underestimated or under-resourced.
11.8 In Scotland, as part of a broader focus on outcomes, the concept of ‘good
conversations’ was introduced at the start of the adaptation process. This
incorporated supported self-assessment, raising awareness of housing options,
effective signposting and routing to appropriate services.
104

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.9 A number of different pathways are required relating to people’s needs and the
complexity and urgency of their case. This allows people to have more choice.
For example, if someone is asked at the point of first enquiry if they would
consider moving, it opens another possible route for help and support. If instead
they are automatically put in the queue for a DFG, by the time they are assessed
it may be too late to consider the rehousing option.
11.10 Online advice is another option to give people more choice. The main expert
system is ADL Smartcare which is Care Act compliant. This has been used for
several years in East Lanarkshire and is now in use in an increasing number of
authorities across England. It gives round the clock access to information and
a self-assessment system without having to wait for a therapist. People can
identify equipment, adaptations, technology or exercises that will be able to
assist them with activities of daily living. It gives people more control, and at the
same time can reduce demand for scare occupational therapy support. If used,
this needs to be easy to find and very visible on local authority websites.
11.11 A third of older people are not online, so this should not be the sole way for
people to get help. For someone who is lonely and struggling, has mental health
problems or learning disabilities there is nothing that can replace human contact
for assessment, advice and support. However, there is likely to be more staff
time to provide support to those who need it most if other customers can do
some of the assessment process themselves. A test of the flexibility of new
services will be for staff to trust and accept people’ own assessments rather
reassessing everyone.
Effective working
Deciding what is complex and needs occupational therapy input
11.12 To effectively route people down different pathways there is a need to
understand the potential complexity of the case. Without this understanding,
there is a risk that people will be routed along the wrong pathway, causing
unnecessary delay and distress.
11.13 A complexity framework for home modification services has been developed in
Australia to address the skills required to handle a case
90
. This framework,
illustrated in Figure 11.1, considers two aspects of complexity:
Firstly, whether the adaptation is likely to be minor or major. Unlike England,
where cost tends to define whether an adaptation is minor or major, in this
framework adaptations are defined by the structural changes required to
adapt the home environment.
90
Ainsworth, E., & de Jonge, D. (2019) Minor modifications: It’s not as simple as “Do It Yourself”
(DIY). To be published in E. Ainsworth & D. de Jonge (Eds.) An occupational therapist’s guide to
home modification practice (pp. 381-388). Thorofare, NJ: SLACK Inc.
105
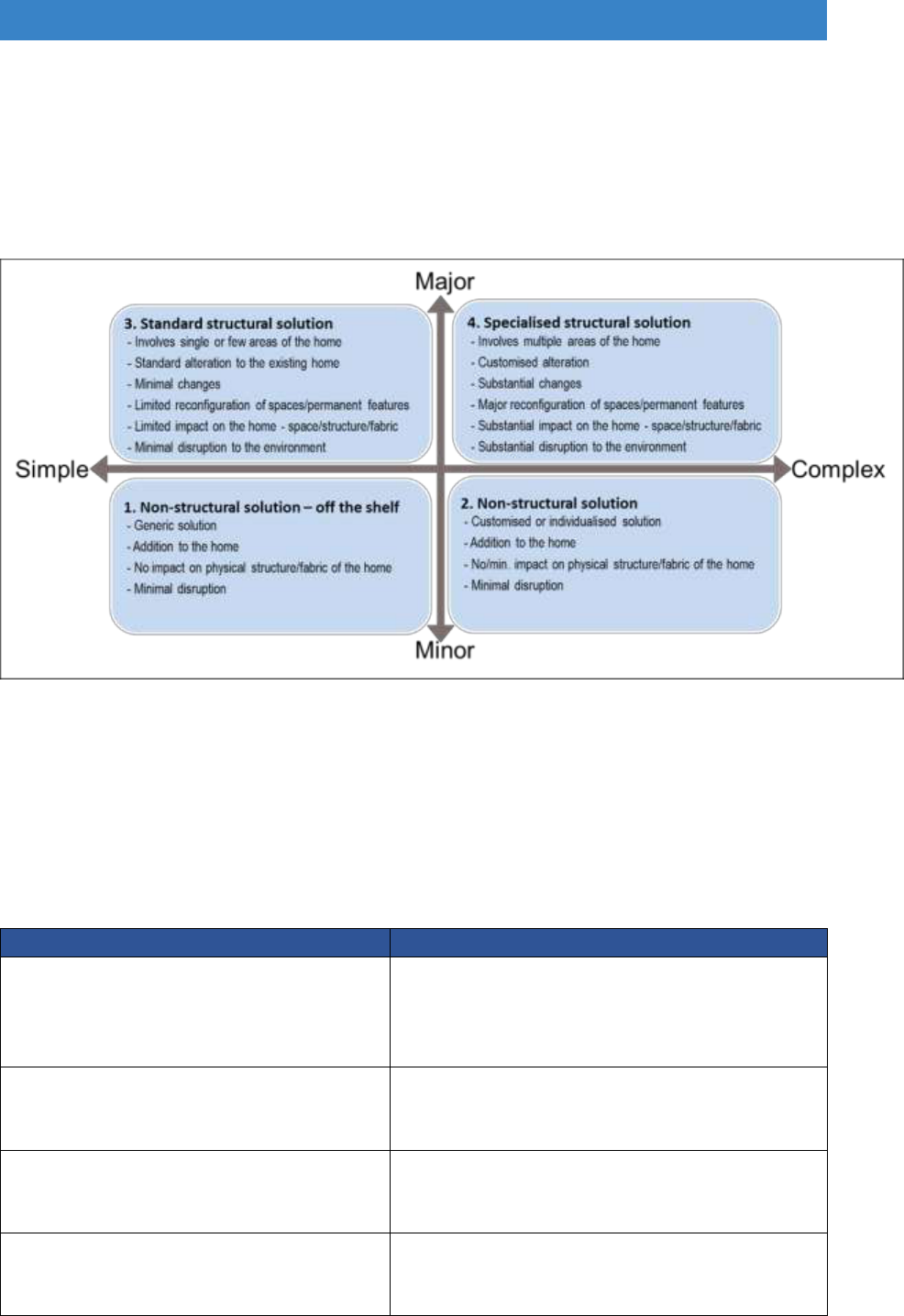
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Secondly, whether the person’s situation is simple or complex – using 54
different factors. These include the nature of the person’s condition, how
urgent the need is, the type of activity the person is wanting to do, and how
ready the person is to have their home adapted.
Figure 11.1 Framework for home adaptations service delivery
11.14 Table 11.1 provides an example of how the complexity framework can be used
to consider how different types of cases can be managed based on who has
the most appropriate skills to support the person through the adaptations
process.
Table 11.1 An integrated approach to managing cases based on complexity
The nature of the case
How the case can be managed
The situation is non-complex, and the
adaptation is non-complex
With appropriate advice and support (from
example for a handyperson or trusted
assessor) the case could be managed by
the person, carer, or family member.
The person’s situation is non-complex
but due to the structural of the
property it is complex to adapt
Housing professional leads the case but
consults with occupational therapist if
needs change or arise
The person’s situation is complex, but
the home is not complex to adapt
Occupational therapy team leads the case
but consults with housing team if advice is
required on the design of the adaptation
The situation is complex, and the
structural changes required to provide
a solution is also complex
Joint management of the case.
106

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.15 The ‘Adaptation Design Communications Tool Kit’
91
, developed in Northern
Ireland, is an example of how cross sector collaboration can improve the
delivery of adaptation services. Development involved disabled people,
occupational therapists, and housing designers/teams. Research was
conducted to produce evidence-based design standards for a range of
adaptations. Occupational therapists now use these standard designs to
recommend adaptations without additional input from the housing team. By
standardising the design of adaptations in this way, housing team members and
occupational therapists now use their time more effectively to collaborate on
complex cases where the standardised solution will not meet the person’s
needs, or where the standard adaptation will not structurally fit within the
existing layout of the home environment.
Improving the model for assessing what adaptations are necessary,
appropriate, reasonable and practicable
11.16 As part of the DFG approval process, the local authority must identify what
‘relevant works are necessary and appropriate to meet the needs of the
disabled occupant, and that it is reasonable and practicable to carry out the
relevant works’. In determining what adaptations are necessary and
appropriate, the housing authority has a duty under the legislation to consult
with the social services authority (unless they are themselves a social services
authority).
11.17 Whilst the legislation does not stipulate who in the social services authority
should carry out the function of identifying what works are necessary and
appropriate, occupational therapists have traditionally carried this out. They are
skilled at assessing older and disabled people in their home and identifying
ways the home environment can be adapted to improve health and well-being,
including the recommendation of equipment and adaptations.
11.18 Previous guidance on the DFG has acknowledged the complexity of
determining the needs of older and disabled people and for this reason has
provided little direction on what factors occupational therapists (or other
professionals involved in the assessment process) should consider when
determining what works are necessary and appropriate. The guidance does,
however, recognise that adaptation should provide sustainable and effective,
individualised solution based on the judgment of the professionals involved with
the case.
11.19 From the findings of complaints investigated by the ombudsman service, it is
evident that at times sustainable and effective individualised adaptations have
91
Northern Ireland Housing Executive (2018).Adaptations Design Communications Toolkit [online]
https://www.nihe.gov.uk/adaptations_design_communications_toolkit.pdf.
107
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
not been installed. The issue in these cases is the initial assessment of need
and the narrow focus taken by professionals in understanding what is important
to disabled and older people. It has been identified that money is wasted, and
potential harm caused when the initial assessment of need focuses on a narrow
range of factors such as safety and function, rather than wider aspects valued
as important to the person, such as dignity, choice and control.
11.20 Whilst it is important for an independent assessment to be made about what
works are necessary and appropriate, the lack of guidance on what factors
should be considered has hampered professional reasoning and failed to give
older and disabled people a voice around what they value. This failure has led
to adaptations not providing individualised and sustainable solutions. To reduce
the risk of installing inappropriate adaptations and to ensure consistency of
practice across England, it is evident that written principles could assist
professionals involved in the complex process of identifying what works are
necessary and appropriate.
11.21 Nine such guiding principles have already been identified by Heywood (2004)
in her research on improving the quality of adaptations provided through the
DFG system. In this research, she identified the following nine needs older and
disabled people consider important when being assessed for what works are
necessary and appropriate.
Nine guiding principles for installing adaptations
1. Need to retain (or restore) dignity
2. The need to have values recognised
3. Need for relief from pain, discomfort and danger
4. Need to minimise barriers to independence
5. Need for some element of choice
6. The need for good communication as part of giving choice
7. Need for light
8. Particular needs of children: to provide for growth and change; and the need
for space
9. Need of other family members and of the family as a whole
11.22 The above principles do not replace the professional judgement of practitioners;
instead, it provides a framework to support the decision-making process and to
support the communication of what works are necessary and appropriate for
improving the health and well-being of older and disabled people.
108
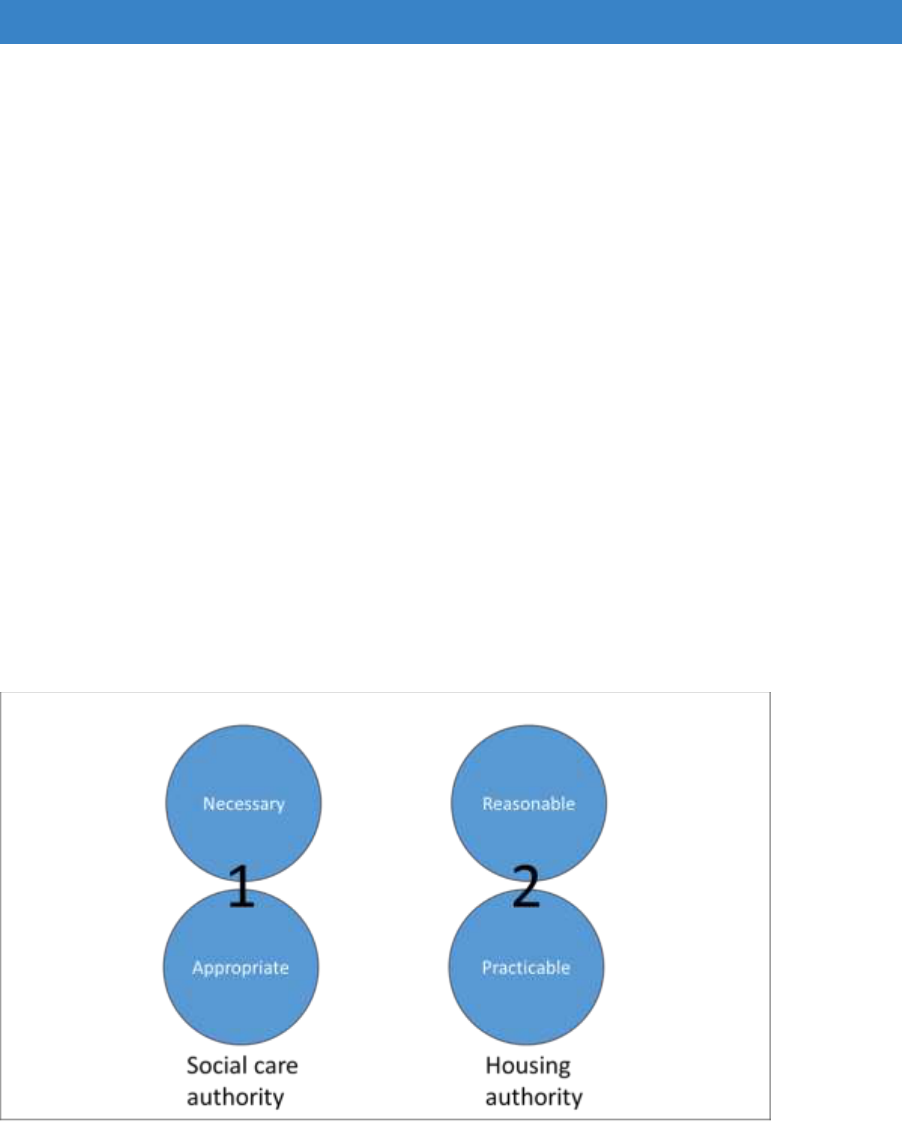
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
A collaborative model for the process of determining necessary and
appropriate, reasonable and practicable
11.23 In the legislation, and supporting case law, the function of identifying what works
are necessary and appropriate must occur before the housing authority decides
upon whether the works are reasonable and practicable. The reason the
assessment of necessary and appropriate occurs separately and before the
assessment of reasonable and practicable is so that the assessment of the
older or disabled person’s needs for adaptations is based on need and not on
the resources available to fund the works.
11.24 For simple cases, this process (Figure 11.2) is fit for purpose, with the
occupational therapist completing an assessment of need with the older or
disabled person and identifying and recommending what works are necessary
and appropriate. The housing authority then decides whether the
recommended works are reasonable and practicable to award the grant.
However, where the home environment is structurally more complex to adapt,
this model can cause delay and confusion.
Figure 11.2 The traditional way of recommending adaptations
11.25 Whilst most occupational therapists working in social care and housing have a
good understanding of what can be done structurally to adapt a person’s home,
they are not building experts. Inadvertently, they may recommend an
adaptation that is not practicable to install due to the structural limitations of the
property. In these situations, after identifying it is necessary to adapt the home,
the occupational therapist may require the support of the technical officer to
identify what adaptations are practicable. Only then can the occupational
therapist decide (in collaboration with the older or disabled person), which
solution is appropriate. Resolving issues where an occupational therapist has
109
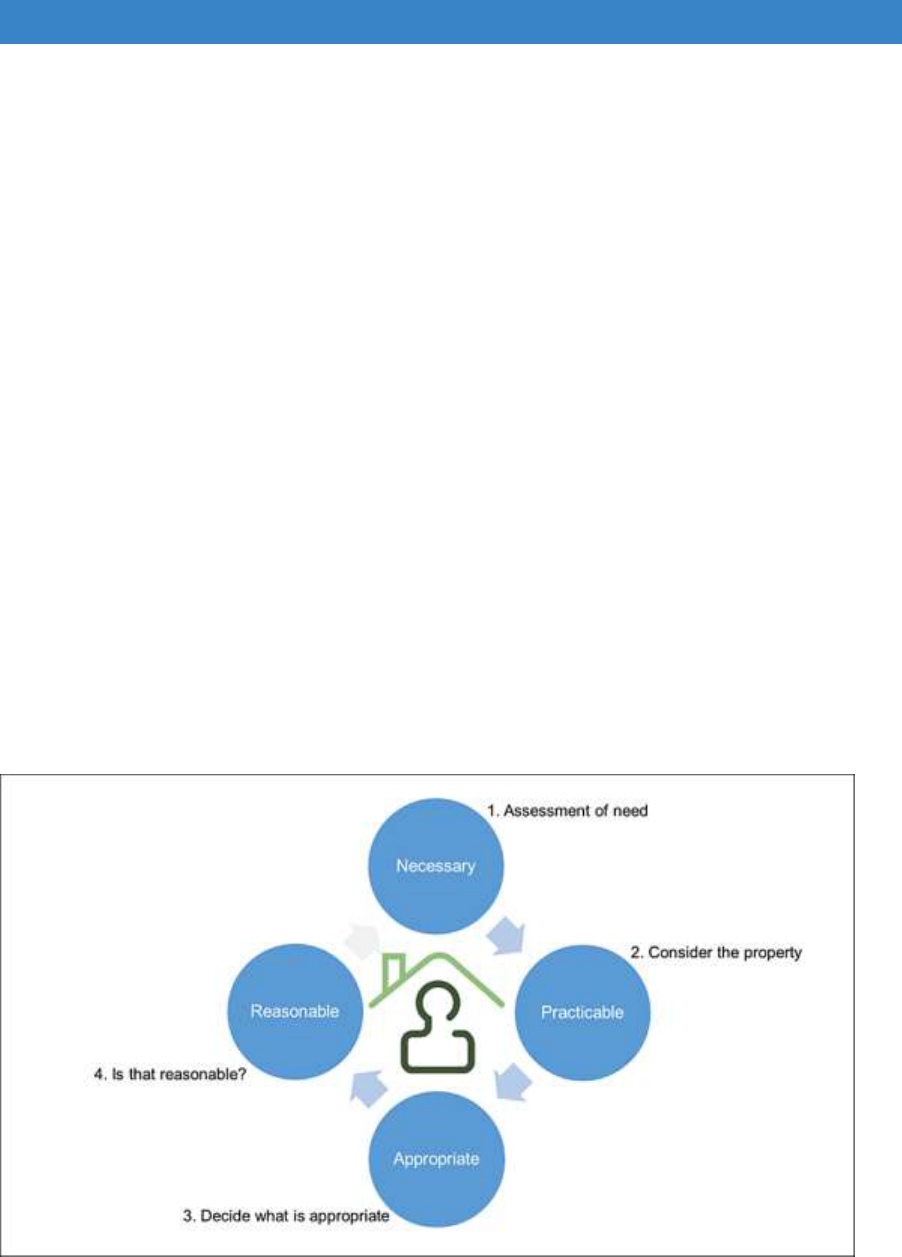
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
inadvertently recommended an inappropriate solution causes unnecessary
delay and confusion, and frustration for the older or disabled person.
11.26 To avoid the consequences associated with recommending inappropriate
adaptation, an integrated approach between the occupational therapist and
technical officer is recommended. This approach is illustrated in Figure 11.3
and demonstrates that the older or disabled person is at the centre of the
process:
The process begins with the assessment of need and with identifying if it is
necessary to adapt the home environment.
The next step involves considering the home environment and identifying
the potential solutions for adapting the home environment and meeting the
needs of the person.
From the range of solutions, the occupational therapist collaborates with the
person to identify the most appropriate solution.
The final stage of the process considers whether it is reasonable to approve
the grant.
11.27 Currently, a number of occupational therapy and housing teams routinely
conduct these types of joint home visits.
Figure 11.3 A way of developing better adaptation solutions
11.28 These new ways of working underpin the ‘goldilocks’ approach of partnership
working and are encouraged by the Royal Collect of Occupational Therapy who
said that occupational therapists must realise that “your work or role may be
integrated into a larger cross-agency service. You may need to adapt your
110

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
working, learn new skills and share those you have. Working closely with your
colleagues can enable a more comprehensive and efficient service”
92
.
Developing a standardised design and construction process for housing
adaptations
11.29 As with the DFG process, several professional groups are involved in the design
and construction of large building projects. For these projects to be completed
on time and within financial constraints, the flow of information between these
professional groups is crucial. It is also important that each group is aware of
how they, and others, contribute to the overall success of the project.
11.30 Within the design and construction industry, a number of standardised
processes have been developed, such as the RIBA Plan of Work
93
, to manage
this process. By simplifying the process, making transparent the responsibility
of each professional group, and identifying where and how information needs
to flow through the process, these standardised tools have improved the way
major building projects are delivered.
11.31 Home adaptations are relatively simple design and construction projects,
however the report from the DFG summit in 2015 (organised by the Royal
College of Occupational Therapists and Foundations) identified and
recommended making it easier for older and disabled people and their carers
to understand the process and to improve the flow of information between
professionals and teams involved in the delivery of the DFG
94
.
11.32 Given the benefits of using a standardised process on large building project, a
standardised process for the design and construction of adaptations would
address several recommendations from the DFG Summit. The Welsh Audit
Office review of the DFG 2018 found that occupational therapists and other
professionals ‘believe that their work would benefit from standardising
assessment approaches and forms across delivery organisations”
95
.
11.33 Recent research on the role of occupational therapists in the adaptations
process has led to the development of a standardised process called the Home
Modification Process Protocol (HMPP)
96
. The HMPP is based on a design and
construction process and describes the role of the occupational therapist at
92
Royal College of Occupational Therapists (2016) Care Act 2014 Guidance for Occupational
Therapists: Disabled Facilities Grants 2016, p. 19. [online] https://www.rcot.co.uk/practice-
resources/rcot-publications/downloads/care-act-2014-dfg.
93
RIBA (2013) Plan of Work [online] https://www.ribaplanofwork.com/.
94
Royal College of Occupational Therapists and Foundations (2015). DFG Summit. [online] London:
Royal College of Occupational Therapists and Foundations.
https://www.rcot.co.uk/file/1550/download?token=UJrn-qHx.
95
Wales Audit Office p.40, ibid.
96
Russell, R., Ormerod, M. and Newton, R., (2018) The development of a design and construction
process protocol to support the home modification process delivered by occupational therapists.
Journal of aging research. https://doi.org/10.1155/2018/4904379.
111

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
each phase of the project. The process also identifies when occupational
therapists need to collaborate with housing colleagues and indicates what
information housing colleagues require from the occupational therapist to
enable the efficient and timely installation of the adaptations. As the HMPP is
based on occupational therapy principles, it takes a person-centred approach
and demonstrates how older and disabled person and their carers can be
involved in all phases of the process.
11.34 The outcome of using the HMPP in a proof of concept with a team of
occupational therapists working in a local authority housing team indicates that
it provided therapists with a greater understanding of how their role fits in with
the overall design and installation of an adaptation. The occupational therapists
indicated the tool had helped them and housing colleagues to develop a deeper
appreciation of each other’s role, and that they had made changes to the DFG
process so that they made better use of time and each other’s skills. The HMPP
gave the occupational therapists a better appreciation of what type of
information housing colleagues needed about the person to help in the design
the adaptation, and this then helped the therapists to consider ways in which
they could share information in a way that did not breach confidentiality or
compromise professional standards.
Communicating with customers, carers and their families
11.35 There is emerging evidence that better visual tools are needed to communicate
design plans to customers, carers and their families and to contractors
97
. Most
people coming into DFG services know very little about equipment and
adaptations, and do not know what is available or how it will fit into their home.
11.36 A research study looked at the role of 3D design in the communication
process
98
. A 3D tool helped people better communicate to professionals the
nuances of the way they use their home, and it helped practitioners show the
home adaptations options available. Users were able to see what these looked
like and discuss how those changes might impact on their personal
environment. It was a small study with people who were reasonably computer-
literate, but it clearly allowed much better communication and joint decision-
making and avoided a lot of the mis-understandings that currently occur. A key
finding was that people appreciated using these tools alongside the
professional rather than on their own.
97
Walker, M. (2016) Effective communication methods for Housing OTs http://ot-
magazine.co.uk/effective-communication-methods-for-housing-ots.
98
Money, A. et al. (2015) Using the Technology Acceptance Model to explore community dwelling
older adults’ perceptions of a 3D interior design application to facilitate pre-discharge home
adaptations, BMC Medical Informantics and Decision Making, 15:73. https://doi.org/10.1186/s12911-
015-0190-2.
112

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.37 People are getting used to kitchen and bathroom vendors using these 3D tools
and will increasingly expect to see them used by adaptations teams. A number
of tools have been developed, such as:
The IDAPT 3D planner
99
. IDAPT is a specialist computer-aided design
system used by many local authorities to produce floor plans and 3D
visualisations for standard adaptations like showers and ramps. They are
currently developing a virtual reality module with photo-realistic renderings
of adaptations that would allow a client to be placed into an adapted space
and fully understand how it would work for them.
Glasgow Centre for Inclusive Living online 3D design tool to help people
plan their homes
100
.
Australia has developed a sophisticated online tool called My Home Space
to help disabled people plan their own designs
101
.
A number of apps are being developed to help with design and adaptation
planning for people with dementia
102
.
There is also a Home Modify App from Australia
103
.
11.38 Having a design centre or centre for independent living such as in Dorset,
Bristol, North Somerset or Knowsley is another option that allows people
greater access to practical advice and information where they can see exactly
what the options would look like within a room setting.
Working in partnership with contractors
11.39 It is possible to fast-track work directly to contractors provided they are also
treated more as partners in the process. The Rutland example below is being
piloted and shows how stages in the ‘normal’ adaptations process can be
removed for non-complex cases. This provides a fast and effective service that
is much more in keeping with what customers are looking for.
11.40 A few authorities, such as Bristol, fast-track cases to contractors who use the
IDAPT planning tool to communicate decisions to the adaptations team. They
can also use it to discuss options with customers making communication better
all round.
99
IDAPT 3D planner https://www.idaptplanner3d.com/
100
Glasgow Independent Living Centre www.home2fit.org.uk, www.adapt2fit.org.uk.
101
My Home Space https://www.myhomespace.org/
102
University of Stirling (2018) App to help improve environments for people living with dementia.
https://www.stir.ac.uk/news/2017/06/newapptohelpimproveenvironmentsforpeoplelivingwithdementia/.
103
https://www.homemods.info/apps
113
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Rutland – working in partnership with contractors
Rutland is a small, unitary authority in the East Midlands. It had a very traditional DFG
service but is trialling a new approach. The DFG budget (£211,000) was often
underspent because Rutland is a relatively affluent area and most clients fail the
means test. However, they are still vulnerable and in need of support. The DFG team
wants to promote independence and mirror health interventions which are mainly free
at the point of contact.
Health Prevention Grant (HPG) delivers rapid outcomes with no means test up to a
maximum of £10,000 (£9,000 plus contingencies). A 12-month pilot started In October
2017 across all tenures (the council stock was transferred to a registered provider).
By the end of March 2018 49 cases had been opened and 24 completed. More people
are coming forward because of the flexible, non-stigmatising approach.
The adaptation service - partnership with local contractors. Specifications are
written by the referrer (occupational therapist, occupational therapy aide or
physiotherapist) with contractors trusted to take responsibility for the project as they
would with any private client. They are asked to personalise the offer, for example,
they hold a range of non-white, non-standard size wall tiles to offer clients choice to
get away from the ‘medicalised’ grant model. If they wish, clients can use their own
contractor and upgrade the specification using their own funding. There is no grant
officer or technical officer involvement other than as a ‘facilitator’ to help support clients
and contractors. Inevitably there are extras and unforeseen work, but this has not
caused major problems.
The average time from application to completion for a level access shower is
12.6 weeks, with stairlifts taking 2.7 weeks through a single supplier contract.
stairlifts and ceiling track hoists get a two-year warranty and are replaced if they fail.
They have also pre-purchased modular ramps from a company who store them, install,
service and remove.
Complex DFGs over £10k are delivered by Peterborough County Council as
Rutland has very few each year.
Delivering better health and social care outcomes
Examples of preventative services providing savings to health and care
11.41 There are now a large number of adaptation services providing direct support
to health through hospital discharge schemes and falls prevention work.
Foundations and the Housing LIN have produced an interactive map that will
be regularly updated to show the types and location of different services
104
.
There are four key categories of service:
104
Housing LIN (2018) Home from Hospital tool [online] https://www.housinglin.org.uk/home-from-
hospital/tool/.
114
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Co-located / embedded caseworkers (often within hospital discharge
teams), linked to a community-based handyperson’s service to deliver
practical support in the home.
Co-located / embedded housing support, focussed on providing assessment
and holistic community navigation, based within a hospital discharge team.
Community-based practical housing support, including handyperson’s
services, focussed on preventing admissions to hospital as well as
supporting patients in transition and on their return home.
Step down beds and apartments provided within a housing setting, to enable
prompt hospital discharge before a patient is ready to return home.
West of England Care and Repair hospital discharge service
To enable older patients to return home from hospital more rapidly and safely, West
of England Care & Repair (WECR) organises and/or carries out:
Clutter clearance/deep cleaning to make home sanitary
Urgent home repairs to make home safe and secure
Sanitation repairs e.g. broken toilet, washing facility
Hazards removal e.g. falls risks, electrical wiring dangers
Heating systems repaired/emergency heating
Small, essential adaptations e.g. stair rail
Some patients pay for the work themselves but there is charitable funding for those
who either have no resources or where it would take too long to organise payment,
such as those on low incomes, with dementia or mental health problems.
Service Capacity: 135 patients discharged from hospital per FTE Caseworker per
annum. Average cost of works per discharge £273.
Impact: An independent evaluation used case records and interviews with hospital
staff to assess how the housing interventions affected length of stay in hospital and
examined time savings for hospital and care staff
105
. This identified:
A saving in hospital bed days of £13,526
A total cost of the housing interventions to achieve @ £948
A cost-benefit ratio of 14:1
Savings in hospital staff time amounted to a further £897
Falls prevention: WECR is also piloting and evaluating a falls prevention project. An
occupational therapist and a handyperson do home safety checks, fix trip and fall
hazards, fit minor adaptations and provide people with better strategies to move safely
around the home and outside.
105
Adams, S. (2016) Reducing Delayed Transfer of Care through housing interventions: Evidence of
Impact. http://careandrepair-england.org.uk/wp-content/uploads/2014/12/WE-C-R-Case-Study-
Final.pdf.
115
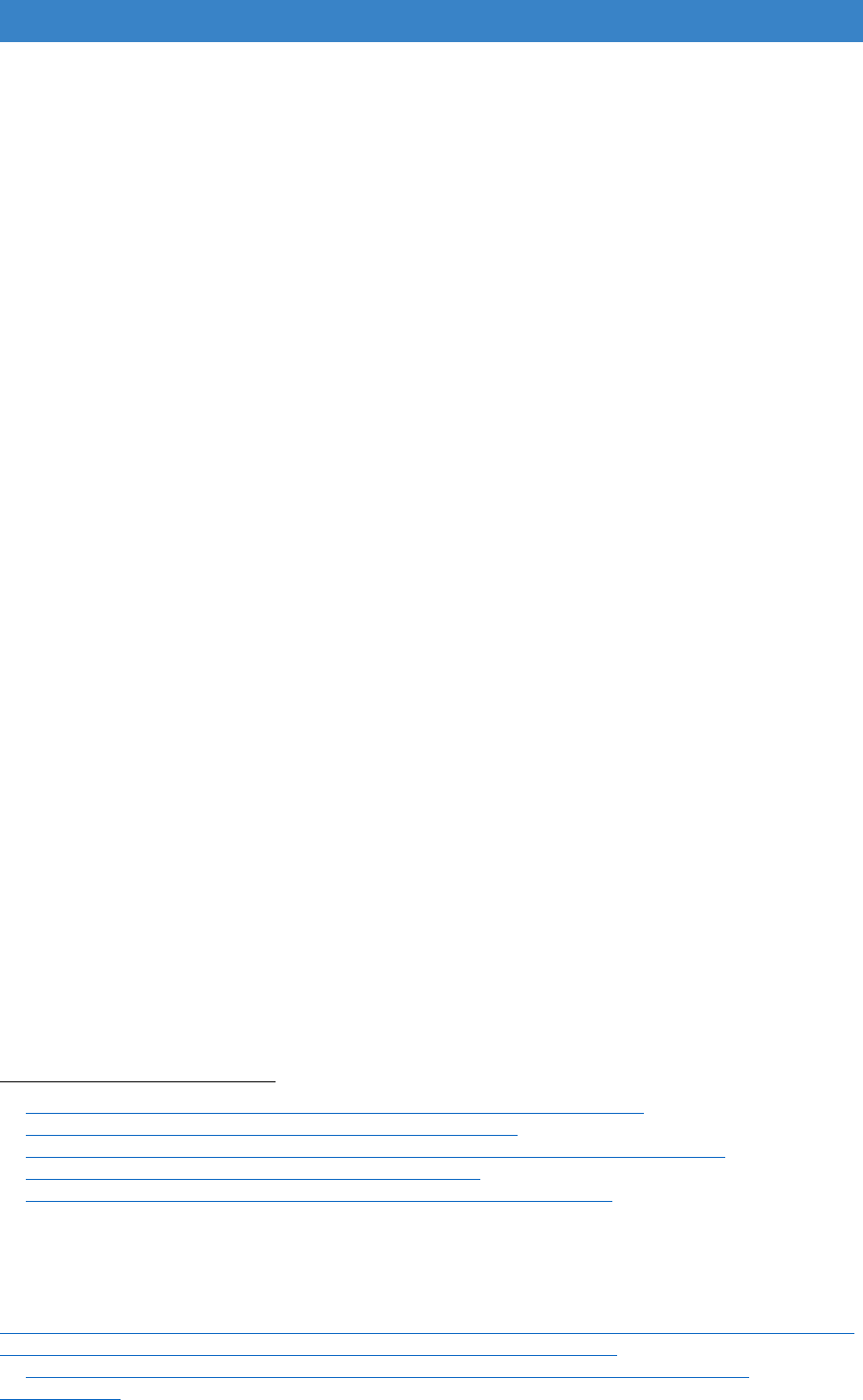
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Dementia and the DFG
11.42 The number of people with dementia in the UK is forecast to increase to over
one million by 2023, with the largest increases for people over 80
106
. Over 90%
of people living with dementia have more than one health condition
107
. They are
very high users of health services, accounting for 20% of all hospital
admissions. They occupy 25% of beds at any one time, are three times more
likely to experience a fall in hospital and 20% more likely to die. They tend to
stay in hospital 25% longer and are twice as likely to be readmitted
108
. Around
40% of people with dementia admitted in an emergency will be discharged to a
place other than home
109
and they account for over 70% of those in residential
110
care .
11.43 The home plays an important role as two-thirds of people with dementia live in
ordinary housing
111
and 85% of them express a preference to remain there
112
.
Helping people remain independent at home, and for that home to be fit for
them to be discharged after a hospital stay, is therefore vital to reduce
pressures on health and care services. Up to now there has been limited use
of the DFG to improve homes for people with dementia, but there is scope for
it to be used far more as a preventative measure.
11.44 Dementia friendly design principles were developed in health and care settings
which are not always easily or acceptably transferred to someone’s home.
There is beginning to be greater understanding of what works in the home
113 114
supported by the publication of a number of design guides and apps .
There has been some evaluation of outcomes, but this needs further research.
There also is a need for more dementia specific training for staff delivering the
DFG. The following example shows how the DFG is being used in more
innovative ways.
106
https://www.dementiastatistics.org/statistics/prevalence-by-age-in-the-uk/
107
https://www.dementiastatistics.org/statistics/comorbidities/
108
https://www.cqc.org.uk/sites/default/files/documents/cqc_care_update_issue_2.pdf
109
https://www.dementiastatistics.org/statistics/hospitals/
110
https://www.alzheimers.org.uk/about-us/news-and-media/facts-media
111
Alzheimer’s Society (2012) Home Truth. Housing Services and support for people with dementia.
London: Alzheimer’s Society.
112
Alzheimer’s Society (2016) Fix Dementia Care: Homecare, London: Alzheimer’s Society.
113
Dementia Services Development Centre (2013) Improving the design of housing to assist people
with dementia, Stirling: University of Stirling.
http://www.cih.org/resources/PDF/Scotland%20general/Improving%20the%20design%20of%20housi
ng%20to%20assist%20people%20with%20dementia%20-%20FINAL.pdf.
114
https://www.scie.org.uk/dementia/supporting-people-with-dementia/dementia-friendly-
environments/.
116
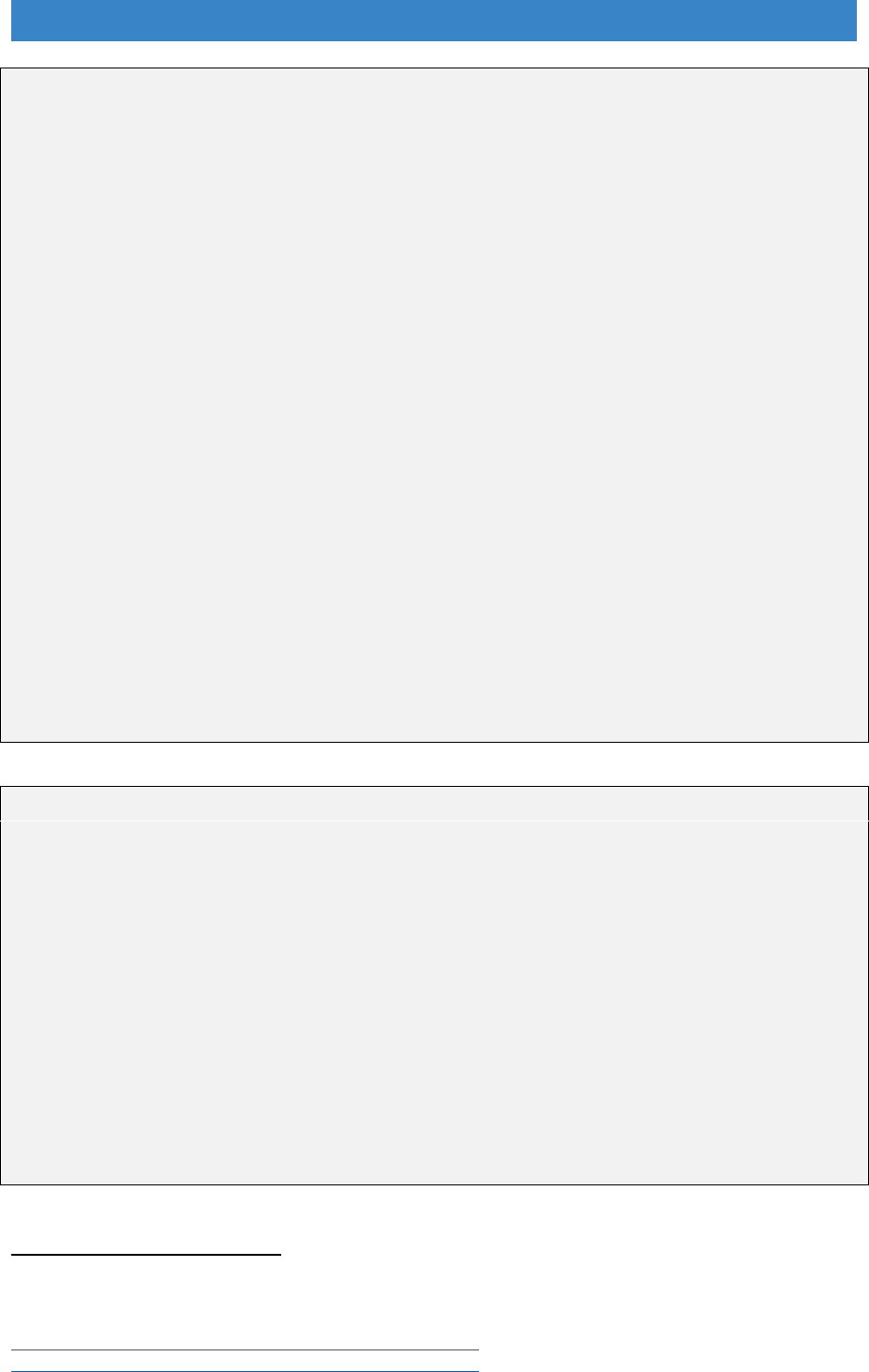
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Design for dementia
Dementia Dwelling Grants - Worcester City Council is leading a joint health, social
care and housing project that involves integrated working between six local authorities
(Bromsgrove, Malvern Hills, Redditch, Worcester, Wychavon and Wyre Forest District
Councils). It uses a top-sliced amount of the DFG allocation to provide non-means
tested grants to help people with dementia make changes to their home. People are
referred via the community mental health team, GPs and the early intervention
dementia team to Age UK Hereford and Worcestershire Dementia Advice Service
(DAS). Dementia Advisors provide advice and information and support households to
claim the grant. The maximum available is £750 per household.
The project is being evaluated by the University of Worcester
115
. In 2017-18 over 500
people were assessed and over 380 accepted the grant. Over 86% of recipients are
home-owners living in their own home rather than in residential or acute care. People
choose their own preferred solution based on the difficulties they are experiencing and
feedback about what works and what does not work on evaluation visits.
The average cost of a Dementia Dwelling Grant is only £150 for those living alone and
£132 for those living with a partner or family. This evaluation will help inform the design
of future equipment and adaptations. Other local authorities are copying the model
and writing Dementia Design Grants into their RRO policies. This project demonstrates
that a timely, preventative, housing response to a diagnosis of dementia need not be
expensive to the public purse. It can make a substantial difference to the lives of
people coming to terms with their diagnosis and help them maintain their
independence for longer.
BRE demonstrator home
The BRE innovations park at Watford showcases good practice in building design and
has around 20,000 visitors a year. In 2018 they opened a demonstrator home aimed
at professionals in the health, care and housing sectors involved in helping people live
independently in later life, particularly those with dementia.
It originated from collaboration with an architectural partnership and staff from John
Moores University in Liverpool who had used a ‘living laboratory’ approach to see what
was important to enable people with dementia to carry on living in their own home
116
.
In collaboration with BRE they developed a set of design principles. As most people
live in the existing stock and want to stay in their home BRE have created a typical
home, a Victorian terrace house, to demonstrate good practice in how to retrofit a
home for later life and how this can help people with dementia.
There is potential to use this as a training location for home adaptations teams.
115
Evans, S., (April 2018) Dementia Dwelling Grants – evaluation of the pilot programme. Interim
evaluation report, University of Worcester Association for Dementia Studies.
116
Halsall, B. and MacDonald, R. (2015) Design for dementia – Vols 1 and 2.
http://www.hlpdesign.com/images/case_studies/Vol1.pdf.
http://www.hlpdesign.com/images/case_studies/Vol2.pdf
117

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Making every contact count (MECC)
11.45 There is much more scope for health, care and housing to work better together,
particularly to identify people who require adaptations before they reach crisis
point, as a lot of need is hidden. There are several services that could potentially
identify and refer those who need help if they find that someone is living in a
home with potential hazards, has already had a fall, is beginning to struggle
with activities of daily living or is in the early stages of dementia. These include:
GP surgeries
Community health/care navigators/social prescribing teams
‘Staying steady’ exercise classes for people who have experienced falls
Dementia clinics and memory cafes
Fire service home safety checks
117
Care providers
11.46 In 2015, Age UK developed a pilot care navigator project in South
Warwickshire. They worked with people over 75 who had the greatest health
care needs from 31 GP surgeries. It was done in conjunction with the FirstStop
advice service. The service raised awareness of housing and care options;
gave specific housing and care advice; and provided more extensive help to
enable people to move home, get adaptations or otherwise improve their
housing situation. Evaluation showed that the potential cost savings of better
health outcomes considerably outweighed the revenue costs
118
. There is
potential for DFG teams to work in partnership with care navigator services
across the country.
11.47 Other health and housing links are being developed, as is demonstrated by the
Cornwall Home Solutions adaptations service. They have a pathway to ensure
that that adults and children who are referred for a wheelchair get an
assessment to see if they need adaptations to their home. They also consider
whether a riser wheelchair would be a more cost-effective solution. If this was
a standard service across the country, it could make a huge difference to
wheelchair users. The 2015/16 English Housing Survey found that there are
232,000 households with at least one person who uses a wheelchair inside the
home. Half (51%) found it very, or fairly, difficult to manoeuvre their wheelchair
around their homes, so there is obviously a high level of unmet need
119
.
117
Public Health England (2016) Evaluation of the impact of Fire and Rescue Service interventions in
reducing the risk of harm to vulnerable groups of people from winter-related illnesses.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/57
3558/FRS_winter_pressures_evaluation.pdf.
118
Adams, S. (Mar 2017) Integration in Action: Evaluation of Age UK Warwickshire’s provision of
impartial information and advice about housing, care and related finance in later life.
http://careandrepair-england.org.uk/wp-content/uploads/2017/05/AgeUk-W-Evaluation-report-
Final.pdf.
119
Ministry of Housing, Communities and Local Government (2018) English Housing Survey 2015/16,
ibid.
118

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.48 There are also a number of well-established hospital discharge schemes being
run by home improvement agencies, such as Manchester Care & Repair, but
not many have been properly evaluated and written up. There is a need for
more research to demonstrate the impact of improving housing on health so
that more partnership working can be established.
Data collection and reporting
11.49 Home adaptation services have been good at reporting outputs (number of
grants and amount spent) but not as good at measuring outcomes and impact
(number of people helped to remain independent and impact on health and
wellbeing) as this is much more difficult. It is beginning to change. There is a
need for much better evidence to support service reorganisation, and once
services are integrated and strategic oversight is stronger, regular performance
reporting is expected. There is also a need to collect and evaluate a range of
data to demonstrate fair access to services under the Equality Act.
11.50 One important element of service delivery is the end-to-end speed of the
service. The 2013 good practice guide gave a table of time targets for three
stages of the customer journey: 1) from first enquiry to occupational therapy
referral; 2) from referral to approval; and 3) from approval to completion of work.
This was further split into urgent and non-urgent work. However, there is often
no effective end-to-end reporting system. There is also no contingency fund to
deal with backlogs if delays occur.
11.51 Time measurement should reflect the new context that the DFG is operating in.
Services have to be faster if they are to be preventative and work effectively
with health and social care. Customers need a much quicker service to return
from hospital, to prevent their condition worsening, to improve their wellbeing
and to stop carers being put under undue strain. This requires fast-track
systems which may cut out some stages entirely or new funding packages of
which the DFG is only one part.
11.52 What is needed is much better data collection, effective reporting and
benchmarking with other authorities, with services accountable to their Housing
and Health Partnership Board, the BCF and HWB (or their successor bodies).
Local reporting
11.53 Use of NHS numbers on case files is still not commonplace, despite being a
requirement of the 2014 Care Act and the BCF. There is a need for more data
sharing protocols and alignment of IT systems to enable the end to end
customer journey to be more effectively managed and monitored than it has up
to now.
119
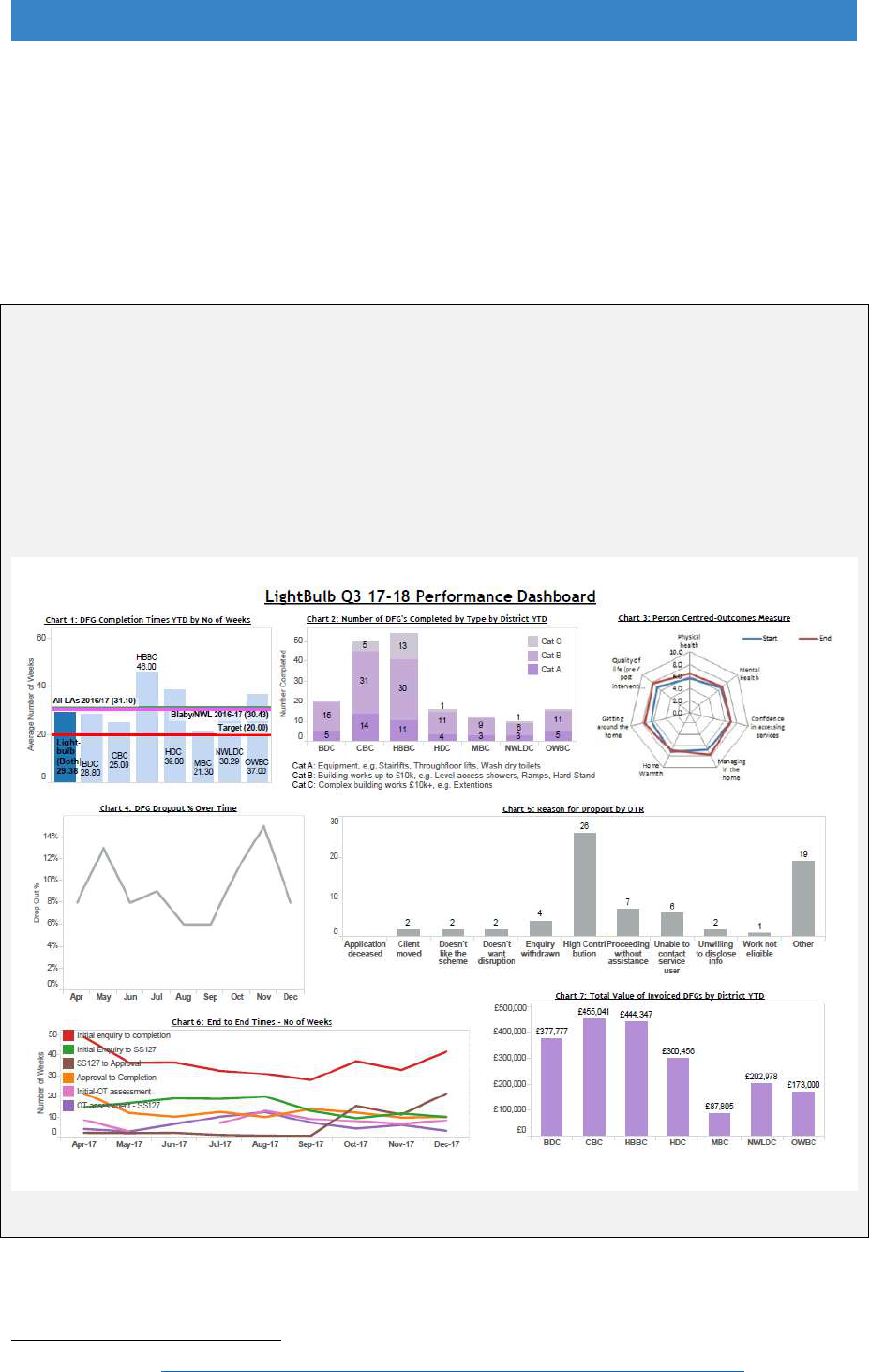
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.54 Some useful reporting models are developing, as evidenced by the Lightbulb
dashboard below. Foundations has also launched a DFG analytics system in
partnership with Intel4Housing
120
. This incorporates cost, timescales, outcomes
and social value data and allows services to benchmark their performance
against others to see how they compare, learn from their approach and
measure improvement over time.
Leicestershire Lightbulb project performance dashboard
A performance management system was designed for the Lightbulb Programme when
it was established. It provides Management Board and Delivery Group members with
a dashboard of tables and charts giving an overview of key areas of performance. A
report is produced each quarter and compared to previous figures. A separate
dashboard shows results of the Hospital Housing Enabler work. The data is used to
improve performance and deliver a more effective service for customers.
120
DFG Analytics http://www.foundations.uk.com/dfg-adaptations/dfg-tools/dfg-analytics/
120

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Intel4Housing – DFG Analytics
i4H is a specialist consultancy who set-up analytics and benchmarking systems to
drive performance improvements in social housing. They recognised the potential to
use advanced data analytics techniques with the DFG that would provide valuable
business intelligence.
Working with Foundations they have established a large database of DFG
performance data that Local Authorities can use to benchmark their own performance
and identify key areas for improvement. A number of Councils have now signed up to
the system and collaborating through a learning and innovation club.
11.55 It is very important to demonstrate the impact of adaptations to health and social
care partners and to provide effective case studies. Case studies are a crucial
way of showing how the grant works, its impact on disabled and older people,
and potential cost savings. One way of doing this is shown below.
Tower Hamlets Improvement Project
Aim: to capture the impact of the provision of wet floor showers on care packages and
the benefits to the person/carers.
Occupational therapists seldom review care needs when adaptation work has been
completed, this is left to reablement or social work teams. These teams have waiting
lists which delays reviews and there is no feedback to allow assessment of the benefits
of adaptations. With support from managers and project specialists, four occupational
therapists developed the skills and knowledge to review care packages. It created a
more streamlined review process with reduced waiting times and better continuity of
care for service users. Four cases were selected on the basis that the care package
was only for personal care or that it was a large component of the care package.
Results: In three cases the care package was stopped, and in the other considerably
reduced after the adaptations were installed. All participants felt more independent
and their dignity and wellbeing had improved. They were also more physically active
as they were carrying out their own personal care.
The total care cost saving over a 12-month period: £23,930.
The review procedure has now been rolled out to the whole team and managers are
recording the on-going cost savings.
Learning points: cases need to be open for longer than normal and there must be a
way of handing cases over to the social work team if care is complex.
121

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
11.56 It is important to recognise that the shift to measuring outcomes is about “a
different way of seeing and providing public services that starts with people’s
lives and what matters to them in their lives”
121
. It is about getting the right
information to understand what is happening to the service and what it is
delivering, but the real focus should be on how many more people it is reaching
and helping to achieve their own housing goals. The outcomes star shown in
the top right of the Lightbulb dashboard might be a good way to help staff really
listen to customers to find out about their needs, and after work has been
completed to see how the service has helped individuals reach their goals.
11.57 It is not just about data collection. Having a user scrutiny panel and following
up with any customers who were not fully happy with the service will also help
to feed into continual service improvement.
National reporting
11.58 Up to now, national level data has only been available from LOGASnet, which
is an administrative dataset, not one designed for detailed analysis and
research. Returns are voluntary and have reduced over the last five years to
only 66% completion rate in 2016/17. As part of the review a Better Care Fund
lead told us:
“My surprise came in that the data is retrospective and provided
voluntarily, so although the majority of Local Authorities provide the
information, some don’t. How can so much money exchange hands and
there be no regulated return? Commissioned services be they Local
Authority, Clinical Commissioning Group or anything over £15k have to
report on activity monthly. This leaves the fund open to a whole raft of
inadequate use, and lack of innovative application. Were it monthly or
quarterly as part of one BCF report, partners and the Health & Wellbeing
Board would be able to scrutinise it justifiably along with the rest of the
programme using an integrated lens."
11.59 This Review has used LOGASnet data but has had to rely on Freedom of
Information Requests to fill gaps in the evidence base. This highlights the need
to introduce far more robust monitoring arrangements that help us better
understand the impact of DFG, and also to allow Local Authorities to benchmark
their delivery and drive service improvements.
11.60 LOGASnet is due to be replaced. There is scope to add more detail and to make
the return a condition of DFG funding so that effect of changes to service
delivery can be monitored more effectively.
11.61 To support local scrutiny and innovation we recommend that the current annual
LOGASnet returns are replaced with quarterly submissions. The aim should be
121
Jeffs, M. (2018) Moving from outputs to outcomes [online]
https://goodpracticeexchange.wales/2018/05/15/moving-from-outputs-to-outcomes/.
122

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
to understand the pattern of local delivery and follow progress in delivering the
recommendations set out in this report. We recommend a broader set of
indicators is used to cover the different elements of integrated adaptation
services, including the DFG. The return should be prepared by each Housing
and Health partnership board as a required part of future BCF plans (or similar
future requirements) and come under the overall metric of ‘the number of people
helped to remain independent at home’. A short list of possible variables to be
included is shown in Appendix A1.
Recommendations – working better together
Better analysis of local need to develop preventative strategies and
determine levels of revenue and capital funding.
Better partnerships with health and care to ensure that ‘Making Every
Contact Count’ works effectively to refer people earlier, not at crisis point.
A single point of access with ‘good conversations’ at the start so that people
are routed down appropriate pathways.
New staff roles combining occupational therapy, technical and casework
skills to support customers more effectively.
New decision-making tools to help occupational therapy and technical staff
collaborate more effectively.
Use of 3D design and design centres to communicate better with customers
and tailor solutions to people’s own goals.
Use of NHS number on all files, data sharing protocols, aligned IT systems
and improved local reporting focussed more on outcomes.
National reporting by each Housing and Health Partnership Board as a
requirement of future BCF plans
123

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 12. The allocation of resources
Current allocations methodology and the need for review
12.1 In recognition of the rising need for home adaptations, central government
funding for the DFG within the BCF has increased considerably. In 2016/17,
provision rose from £220 million to £394 million. In 2018/19, it is £468 million,
and it is projected to increase to over £500 million by 2019/20.
12.2 The key issue for DFG allocations to local authorities that needs to be
understood from the outset is that establishing a method for distributing financial
resources relative to need is inherently difficult; there is demand in all areas but
the number of people receiving DFG in each local authority is relatively small.
In addition, the test of resources for DFG means that determining the number
of people potentially eligible for the grant is very complex. Furthermore, a lack
of robust data to identify or forecast need for DFG at local level means that any
allocations model can currently only incorporate indicators of potential need for
the grant.
12.3 The last major review of the DFG allocations methodology was undertaken in
2011 by the Building Research Establishment (BRE). At that time, the DFG
allocations were determined by using a complex mix of formulae and bids
submitted by individual local authorities. The BRE review concluded that the
allocation methodology in place was very volatile, lacked transparency and
could not represent the relative potential need for adaptations in any one year.
The large fluctuations in annual allocations also made it very difficult for local
authorities to plan, prioritise and deliver the DFG.
12.4 The BRE report proposed two new allocation methodologies. The first of these
was a ‘full’ allocations model using four factors to create an index of potential
DFG need for each region and local authority. The four factors were derived
from available national statistics and were considered the most appropriate and
robust for use in a new allocations model, and were:
the number of claimants of disability related benefits
the proportion of population aged 60 or over
the proportion of people on means tested benefits
the proportion of the housing stock that is not owned by local authorities.
12.5 The ‘full’ model had a ‘weighting’ for poverty through the inclusion of means
tested benefits and was considered to be appropriate where there is some
stringent means testing for DFG, as occurs under the present system. Using a
model which reflects relative poverty could also be beneficial should
124

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
government policy wish to direct funding to the more deprived regions and local
areas.
12.6 The second model created by BRE was a ‘simplified’ model which omitted the
means tested benefits. If future DFG eligibility were to involve less stringent or
no means testing, there is arguably less need for the allocations model to reflect
relative poverty (notwithstanding the benefits of general redistribution of funding
to the more deprived areas). Regional building price factors were applied to
both models.
12.7 Applying either the full or simplified allocation model to the entire DFG budget
at the time would have caused some large swings in local funding levels, with
some authorities much better off, but some much worse off. To avoid such large
swings, a decision was taken by Government that any future uplifts in DFG
funding would use a new allocation methodology to allow for a graduated move
to the new model. The ‘simplified’ model was chosen for any future uplifts.
12.8 There have been several developments since the new simplified model was
adopted that mean a further review is required, and include:
The incorporation of DFG funding into the BCF in 2015, so that the provision
of adaptations could form part of the strategic consideration and planning of
services to improve outcomes for service users.
Changes in the types of state benefits and the increase in state Pension
Age. The indicators of proxy need for adaptations need to be reviewed and
if necessary, updated.
Possible misalignment between local authority DFG funding allocations
versus actual local authority expenditure on DFGs
122
, some local authorities
have not spent all their DFG allocations while others have reported being
able to approve more DFGs had additional resources been awarded. It is,
therefore, important that the review evaluates the extent to which the current
or any proposed new methodology can forecast potential need for DFGs at
local level.
12.9 Without further depth research it is difficult to understand exactly why the
current allocations model would not deliver an equitable distribution of
resources relative to need, but it is important to examine each element of the
formula to assess its impact on grant distribution. Contributory factors to
possible misalignment of DFG funding with DFG expenditure and/or need may
include:
Historical factors – the mix of using the new simplified model for the funding
uplifts with outcomes from the previous allocations method, which included
annual bidding for funds by local authorities.
122
Mackintosh, S. and Leather, P. (2016) ibid.
125

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
The use of the simplified model for the allocations rather than the full model
which includes an ‘ability to pay element’; this could mean that more
prosperous local areas would benefit from funding arrangements than they
would if income (ability to pay) were factored in.
The way DFG processes operate on the ground for some areas. Any delays
for local authorities receiving their DFG allocation, delays in assessing DFG
applications and delivery delays may all mean resources are not being spent
quickly, although they are needed. There will be variations in efficiencies
among authorities through different ways of working.
Not all those in need of adaptations are applying for DFGs.
Issues with tenure – there are variations within local authority areas as to
whether registered providers and ALMOs use the DFG or their own financial
resources to undertake adaptation works for their tenants. It is very hard for
an allocations formula to reflect these diverse arrangements.
The need for DFGs will exceed the money available despite the overall
increased DFG budget provided within the BCF i.e. there is demand in all
areas for adaptations but the number of people receiving DFGs in each local
authority is relatively small.
12.10 Owing to the above developments and concerns about underspending of
allocated DFG funds in some local authorities, Government wishes to evaluate
whether the allocation methodology is still fit for purpose and, if not, what
alternative options may be available. Fair and transparent allocation
mechanisms are always important for DFG allocations and arguably more so at
present, as local authority contributions to DFG are declining and the level of
central government funding is rising.
Our approach to the review of resource allocation
12.11 This section provides details of: our overall approach to the review; the
investigation of data sources; and findings on the sensitivity analysis of different
indicators or factors related to the need for DFG.
12.12 There are several factors that will be related to the need for DFG:
The number of people with a limiting disability who require modifications to
their home to remain as independent as possible
How far the above people can afford to do the work themselves without
assistance from DFG
Whether they live in a home where they can apply for DFG (i.e. they are not
local authority renters).
12.13 In an ideal world, we would have reliable local level data for each stage of the
‘DFG eligibility journey’ (from A to B in Figure 12.1 below) that would enable the
allocations formula to accurately predict DFG need. Finding reliable proxy
126
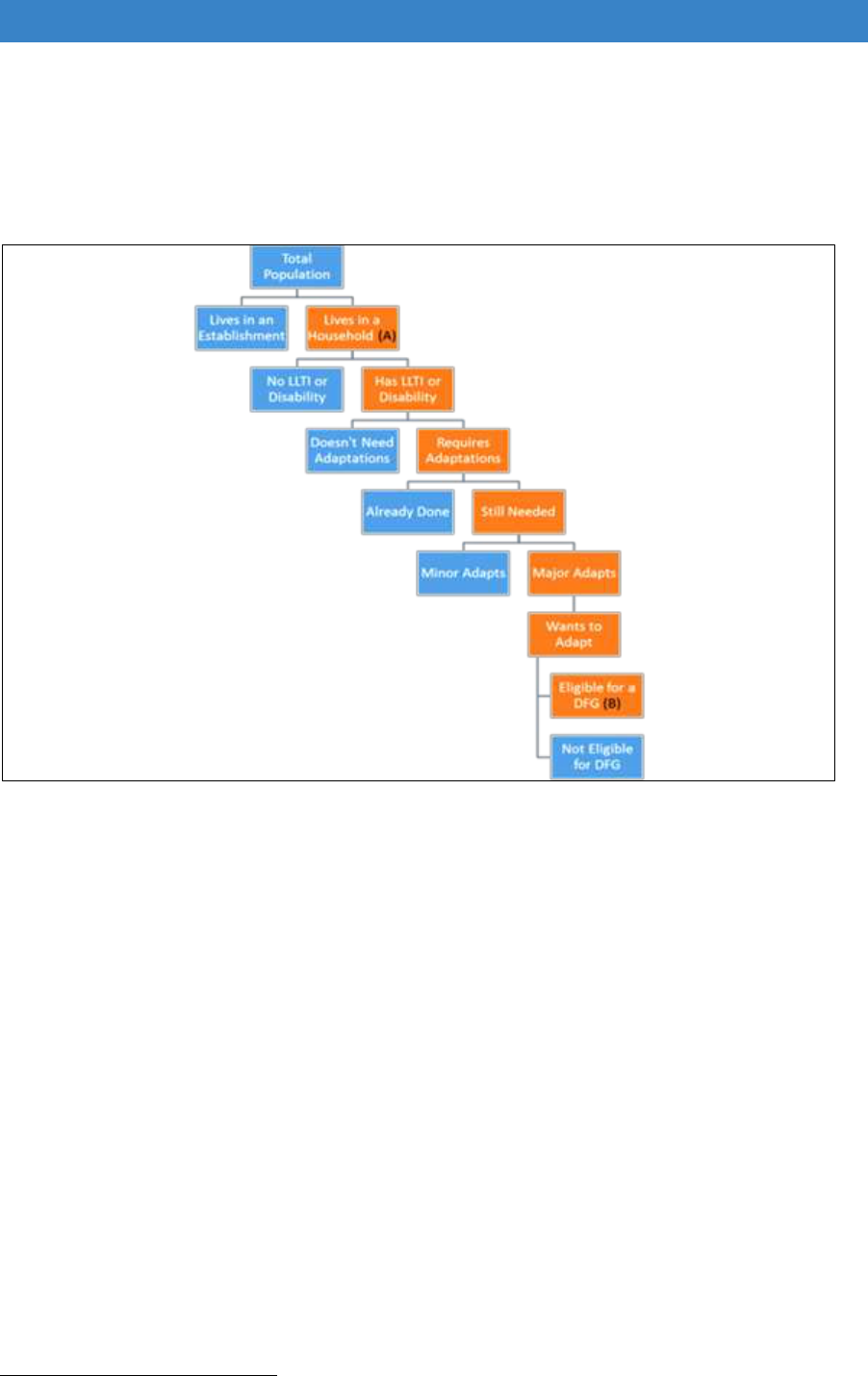
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
indicators for these is, however, not straightforward. This review of the
allocations formula has re-examined data used in the models recommended by
the 2011 BRE review and evaluated some potential new sources.
Figure 12.1 Stages of predicting DFG eligibility
12.14 As with the previous BRE review, it was considered imperative that the data
available for predicting DFG need should meet specific criteria: simplicity,
transparency, be readily accessible, be fair, and provide sustainability over the
medium-term (at least 5 years) but be responsive to changes in the population
and their circumstances.
12.15 The starting point for this review was to create a baseline of the number of
people within the local authority or region who could potentially benefit from
adaptations to their home and then add in ‘adjustment’ factors one by one so to
examine the cumulative effect of each stage; this would help determine where
the greatest shifts in the distribution of allocations may occur. In the analysis
described below, all of the adjustment factors have been given equal weight;
whether this is the preferred approach needs to be carefully considered.
12.16 Due to the timescales available for this project, we focussed on two regions
123
:
London (which is very diverse) and Yorkshire and Humberside (which has a mix
of rural and urban authorities).
123
Formerly known as the government office regions
127

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
1. The baseline
12.17 Essentially, this is our best estimate of the number of people who are most likely
to need adaptations to their home. There is no reliable, easily accessible data
at local authority level on whether people require and could benefit from
adaptations to their home, so the indicators examined can only be regarded as
proxy indicators of need. The options looked at were:
a) DWP data on receipt of benefits
12.18 The main benefits considered were: Disability Living Allowance (DLA);
Attendance Allowance (AA); Personal Independence Payment (PIP);
Employment and Support Allowance (ESA) and Carers Allowance (CA). We did
not include ‘temporary’ benefits such as Statutory Sick Pay (the latter is paid for
a maximum of 26 weeks). Other much more rarely received disability related
benefits like Industrial Injuries Disablement Benefit (IIDB) were not included, as
the number of recipients would not impact greatly on the baseline, but IIDB
could be included in the baseline if considered essential for further baseline
analysis.
12.19 The review also decided to exclude ESA from the baseline simply because ESA
is an ‘earnings replacement benefit’ where eligibility is based on capacity to
work and take part in work-related activities (e.g. training), rather than specific
disability needs. If we included both ESA and PIP, the baseline would also
double count the potential ‘need’ for many working age households giving less
weight to those who were over State Pension Age. Also, ESA is most commonly
the means tested (rather than contribution-based) variant and may be best dealt
with as part of an ‘ability to pay’ factor to be added later. Similarly, there would
be double counting if we included CA, as one of its main conditions of eligibility
is that the person cared for is already receiving one of the following: AA; the
daily living component of PIP; or at least the middle rate ‘care’ component of
DLA.
12.20 DWP claimant data is updated at least once a year and is readily accessible at
local authority level. For PIP, a number of claims are being currently reassessed
following the PIP Judicial Review that ruled that the revised guidance unfairly
discriminated against those with mental health problems. This DFG allocations
review therefore looked at the impact of using data on PIP caseload (the
number of ‘live claims’ which would include those being reassessed) and actual
recipients. Although there is a big difference in the absolute numbers, the
proportions of cases within each region and within each local authority within
the two regions examined are virtually identical. Table 12.1 below illustrates the
comparative regional profiles. The review concluded that the use of actual
recipients was best for simplicity’s sake.
12.21 One key disadvantage of using disability related DWP data is that it will
underestimate potential need, because there will be some people who may be
eligible for such benefits but who do not apply for them for various reasons. The
128
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
reasons include lack of knowledge, uncertainty around entitlement and concern
that receipt of certain benefits may impact adversely on other support received.
That said, DWP data is probably no less robust than other proxy indicators.
Table 12.1 Distributions of disability related DWP* payments/applications
number % rank number % rank number % rank number % rank
North East 115,075 6.5 9 69,228 5.7 9 189,628 7.3 9 95,864 7.4 9
North West 298,628 16.9 1 181,182 15.0 2 460,259 17.7 1 238,713 18.3 1
Yorkshire and The
Humber
195,696 11.1 4 117,608 9.7 7 290,549 11.1 5 144,492 11.1 5
East Midlands 159,066 9.0 8 108,282 8.9 8 241,746 9.3 6 116,850 9.0 8
West Midlands 195,608 11.1 5 142,768 11.8 3 322,456 12.4 3 153,508 11.8 4
East 163,623 9.3 7 140,004 11.6 4 240,400 9.2 7 120,952 9.3 6
London 230,771 13.1 3 127,710 10.5 6 324,250 12.4 2 160,802 12.3 2
South East 236,290 13.4 2 186,104 15.4 1 308,010 11.8 4 155,360 11.9 3
South West 168,137 9.5 6 138,324 11.4 5 229,504 8.8 8 117,658 9.0 7
Total 1,762,894 100.0 1,211,210 100.0 2,606,802 100.0 1,304,208 100.0
PIP payments
DLA payments
AA payments
PIP applications
*DWP data for August 2017
b) Census data
12.22 The census asks whether each person has a long-term illness or disability and
whether it affects their day to day activities. The census data proved to be very
strongly related to claimants of AA, PIP and DLA. As census data is more
difficult to use for this type of analysis and only collected every 10 years, it was
felt using the DWP data was, on balance, fairer and simpler.
12.23 Table 12.2 and Table 12.3 show the ranking of the different local authorities
within Yorkshire and Humberside and within London for three types of data
which may predict need for adaptations: the census data on long-term illness,
receipt of AA, DLA and PIP combined and the overall ‘health deprivation and
disability domain’ of IMD (see below). There is a very close correspondence
between census data and benefit receipt, but less so with overall IMD.
c) Index of Multiple Deprivation
124
12.24 This has a separate ‘health deprivation and disability’ domain which does
include receipt of disability related benefits in its construction. Other factors
included are: years of potential life lost; acute morbidity; and a comparative
illness and disability measure. It is more difficult to use in a formula, as it is an
index that ranges from -1.0 to +1.0 and IMD is only updated sporadically. As
the domain was again reasonably closely related to DWP benefit receipt, the
review decided to omit this from further analysis. Furthermore, we were unable
to conclude whether the data sources for the IMD indices are any more robust
than DWP or census data.
124
The Health Deprivation and Disability Domain measures the risk of premature death and the impairment of
quality of life through poor physical or mental health. The domain measures morbidity, disability and premature
mortality but not aspects of behaviour or environment that may be predictive of future health deprivation
129
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
12.25 It is important to remember that all three data sources are only broad-brush
indicators of baseline need for adaptations. Not all people with disabilities or
claiming relevant benefits will need adaptations, either because they have them
already and/or the nature of their disability means that there are no common
adaptations to their home that can be made e.g. for someone with severe
learning difficulties. Similarly, some people who have significant problems and
would benefit from adaptations do not claim the disability related benefits they
would qualify for.
12.26 In common with other surveys that include health/mobility related questions, the
census is likely to underestimate the number of people with long-term health
difficulties, as not all respondents wish their health problems to be recorded.
Table 12.2: Ranking of local authorities by potential need for adaptations, Yorkshire
and Humberside
Rank - IMD
health
deprivation
census rank
(all long term
disability -
limits a lot)
DWP rank -
benefit
receipt*
Barnsley 21 15 14
Bradford 15 19 18
Calderdale 13 11 11
Craven 20 3 3
Doncaster 14 16 16
East Riding of Yorkshire UA 4 13 13
Hambleton 9 5 5
Harrogate 5 6 6
Kingston upon Hull, City of UA 17 12 12
Kirklees 12 17 17
Leeds 19 21 20
North East Lincolnshire UA 1 9 9
North Lincolnshire UA 8 10 10
Richmondshire 7 1 1
Rotherham 16 14 15
Ryedale 11 2 2
Scarborough 3 7 7
Selby 6 4 4
Sheffield 10 20 19
Wakefield 18 18 16
York UA 2 8 8
Note: * receiving AA, DLA or PIP at moment – numbers/lowest rank=1
130
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.3: Ranking of local authorities by potential need for adaptations, London
Rank - IMD
health
deprivation
census rank
(all long term
disability -
limits a lot)
DWP rank -
benefit receipt*
Barking and Dagenham 30 10 11
Barnet 7 32 31
Bexley 9 15 18
Brent 17 29 27
Bromley 6 27 26
Camden 21 9 12
City of London 4 1 1
Croydon 19 33 32
Ealing 20 31 30
Enfield 14 30 33
Greenwich 24 23 25
Hackney 31 20 22
Hammersmith and Fulham 27 6 5
Haringey 22 16 15
Harrow 5 12 9
Havering 12 24 17
Hillingdon 16 19 20
Hounslow 18 13 13
Islington 32 14 19
Kensington and Chelsea 3 4 4
Kingston upon Thames 2 2 2
Lambeth 25 21 23
Lewisham 26 25 24
Merton 8 5 6
Newham 29 28 29
Redbridge 11 26 16
Richmond upon Thames 1 3 3
Southwark 28 22 28
Sutton 10 7 7
Tower Hamlets 33 17 21
Waltham Forest 23 18 14
Wandsworth 13 11 10
Westminster 15 8 8
Note: * receiving AA, DLA or PIP at moment – numbers/lowest rank=1
131

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
2. Adjusting this ‘baseline need’ using factors
12.27 The review examined data sources and the impact of using three different sorts
of factors:
Income/affordability (including housing costs)
Frail elderly
Tenure
a) Income/affordability
12.28 Local authorities have the power to devise their own form of means testing to
decide whether people get support from DFG to pay for all or part of the cost of
their adaptations. Virtually all will ‘passport’ those who are in receipt of the main
means tested benefits, which are:
Income support
Job seekers allowance (income based only)
Employment and Support Allowance (income based only)
Housing Benefit
Council Tax Support
Pension Credit (guarantee element only)
Universal Credit (where rolled out)
Working Tax Credit and/or Child Tax Credit, provided that the annual
income for the purposes of assessing entitlement to the tax credit is less
than £15,050 (in areas where Universal Credit still not ‘live’).
12.29 Some other benefits, like Carers Allowance, involve some means testing
although this is only of income from employment, and using Carers Allowance
will double count disability related benefit receipt. The problem is getting reliable
data on whether people receive any of these.
12.30 The DWP data at local authority level do not cover combinations of benefits
(there will be a lot of double counting, as people will often be claiming more
than one type). The main double counting would be with housing benefit; using
this would mean that the allocation model ran the risk of overestimating need
amongst renters at the expense of owners (who can’t claim housing benefit).
Also, the local level DWP data cannot distinguish between JSA and ESA, which
are income based (i.e. means tested), and those which are contribution based
(i.e. not means tested).
132
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
12.31 There does not appear to be any local authority or even regional level data on
receipt of tax credits through either DWP or HMRC (who administer this
benefit). In future, when Universal Credit (UC) is operating in all areas, it should
be a lot simpler to use this data for working age households, as it covers all
means tested benefits together with working tax credit. However, at the
moment, using this UC data without the data on Tax Credits would result in
bias, given that UC has been rolled out on a local authority by local authority
basis and there are a large number of areas where it is still not ‘live’. We were
unable to find any local authority level data on receipt of Council Tax Support.
12.32 Given the current problems with establishing the number of households or
people in receipt of means tested benefits, we examined the ‘income’ domain
of IMD
125
. The most useful part of this appears to be the number of people in
income deprived households (see Appendix 2 for more information on how this
domain is calculated). If we standardise this by the population, we can create a
very simple low-income factor to adjust the proxy ‘need’ for DFG. This was done
by calculating the proportion of the population who are ‘income deprived’ and
adding 1.
12.33 For comparison, we created an ‘income’ factor using DWP benefit data; in this
case the number of households who were claiming IS, JSA, ESA, PC or UC.
There will be some double counting in certain households and between both
ESA and PIP and between AA and pension credit. The impact of using this
rather than IMD is broadly similar, with more variation apparent within London
(highlighted in Table 12.5) than within Yorkshire and Humberside (Table 12.4).
More detailed investigation would be needed to see how much of these
differences may be due to the roll out of Universal Credit in different areas.
125
The Income Deprivation Domain measures the proportion of the population in an area experiencing
deprivation relating to low income. The definition of low income used includes both those people that are out-of-
work, and those that are in work but who have low earnings (and who satisfy the respective means tests).
133
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.4: Profile of potential affordability of DFG, Yorkshire and Humberside
% income
deprived
rank
% households
in receipt
rank
East Riding of Yorkshire 10.6% 8 16.2% 8
Kingston upon Hull, City of 25.3% 22 32.3% 22
North East Lincolnshire 20.3% 21 27.3% 20
North Lincolnshire 14.7% 9 21.2% 11
York 8.1% 5 13.0% 2
Craven 7.7% 4 14.4% 6
Hambleton 7.4% 3 13.6% 5
Harrogate 7.1% 2 13.5% 4
Richmondshire 6.9% 1 13.1% 3
Ryedale 8.6% 7 16.0% 7
Scarborough 16.1% 15 24.2% 17
Selby 8.5% 6 13.0% 1
Barnsley 17.9% 17 27.6% 21
Doncaster 18.2% 18 25.9% 19
Rotherham 18.3% 19 25.4% 18
Sheffield 16.5% 16 22.7% 13
Bradford 19.9% 20 23.9% 16
Calderdale 15.8% 14 23.6% 15
Kirklees 14.9% 10 21.0% 10
Leeds 15.3% 11 20.6% 9
Wakefield 16.0% 12 23.1% 14
Total 15.7% 13 21.9% 12
IMD income
Receipt of means
tested benefits
134
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.5: Profile of potential affordability of DFG, London
% income
deprived
rank
% households
in receipt
rank
Camden 15.2% 18 19.0% 21
City of London 5.0% 1 9.4% 1
Hackney 20.7% 33 23.4% 32
Hammersmith and Fulham 16.2% 21 23.0% 31
Haringey 19.1% 29 21.3% 28
Islington 18.9% 28 24.1% 34
Kensington and Chelsea 13.3% 13 18.9% 19
Lambeth 17.6% 24 20.6% 26
Lewisham 18.0% 27 20.7% 27
Newham 19.2% 30 18.3% 18
Southwark 17.8% 26 24.0% 33
Tower Hamlets 20.7% 32 22.1% 30
Wandsworth 11.9% 9 14.4% 11
Westminster 15.0% 16 17.7% 14
Barking and Dagenham 21.3% 34 20.4% 24
Barnet 12.0% 10 13.9% 9
Bexley 11.6% 7 14.1% 10
Brent 17.4% 23 19.0% 20
Bromley 10.3% 5 12.6% 4
Croydon 15.0% 17 21.9% 29
Ealing 15.9% 20 18.1% 17
Enfield 19.3% 31 19.2% 23
Greenwich 16.9% 22 20.1% 25
Harrow 11.9% 8 13.4% 6
Havering 12.2% 12 14.9% 12
Hillingdon 12.1% 11 13.3% 5
Hounslow 13.5% 14 19.2% 22
Kingston upon Thames 7.8% 3 10.5% 3
Merton 10.9% 6 13.6% 8
Redbridge 13.6% 15 13.5% 7
Richmond upon Thames 6.6% 2 9.9% 2
Sutton 10.2% 4 16.0% 13
Waltham Forest 17.8% 25 17.9% 15
Total 15.2% 19 17.9% 16
IMD income
Receipt of means
tested benefits
135

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Housing costs
12.34 The review of the allocations model was also tasked with determining how
housing costs could be factored into both the means test and the allocations
model. This is especially challenging, not least because what housing costs
should comprise is subjective e.g. should it be rental or mortgage costs only or
should we include council tax, or should the location, age and type of home be
given consideration, given that these housing characteristics influence
maintenance and upkeep costs. There will also be costs incurred by owners
e.g. maintenance and upkeep and buildings insurance that are not paid directly
by renters but which are likely reflected in their rental payments.
12.35 The ONS has done some work in this area for owner occupiers, which is
explained here:
https://www.ons.gov.uk/economy/inflationandpriceindices/articles/understandingt
hedifferentapproachesofmeasuringowneroccupiershousingcosts/apriltojune2017.
12.36 This may be a useful starting point for considering more work in this area if
Government wishes to consider more depth analysis into housing costs.
12.37 Another important consideration for an allocations model is whether there is
comprehensive, comparable and robust data for both private renters and
registered provider renters, given that the latter provide statistical data returns
to the Homes and Communities Agency
126
and private landlords have no such
obligations.
12.38 Data on private rental costs will vary in coverage (i.e. not all can be analysed at
local authority level), in completeness (i.e. the quantity and nature of missing
data will likely vary) and in data collection methodology. There are several
publicly available sources on the private rental market in the UK, although
access to national survey data can only be accessed via the UK Data Archive.
Main sources include: VOA data
127
, the English Housing Survey and Family
Resources Survey (FRS). Using VOA data would seem the most sensible data
source, but further work would be required to fully assess how it could be
factored in.
12.39 While local housing allowances do give an indicator of rents within an area, the
allowances are based on the 30
th
percentile of rents (i.e. the lower end of the
market only) and use different geographical boundaries to DFG.
12.40 Obtaining data on outstanding mortgage costs and monthly repayments is even
more problematic, and we believe that only national survey data (e.g. EHS and
FRS) could potentially assist with this at regional level only. We know from our
work on the EHS that there are issues with the reliability of respondent data as
126
https://www.gov.uk/government/statistics/statistical-data-return-2016-to-2017.
127
ONS also VOA and other data to produce the Index of Private Housing Rental Prices (IPHRP) which is
considered an experimental data source at present
136

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
well as a notable amount of missing data that makes robust analysis
problematic.
12.41 The English Housing Survey Housing costs and affordability 2015-16 report
128
,
which BRE helped MHCLG to produce, contains analysis of average weekly
housing cost (mortgage/rents) by tenure and by various household
characteristics. The report also shows the average proportion of household
income required to pay for these costs and how this varies according to the
definition of household income e.g. income for the household reference person
(HRP) for the survey only or the HRP and partner income or the income for all
household members who, in theory, could contribute to such costs.
12.42 From the EHS report it is evident that there is both a broad range of average
rental/mortgage costs and a broad range for the proportion of income required
to meet these costs, by tenure and type of household. The region where people
live will, of course, also impact on these averages. The report therefore, seems
to give weight to the suggestion that housing costs are an important issue in
terms of someone’s ability to pay for an adaptation. At the same time, however,
the report also demonstrates the complexity of the task e.g. by demonstrating
how the definition of income (particularly whose income) can impact on findings;
this is a similar issue for the means test.
12.43 In view of the above, it is likely very difficult to apply a simple, transparent and
fair regional or local authority factor into DFG allocations formula to take
account of housing costs.
12.44 To summarise, both the DWP benefit receipt data have disadvantages, and we
believe that the issue of housing costs is far too complex to include within an
allocation formula. However, as it is more regularly updated, transparent and
accessible, we feel that the DWP benefit data provides a better indicator of
relative ‘ability to pay’, and that its disadvantages will reduce once Universal
Credit is live in all areas of England.
3. ‘Frail elderly factor’
12.45 The reviewers felt it was sensible to still include something in the allocations
model to take account of the age of the local population, given that older people
are more likely to need home adaptations, albeit they are also more likely to
have a long-term limiting illness included into the baseline indicator of need.
12.46 Currently, the simplified allocations model includes a component for the
proportion of population aged 60 or over. At minimum, the review recommends
that the current allocations model adjusts the age threshold to an age where
128
Ministry of Housing, Communities and Local Government (2017b) English Housing Survey:
Housing costs and affordability, 2015-16, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2015-to-2016-housing-costs-and-affordability.
137

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
people are eligible for the basic State Pension; although this varies for men and
women, a singular threshold would be simpler to model and administer.
12.47 Within the BCF formula, there is a component for older people that includes a
factor to take account of ‘frail elderly’; in this case defined as the percentage of
all these aged 65 or over who are 90 years old or more. There are grounds for
considering a ‘frail elderly’ factor in a new DFG allocations model to replace the
existing age component; the question is what the age threshold should be. The
BCF approach of taking those at least 90 years old is mainly there to account
for the need for residential care, as a higher proportion of this age group are no
longer living at home.
12.48 This review looked at an approach to include a factor to take account of the
proportion of people aged 75 or over in the sensitivity testing, but this ‘frail
elderly’ threshold could be changed. This data comes from population age
statistics from the census which are regularly updated by projections. For this
research we have taken an average of the estimates produced for 2014-2023.
We decided to take the percentage of the total population aged 75 or older
which was converted into a simple factor by adding 1.0.
a) Tenure
12.49 Only people who are home owners, registered provider renters or private
renters can apply for a DFG, so the formula needs to take account of the fact
that the proportion of local authority stock varies considerably by local authority,
with a number having no stock at all following Large Scale Voluntary Transfer
(LSVT). It is relatively simple to construct a factor to adjust the proxy ‘need’
using the proportion of eligible tenure dwellings in the local authority area. This
uses MHCLG data on stock by tenure and local authority area and is updated
annually.
12.50 The data on grant recipients suggests that a disproportionate number of grants
go to registered provider tenants, although it is unclear whether a
disproportionate amount of the total budget goes to these tenants as well. This
is not surprising as the shortage of social housing in most areas means that it
is rationed to those most in need (including people with disabilities) and
registered provider homes are proactively managed by staff who have a good
knowledge of the council services and grants available.
12.51 Home owners may not be aware DFG exists unless they find out about it by
chance (e.g. after being referred to social services after a fall, from
friends/neighbours or advice agencies). Private tenants may be even less likely
to be aware of DFG’s and require the permission of their landlord to carry out
any works. Whether the DFG allocation system should try to address this by
accepting the current barriers to private sector occupiers and giving more
money to local authorities with a large proportion of register provider stock or
whether it should try to be equitable between tenures and consider measures
138
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
to increase awareness and take-up in the private sector is something that needs
full and careful consideration.
4. The new baseline and impact of adding each factor
12.52 A new ‘baseline’ need was created, based on the total number of people
receiving DLA, PIP or AA within that area. We looked at how this affected the
relative need between regions and within the two selected regions: Yorkshire
and Humberside; and London. We then calculated new allocations based on
this by splitting the existing pot
129
(for that region or England as a whole)
according to the proportion of all claimants within the local authority/region.
12.53 Looking first at the baseline position for each overall region (Table12.6), this
looks rather different from their current share of the national allocation, with
greater need in the North West, East Midlands and North East than suggested
by current allocations, and lesser need in Yorkshire and Humber and the South
East.
Table 12.6: Baseline ‘need’ by region and current allocation share
Baseline
need
Proportion of
total pot
allocation -
baseline need
current 2016
allocation
change in £
% change
(as % of current)
North East 280,167 0.065 £25,801,250 £21,738,299 £4,062,951 18.7
North West 718,523 0.168 £66,170,504 £39,216,448 £26,954,056 68.7
Yorkshire and The Humber 457,796 0.107 £42,159,530 £67,931,075 -£25,771,545 -37.9
East Midlands 384,198 0.090 £35,381,714 £27,953,686 £7,428,028 26.6
West Midlands 491,884 0.115 £45,298,776 £48,918,976 -£3,620,200 -7.4
East 424,579 0.099 £39,100,497 £35,533,186 £3,567,311 10.0
London 519,283 0.121 £47,822,015 £51,520,879 -£3,698,864 -7.2
South East 577,754 0.135 £53,206,750 £63,110,289 -£9,903,539 -15.7
South West 424,119 0.099 £39,058,135 £38,077,162 £980,972 2.6
Total 4,278,312 1.000 £394,000,000 £394,000,000 £0 0.0
12.54 The picture within the two regions examined in detail is also rather different. In
Yorkshire and Humberside, baseline need is indicated to be much greater in
some areas, although there is no pattern of more/less money for metropolitan
areas as opposed to more rural authorities (Table 12.7). Baseline need is
significantly lower in North East Lincolnshire, North Lincolnshire, Craven,
Ryedale and Calderdale and significantly higher in Hambleton, Harrogate,
Selby, Doncaster and Sheffield.
129
Based on 2016/17 DFG allocations -termed ‘current allocation’ for ease of reading.
139
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.7: Yorkshire and Humberside - baseline ‘need’ by local authority and
current allocation share
Note: changes of 15% or more highlighted
Baseline
need
Proportion of
total pot
allocation -
baseline need
current 2016
allocation
change in £
% change
(as % of
current)
East Riding of Yorkshire 25,467 0.056 £2,181,614 £2,127,454 £54,160 2.546
Kingston upon Hull, City of 24,200 0.053 £2,073,077 £1,968,062 £105,015 5.336
North East Lincolnshire 14,936 0.033 £1,279,483 £2,188,308 -£908,825 -41.531
North Lincolnshire 15,108 0.033 £1,294,217 £1,763,122 -£468,905 -26.595
York 11,032 0.024 £945,049 £1,003,471 -£58,422 -5.822
Craven 3,855 0.008 £330,236 £433,307 -£103,071 -23.787
Hambleton 5,797 0.013 £496,596 £375,828 £120,768 32.134
Harrogate 9,448 0.021 £809,357 £571,343 £238,014 41.659
Richmondshire 2,988 0.007 £255,965 £212,493 £43,472 20.458
Ryedale 3,467 0.008 £296,998 £452,569 -£155,571 -34.375
Scarborough 10,793 0.024 £924,575 £1,145,100 -£220,525 -19.258
Selby 5,647 0.012 £483,747 £346,958 £136,788 39.425
Barnsley 28,974 0.063 £2,482,038 £2,330,936 £151,102 6.482
Doncaster 30,711 0.067 £2,630,837 £1,965,353 £665,485 33.861
Rotherham 29,367 0.064 £2,515,705 £2,119,269 £396,436 18.706
Sheffield 51,263 0.112 £4,391,411 £3,509,204 £882,207 25.140
Bradford 43,685 0.095 £3,742,247 £3,519,468 £222,779 6.330
Calderdale 15,866 0.035 £1,359,150 £2,063,214 -£704,064 -34.125
Kirklees 34,678 0.076 £2,970,668 £2,483,091 £487,577 19.636
Leeds 56,263 0.123 £4,819,733 £5,630,909 -£811,176 -14.406
Wakefield 34,247 0.075 £2,933,747 £3,006,990 -£73,243 -2.436
Total 457,792 1.000 £39,216,448 £39,216,448 £0 0.000
12.55 For London, there is more of a clear pattern with baseline need tending to be
higher than current allocations in inner London and lower in Outer London
(Table 12.8).
140
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.8: London - baseline ‘need’ by local authority and current allocation share
Note: changes of 15% or more highlighted
Baseline
need
Proportion of
total pot
allocation -
baseline need
current 2016
allocation
change in £
% change
(as % of
current)
Camden 14,900 0.029 £1,478,278 £727,538 £750,740 103.189
City of London 290 0.001 £28,772 £26,313 £2,459 9.344
Hackney 18,394 0.035 £1,824,930 £1,184,865 £640,065 54.020
Hammersmith and Fulham 10,076 0.019 £999,673 £1,018,510 -£18,837 -1.849
Haringey 16,726 0.032 £1,659,442 £1,818,183 -£158,742 -8.731
Islington 17,097 0.033 £1,696,250 £1,318,486 £377,764 28.651
Kensington and Chelsea 8,033 0.015 £796,981 £666,726 £130,255 19.536
Lambeth 18,701 0.036 £1,855,388 £1,145,265 £710,123 62.005
Lewisham 18,859 0.036 £1,871,064 £1,053,080 £817,984 77.675
Newham 20,000 0.039 £1,984,266 £1,932,506 £51,761 2.678
Southwark 19,726 0.038 £1,957,082 £1,149,371 £807,711 70.274
Tower Hamlets 17,495 0.034 £1,735,737 £1,572,542 £163,195 10.378
Wandsworth 14,584 0.028 £1,446,927 £1,199,531 £247,396 20.624
Westminster 13,647 0.026 £1,353,964 £1,182,326 £171,639 14.517
Barking and Dagenham 14,737 0.028 £1,462,107 £1,264,509 £197,598 15.626
Barnet 20,774 0.040 £2,061,057 £1,971,131 £89,926 4.562
Bexley 17,001 0.033 £1,686,726 £2,023,569 -£336,844 -16.646
Brent 19,578 0.038 £1,942,398 £3,599,500 -£1,657,102 -46.037
Bromley 19,132 0.037 £1,898,149 £1,680,928 £217,222 12.923
Croydon 24,909 0.048 £2,471,304 £2,046,194 £425,110 20.776
Ealing 20,360 0.039 £2,019,983 £2,529,769 -£509,785 -20.151
Enfield 21,301 0.041 £2,113,343 £2,542,222 -£428,880 -16.870
Greenwich 18,935 0.036 £1,878,604 £1,941,443 -£62,838 -3.237
Harrow 14,260 0.027 £1,414,782 £1,180,502 £234,280 19.846
Havering 16,900 0.033 £1,676,705 £1,426,010 £250,695 17.580
Hillingdon 17,401 0.034 £1,726,411 £3,456,593 -£1,730,182 -50.055
Hounslow 15,153 0.029 £1,503,379 £2,033,255 -£529,875 -26.060
Kingston upon Thames 7,655 0.015 £759,478 £1,032,341 -£272,864 -26.432
Merton 10,159 0.020 £1,007,908 £989,719 £18,189 1.838
Redbridge 16,830 0.032 £1,669,760 £1,659,392 £10,368 0.625
Richmond upon Thames 8,004 0.015 £794,103 £1,307,463 -£513,359 -39.264
Sutton 11,820 0.023 £1,172,701 £1,233,241 -£60,539 -4.909
Waltham Forest 15,857 0.031 £1,573,226 £1,607,858 -£34,632 -2.154
Total 519,294 1.000 £51,520,879 £51,520,879 £0 0.000
12.56 It is interesting that the relative baseline need indicated by receipt of disability
related benefits differs so much from the current DFG allocations when the
method for existing allocations uses receipt of disability related benefits as its
baseline. There are probably two main reasons for this difference:
The new baseline does not include out of work income replacement benefits
for those deemed unable to work due to health and disability – previously
invalidity benefit and now ESA.
The criteria for receiving PIP are subtly different, and in some aspects more
stringent, than those for receiving DLA which it replaced. There has been
considerable controversy about the face to face assessment process for PIP
141
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
and the many perceived harsh decisions that have been made, and the high
success rate of mandatory reconsiderations and full appeals against the
initial DWP assessments.
12.57 We added each of the 3 factors (low income, frail elderly and tenure) in turn to
examine the impact of each stage. All were given equal weight, which may or
may not be the best approach, although it does illustrate the direction of any
shifts.
Table 12.9: Overall Regions – modelled amounts at each stage
Baseline
need plus income
plus income and
elderly
plus income,
elderly and
tenure
current 2016
allocation
North East £25,801,250 £27,510,015 £27,610,168 £27,310,654 £21,738,299
North West £66,170,504 £69,019,952 £69,009,411 £71,979,448 £39,216,448
Yorkshire and The Humber £42,159,530 £42,945,336 £42,930,066 £41,512,036 £67,931,075
East Midlands £35,381,714 £35,017,484 £35,105,520 £34,278,329 £27,953,686
West Midlands £45,298,776 £45,965,111 £46,045,602 £45,263,348 £48,918,976
East £39,100,497 £37,684,408 £37,932,538 £38,268,033 £35,533,186
London £47,822,015 £47,093,071 £45,662,458 £43,341,554 £51,520,879
South East £53,206,750 £50,575,282 £50,859,031 £52,009,113 £63,110,289
South West £39,058,135 £38,189,340 £38,845,205 £40,037,485 £38,077,162
Total £394,000,000 £394,000,000 £394,000,000 £394,000,000 £394,000,000
new allocation with same total pot
Table 12.10: Overall Regions – difference from current allocation share
Baseline need plus income
plus income
and elderly
plus income,
elderly and
tenure
North East £4,062,951 £5,771,716 £5,871,869 £5,572,355
North West £26,954,056 £29,803,504 £29,792,963 £32,763,000
Yorkshire and The Humber -£25,771,545 -£24,985,739 -£25,001,009 -£26,419,039
East Midlands £7,428,028 £7,063,798 £7,151,834 £6,324,643
West Midlands -£3,620,200 -£2,953,865 -£2,873,373 -£3,655,628
East £3,567,311 £2,151,222 £2,399,352 £2,734,847
London -£3,698,864 -£4,427,808 -£5,858,421 -£8,179,325
South East -£9,903,539 -£12,535,006 -£12,251,257 -£11,101,175
South West £980,972 £112,178 £768,043 £1,960,323
Total £0 £0 £0 £0
Change from current allocation
Note: negative=less money than 2016/17
12.58 Looking at the regions where the estimates show most change, it is clear that
different factors are having more effect in different areas. For example, in the
142
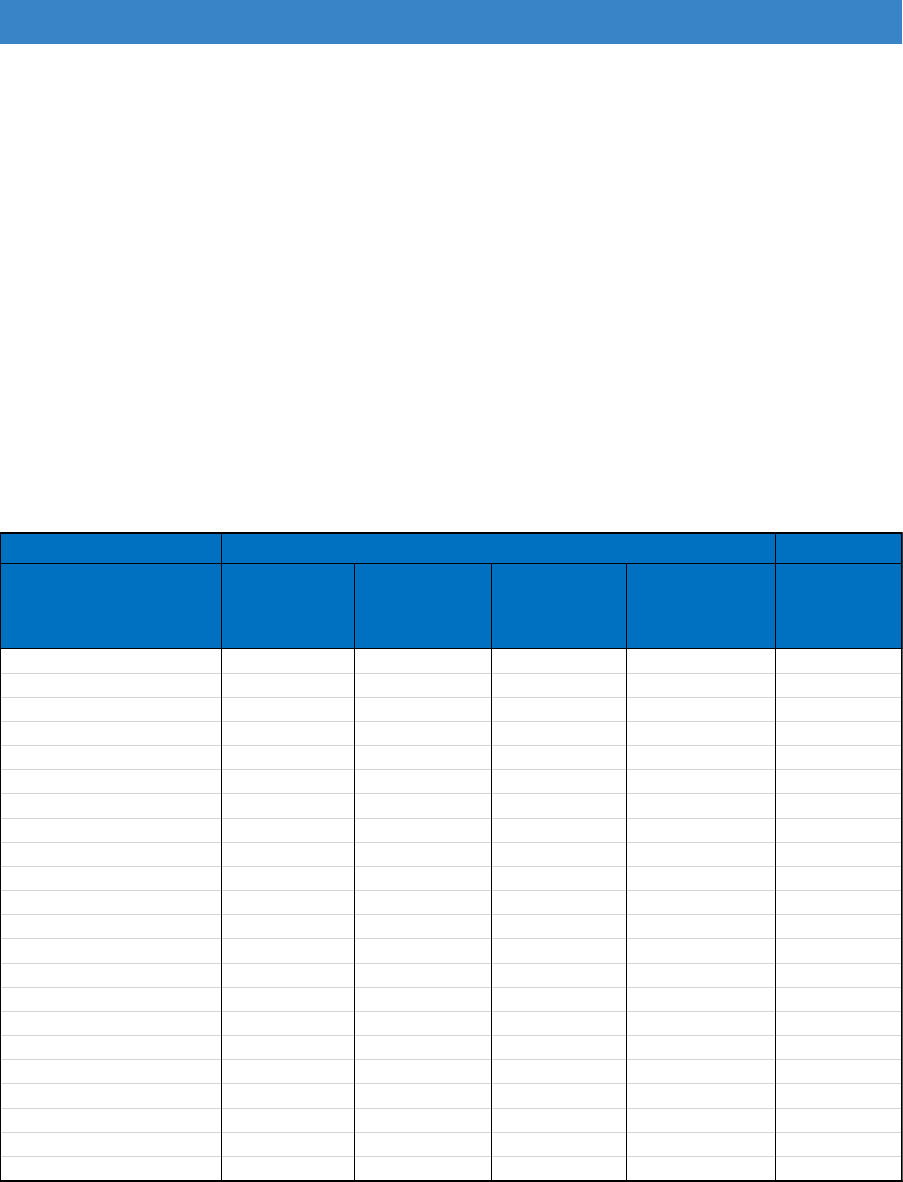
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
North West, the baseline itself is much higher and gets a big uplift on this
compared with the income and, especially, the tenure factors. In the North East,
the main uplift to the baseline is from the income factor. For those regions where
need is estimated to be significantly lower than the current model, again we can
see the different impact of the factors. For Yorkshire and Humberside, the huge
change to the baseline is exaggerated further when the tenure factor is added,
whereas for the South East, the main reduction to the lower baseline comes
with adding the income factor. Applying the tenure factor at the final stage helps
to reduce the losses somewhat.
12.59 Table 12.11 and Table 12.12 examine the modelled impacts of each factor for
the local authorities within the Yorkshire and Humberside region.
Table 12.11: Yorkshire and Humberside– modelled amounts at each stage
Baseline
need plus income
plus income and
elderly
plus income,
elderly and tenure
current 2016
allocation
East Riding of Yorkshire £2,181,614 £2,079,474 £2,139,202 £2,195,015 £2,127,454
Kingston upon Hull, City of £2,073,077 £2,248,609 £2,212,070 £1,944,883 £1,968,062
North East Lincolnshire £1,279,483 £1,335,428 £1,347,573 £1,492,913 £2,188,308
North Lincolnshire £1,294,217 £1,286,013 £1,297,706 £1,437,671 £1,763,122
York £945,049 £876,038 £877,235 £886,502 £1,003,471
Craven £330,236 £309,812 £321,732 £356,480 £433,307
Hambleton £496,596 £462,819 £478,436 £530,109 £375,828
Harrogate £809,357 £753,197 £774,317 £811,242 £571,343
Richmondshire £255,965 £237,494 £239,548 £247,989 £212,493
Ryedale £296,998 £282,444 £292,039 £323,580 £452,569
Scarborough £924,575 £941,584 £976,868 £1,082,372 £1,145,100
Selby £483,747 £448,306 £449,875 £457,905 £346,958
Barnsley £2,482,038 £2,597,473 £2,598,507 £2,382,801 £2,330,936
Doncaster £2,630,837 £2,715,339 £2,719,558 £2,554,325 £1,965,353
Rotherham £2,515,705 £2,587,290 £2,596,968 £2,359,306 £2,119,269
Sheffield £4,391,411 £4,419,187 £4,388,546 £4,055,712 £3,509,204
Bradford £3,742,247 £3,802,704 £3,738,680 £4,138,943 £3,519,468
Calderdale £1,359,150 £1,377,591 £1,372,881 £1,520,833 £2,063,214
Kirklees £2,970,668 £2,946,672 £2,925,055 £2,839,257 £2,483,091
Leeds £4,819,733 £4,767,253 £4,707,865 £4,351,946 £5,630,909
Wakefield £2,933,747 £2,961,554 £2,963,420 £3,282,177 £3,006,990
Total £39,216,448 £39,216,448 £39,216,448 £39,216,448 £39,216,448
new allocation with same total pot
12.60 It appears that the tenure factor is having a greater effect than either low income
or frail elderly – this is simply because there is more variation in this factor than
in the other two. In some cases, e.g. North East Lincolnshire, the addition of the
tenure factor acts to reduce the large losses to some extent, whereas the
opposite happens for Leeds, where adding the tenure factor increases the
losses further.
143
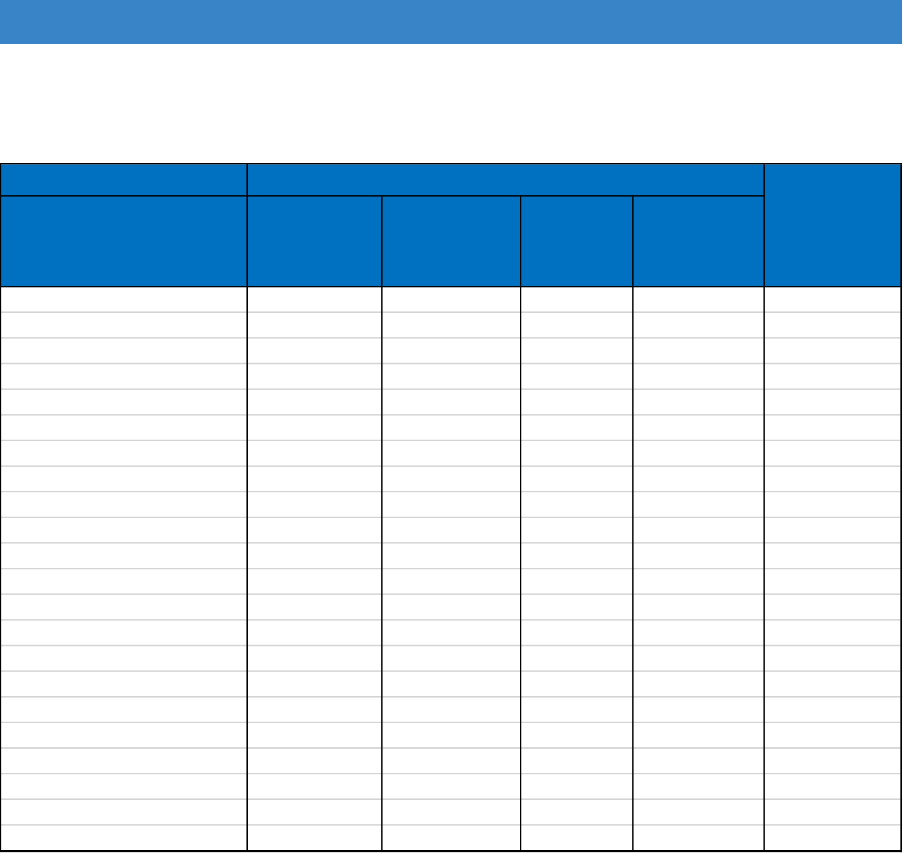
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.12: Yorkshire and Humberside – difference from current allocation share
baseline need plus income
plus income
and elderly
plus income,
elderly and
tenure
East Riding of Yorkshire £54,160 -£47,979 £11,748 £67,561
Kingston upon Hull, City of £105,015 £280,548 £244,008 -£23,178
North East Lincolnshire -£908,825 -£852,880 -£840,735 -£695,395 big loss
North Lincolnshire -£468,905 -£477,109 -£465,416 -£325,451 moderate loss
York -£58,422 -£127,432 -£126,235 -£116,969
Craven -£103,071 -£123,495 -£111,575 -£76,827
Hambleton £120,768 £86,991 £102,608 £154,280
Harrogate £238,014 £181,854 £202,974 £239,899 moderate gain
Richmondshire £43,472 £25,001 £27,055 £35,496
Ryedale -£155,571 -£170,125 -£160,530 -£128,989
Scarborough -£220,525 -£203,516 -£168,232 -£62,728
Selby £136,788 £101,348 £102,916 £110,947
Barnsley £151,102 £266,537 £267,571 £51,865
Doncaster £665,485 £749,987 £754,206 £588,972 big gain
Rotherham £396,436 £468,021 £477,699 £240,037 moderate gain
Sheffield £882,207 £909,983 £879,342 £546,509 big gain
Bradford £222,779 £283,236 £219,212 £619,475 big gain
Calderdale -£704,064 -£685,623 -£690,333 -£542,381 big loss
Kirklees £487,577 £463,581 £441,963 £356,166 moderate gain
Leeds -£811,176 -£863,656 -£923,044 -£1,278,962 big loss
Wakefield -£73,243 -£45,436 -£43,569 £275,188 moderate gain
Total £0 £0 £0 £0
Change from current allocation
Note: negative=less money than 2016/17
12.61 The largest overall reduction in allocation applying this method would be for
Leeds, where the baseline is estimated to be very much lower and the losses
just seem to get bigger as each of the other factors is applied; especially the
tenure factor at the end. The largest increases would be for Sheffield and
Bradford – it is interesting to note that applying the tenure factor at the end
significantly decreases the allocation for the former and increases it for the
latter. The findings from Table 12.12 is shown graphically in Figure 12.2.
144
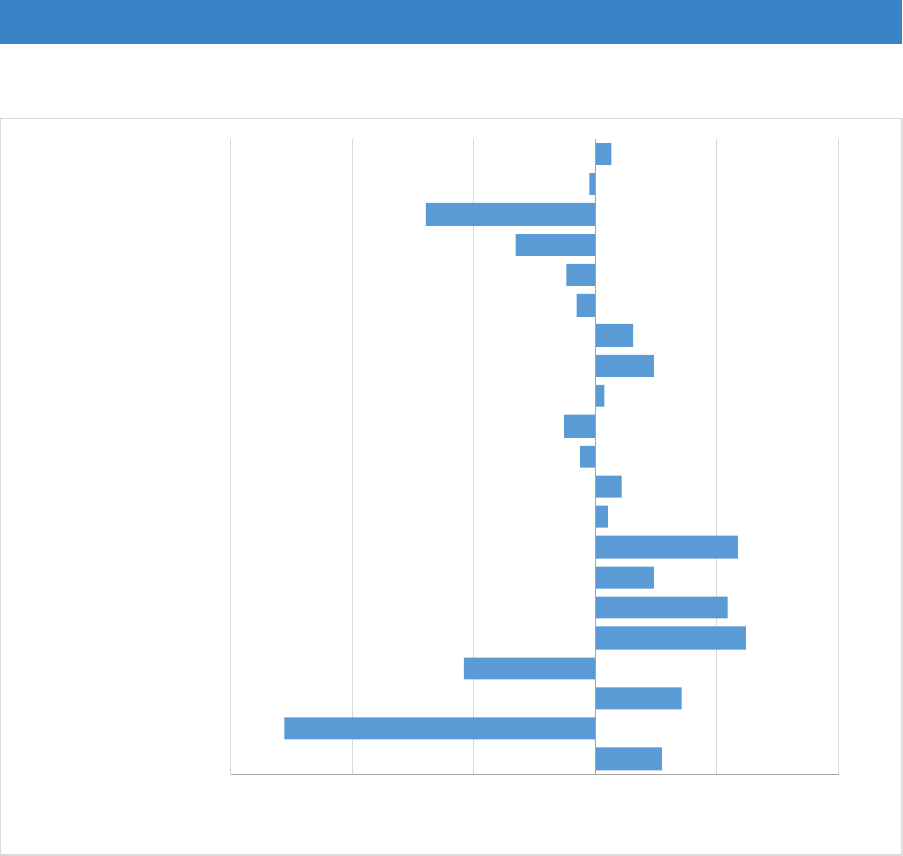
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 12.2: Yorkshire and Humberside – differences from current allocations
-£1,500,000 -£1,000,000 -£500,000 £0 £500,000 £1,000,000
East Riding of Yorkshire
Kingston upon Hull, City of
North East Lincolnshire
North Lincolnshire
York
Craven
Hambleton
Harrogate
Richmondshire
Ryedale
Scarborough
Selby
Barnsley
Doncaster
Rotherham
Sheffield
Bradford
Calderdale
Kirklees
Leeds
Wakefield
change from current allocation
12.62 Table 12.13 and Table 12.14 examine the modelled impacts of each factor for
the local authorities within London.
12.63 It is interesting to see that the final stage of factoring in the percentage of stock
that is not LA owned has a very big impact for some authorities; most notably
Southwark where around 30% of stock is still owned by the local authority. Here,
and in other boroughs with a high proportion of local authority homes, e.g.
Camden, Hackney and Islington the tenure factor acts to ‘dampens down’ to
some extent the very significant increases in estimated need.
145
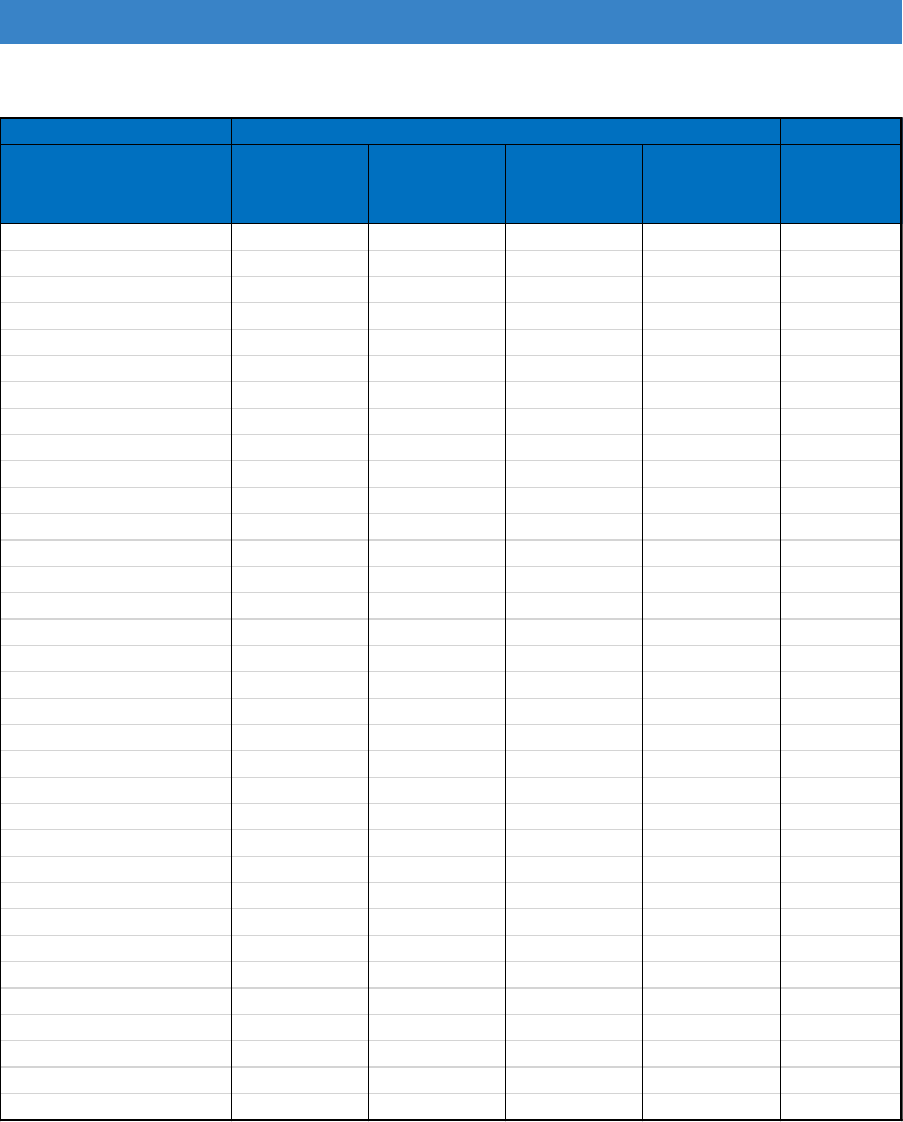
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.13: London– modelled amounts at each stage
Baseline
need plus income
plus income and
elderly
plus income,
elderly and
tenure
current 2016
allocation
Camden £1,478,278 £1,492,031 £1,490,917 £1,302,448 £727,538
City of London £28,772 £26,704 £26,918 £28,266 £26,313
Hackney £1,824,930 £1,910,794 £1,869,796 £1,675,795 £1,184,865
Hammersmith and Fulham £999,673 £1,042,635 £1,035,054 £999,862 £1,018,510
Haringey £1,659,442 £1,707,438 £1,686,900 £1,631,381 £1,818,183
Islington £1,696,250 £1,784,916 £1,758,000 £1,480,399 £1,318,486
Kensington and Chelsea £796,981 £804,148 £814,849 £847,404 £666,726
Lambeth £1,855,388 £1,897,513 £1,863,715 £1,740,032 £1,145,265
Lewisham £1,871,064 £1,915,406 £1,893,689 £1,887,293 £1,053,080
Newham £1,984,266 £1,991,520 £1,946,741 £1,879,336 £1,932,506
Southwark £1,957,082 £2,059,245 £2,021,057 £1,603,998 £1,149,371
Tower Hamlets £1,735,737 £1,797,321 £1,749,319 £1,767,349 £1,572,542
Wandsworth £1,446,927 £1,403,636 £1,387,682 £1,380,518 £1,199,531
Westminster £1,353,964 £1,351,824 £1,353,035 £1,379,082 £1,182,326
Barking and Dagenham £1,462,107 £1,492,669 £1,477,594 £1,258,976 £1,264,509
Barnet £2,061,057 £1,991,650 £2,018,501 £2,116,485 £1,971,131
Bexley £1,686,726 £1,631,912 £1,674,355 £1,889,977 £2,023,569
Brent £1,942,398 £1,960,461 £1,959,444 £2,055,353 £3,599,500
Bromley £1,898,149 £1,812,824 £1,866,566 £2,106,023 £1,680,928
Croydon £2,471,304 £2,554,534 £2,573,324 £2,645,366 £2,046,194
Ealing £2,019,983 £2,023,239 £2,027,110 £2,068,846 £2,529,769
Enfield £2,113,343 £2,136,872 £2,153,260 £2,230,206 £2,542,222
Greenwich £1,878,604 £1,913,862 £1,900,039 £1,713,411 £1,941,443
Harrow £1,414,782 £1,361,481 £1,386,258 £1,479,639 £1,180,502
Havering £1,676,705 £1,633,728 £1,691,620 £1,725,816 £1,426,010
Hillingdon £1,726,411 £1,659,887 £1,673,265 £1,715,535 £3,456,593
Hounslow £1,503,379 £1,520,622 £1,515,684 £1,485,445 £2,033,255
Kingston upon Thames £759,478 £711,957 £720,424 £754,757 £1,032,341
Merton £1,007,908 £971,044 £973,675 £1,098,272 £989,719
Redbridge £1,669,760 £1,607,796 £1,612,479 £1,740,743 £1,659,392
Richmond upon Thames £794,103 £740,387 £750,734 £847,413 £1,307,463
Sutton £1,172,701 £1,153,700 £1,173,890 £1,227,993 £1,233,241
Waltham Forest £1,573,226 £1,573,691 £1,565,184 £1,595,272 £1,607,858
Total £51,520,879 £51,520,879 £51,520,879 £51,520,879 £51,520,879
new allocation with same total pot
12.64 Looking at the two biggest ‘losers’ with a new method (Brent and Hillingdon)
highlights the inequity of the allocation system used up until 2010 and which still
influences allocations today. Between them, they house about 7% of the total
population of London but are being allocated 14% of the total DFG funds for
London. This can be traced back to the allocations for 2010/11, when both
authorities bid for and received allocations at more than double the needs formula
in use at the time.
146
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
12.65 In contrast, the biggest ‘winners’ with a new method (Lewisham and Camden)
received less than half of their ‘need’ due to placing low bids in 2010/11.
Table 12.14: London – difference from current allocation
baseline need plus income
plus income
and elderly
plus income,
elderly and
tenure
Camden £750,740 £764,493 £763,379 £574,910 big gain
City of London £2,459 £391 £605 £1,953
Hackney £640,065 £725,929 £684,931 £490,930 big gain
Hammersmith and Fulham -£18,837 £24,125 £16,543 -£18,648
Haringey -£158,742 -£110,745 -£131,283 -£186,803
Islington £377,764 £466,430 £439,514 £161,914
Kensington and Chelsea £130,255 £137,422 £148,123 £180,678
Lambeth £710,123 £752,249 £718,450 £594,767 big gain
Lewisham £817,984 £862,326 £840,609 £834,213 big gain
Newham £51,761 £59,015 £14,235 -£53,170
Southwark £807,711 £909,874 £871,686 £454,627 big gain
Tower Hamlets £163,195 £224,780 £176,777 £194,808
Wandsworth £247,396 £204,106 £188,151 £180,987
Westminster £171,639 £169,498 £170,710 £196,756
Barking and Dagenham £197,598 £228,160 £213,085 -£5,533
Barnet £89,926 £20,519 £47,370 £145,354
Bexley -£336,844 -£391,658 -£349,215 -£133,592
Brent -£1,657,102 -£1,639,039 -£1,640,056 -£1,544,147 very big loss
Bromley £217,222 £131,896 £185,639 £425,096 moderate gain
Croydon £425,110 £508,339 £527,129 £599,171 big gain
Ealing -£509,785 -£506,530 -£502,658 -£460,923 moderate loss
Enfield -£428,880 -£405,350 -£388,963 -£312,016 moderate loss
Greenwich -£62,838 -£27,581 -£41,403 -£228,032
Harrow £234,280 £180,979 £205,756 £299,137 moderate gain
Havering £250,695 £207,718 £265,610 £299,807 moderate gain
Hillingdon -£1,730,182 -£1,796,706 -£1,783,329 -£1,741,058 very big loss
Hounslow -£529,875 -£512,633 -£517,571 -£547,809 big loss
Kingston upon Thames -£272,864 -£320,384 -£311,917 -£277,584 moderate loss
Merton £18,189 -£18,675 -£16,044 £108,553
Redbridge £10,368 -£51,597 -£46,913 £81,350
Richmond upon Thames -£513,359 -£567,076 -£556,729 -£460,050 moderate loss
Sutton -£60,539 -£79,541 -£59,350 -£5,248
Waltham Forest -£34,632 -£34,167 -£42,673 -£12,586
Total £0 £0 £0 £0
Change from current allocation
Note: negative=less money than 2016/17
147
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
12.66 The findings from Table 12.14 are shown graphically below in Figure 12.3 and
Figure 12.4 for outer and inner London authorities respectively. Note that the
axis scale for the ‘change from current allocation’ is different for each graph,
owing to the far larger values for the outer London authorities.
Figure 12.3: Outer London – differences from current allocations
-2,000,000 -1,500,000 -1,000,000 -500,000 0 500,000 1,000,000
Barking and Dagenham
Barnet
Bexley
Brent
Bromley
Croydon
Ealing
Enfield
Greenwich
Harrow
Havering
Hillingdon
Hounslow
Kingston upon Thames
Merton
Redbridge
Richmond upon Thames
Sutton
Waltham Forest
change from current allocation
148
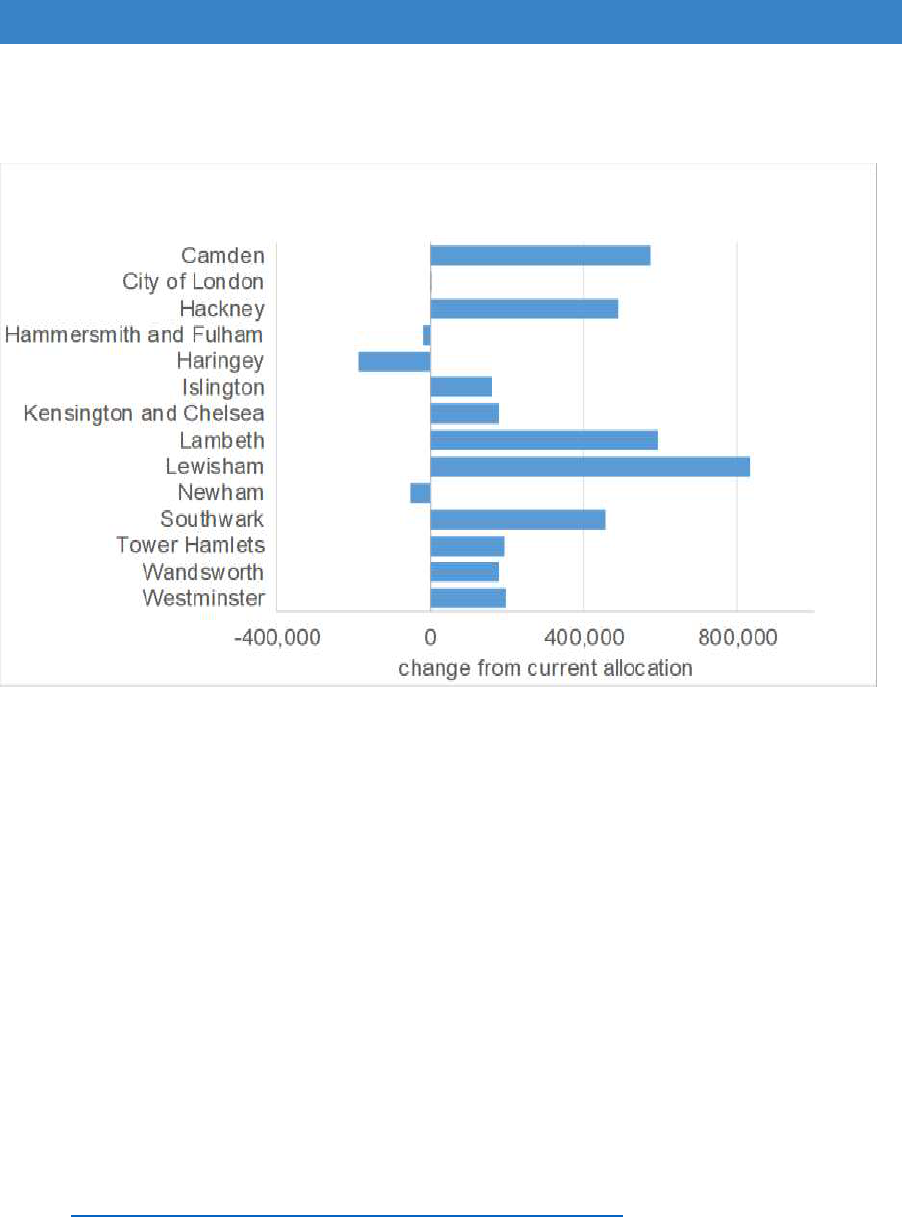
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 12.4: Inner London – differences from current allocations
Building costs/cost of adaptations
12.67 The 2011 BRE review found no firm evidence for regional differences in costs
of adaptations due to variations in the dwelling profile (age and types of homes)
of the housing stock in each region. However, average costs for DFG works
examined at the time of the 2011 review and via the data obtained in this review
show some variation by region for similar type of work. Both the full and
simplified allocation models recommended in the 2011 review included a factor
for variations in building costs (BCIS tender price index).
12.68 There are likely to be several sources for data on building cost variation, such
as the BCIS which requires a subscription. This review found details of UK
Construction Cost Regional Variations via:
https://www.costmodelling.com/regional-variations. The indices set out in this
website are given in Table 12.14
149
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 12.14: Building cost variations by region
Region
Index
North East
100
North West
97
Yorkshire and Humberside
95
West Midlands
92
East Midlands
94
East Anglia
100
South West
100
South East
109
Outer London
105
Inner London
111
UK National Average
100
Note: based on 1Q 2018 where Year 2000 = 100
12.69 There are possible other advantages in including a building cost factor:
If we link the upper limit of the DFG to regional building costs to overcome
the disparity in costs for larger extensions, it would probably make sense to
reflect this in an allocation formula.
The use of building cost would likely ‘dampen’ the potential changes in DFG
allocations, should the allocations model change using the factors examined
in this review. However, it would have little impact on the main ‘winner’
(North West) and would actually reduce the allocation of the main ‘loser’
(Yorkshire and the Humber) further still.
12.70 It is important to note, however, that building prices can be influenced
significantly by local market conditions, and by the size, location and
specification of the building works. Furthermore, some local authorities may be
able to organise their contractual obligations to procure work in cost-effective
ways e.g. gaining a discounted fee for work by using one supplier.
Consequently, building costs indices can only provide an indicative guide of
regional variations.
Summary points – allocation of resources
12.71 These are the main themes highlighted by the review into the DFG allocation
methodology.
1. There are concerns of a possible misalignment between government
funding for DFG and actual expenditure on DFG at local level. This review
therefore needed to examine whether the current allocations methodology used
for DFG funding uplifts is still fit for purpose.
150

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
2. It is important to recognise that under-spending by some local authorities
and overspending by others is not solely due to current allocations being
a poor reflection of need. There are a number of other factors including the
efficiency and resourcing of the whole DFG process from initial referral to
commissioning of the work which are probably more important determinants of
this. For this reason, we suggest that it is important for commissioning groups
to monitor underspend and to understand the reasons for this so appropriate
action can be taken e.g. extra support for individual local authorities, resource
pooling or co-operative working and even re-allocation of funds within an area.
3. There are no robust data that can accurately predict the need for DFG at
regional or local level. The available data can only act as proxy indicators of
that need.
4. The data used for any allocation formula should be simple, transparent,
fair and as robust as possible while responsive to changes in the population
and their circumstances.
5. If a new allocations model were to only include a baseline proxy indicator for
potential need for home adaptations, the allocations would likely change
markedly at both regional level and local authority level. The introduction of
additional factors for ability to pay and age/frailty would obviously change
the distribution of funding further, but the introduction of a tenure factor
can cause marked changes in relative potential need due to the large
variations in the proportion of local authority owned stock.
6. In view of the marked impact of a tenure factor upon allocations and the varied
approach by registered providers in meeting their tenants’ need to home
adaptations, should the DFG allocation system try to address this by accepting
the current barriers to private sector occupiers and giving more money to local
authorities with a large proportion of housing association stock?
Alternatively, should the allocation try to be equitable between tenures and
consider measures to increase awareness and take-up in the private
sector?
7. Given the difficulties in fine tuning allocations to need, our review recommends
that there should consideration of more collaborate DFG funding
arrangements among BCF partners to ensure the most effective use of
resources and more cross local authority collaborations. Using joint pots of
funds would also assist local authorities to meet the need for expensive
adaptions often required for children.
8. The review used disability related DWP data to establish a baseline proxy
indicator of needs, due to its transparency and regularity of update. Although
the DWP data likely underestimates the prevalence of long-term illness (e.g.
issues with take-up of benefits), it is probably no less robust than other potential
data sources.
9. The review also introduced other factors of potential DFG need and
examined their impact on allocations. These factors were: ability to pay
151

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
(using DWP income-based data), frail elderly (census population – predictive
data) and tenure (MHCLG data). These were given equal weight, but this may
not be the best approach and requires further consideration and sensitivity
testing. Are the factors considered by the review for the formula sensible?
I. Should the formula include the income indicator? Working age
people with a disability are more likely to have relatively lower incomes
but this applies less to older people.
II. Should the formula include an age factor and if so, what should the
threshold be? Including an age factor is likely to take funds away from
‘younger’ regions like London but on the other hand, older people are
more likely to need adaptations.
10.The use of regional building costs should be given serious consideration,
although these will not reflect local market conditions and variations in
procurement strategies.
11.Including housing costs into a new allocation formula is problematic due
to lack of robust data. Housing costs may be difficult to define (because there
is potential for any definition to be unfair) and are incredibly varied by tenure
and among different types of households.
12.More sensitivity analysis is needed to look at impact of factors across regions
and all local authorities.
13.Any change in allocation methodology is likely to result in significant ‘winners’
and ‘losers’ due to the impact of bids made in 2010/11 that still influence
allocations today. A new allocation formula would need to be incrementally
introduced over a number of years to allow the biggest ‘winners’ and
‘losers’ to compensate.
Recommendations - allocation of resources
That the allocation formula options are explored further using sensitivity
analysis.
That a new allocation formula is established for the next Comprehensive
Spending Review and is applied incrementally over the implementation
period of that Review.
152
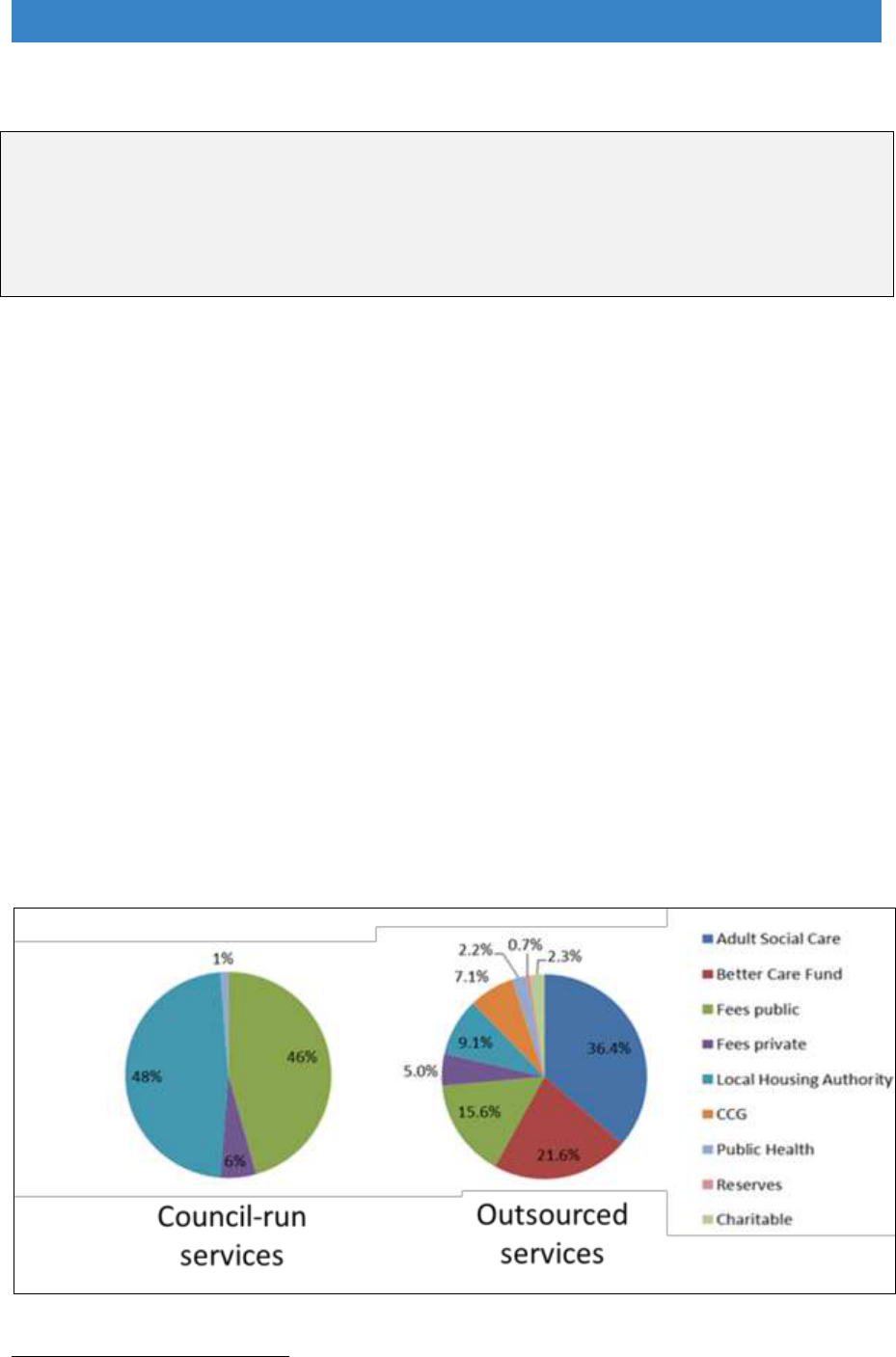
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 13. Other funding issues
“To shift the thinking from ‘welfare’ to ‘investment’ is part of the strategic challenge”
Heywood (2005)
130
Local contributions to DFG funding
13.1 Local authorities used to contribute around 40% of the capital costs of the DFG,
but these contributions have almost disappeared since central government
funding increased from 2015/16 onwards. Housing authorities have found it
hard to justify putting capital into the DFG when the main benefits are felt by
social care and health, especially when housing authorities have been
particularly badly affected by austerity measures.
13.2 Council-run adaptation services typically have a limited number of funding
options. Almost half (48%) comes from housing, 46% from fees levied as part
of the DFG, 6% from public health and 1% from private fees (Figure 13.1).
Nothing comes from adult social care or the BCF. In comparison, independent
home improvement agencies and those managed by registered providers had
a wider variety of sources including: adult social care, the BCF, local housing
authorities, the CCG, public health, charities and fees (DFG and private).
Figure 13.1 Funding for council-run and outsourced services
130
Heywood, F., et al. (2005) Reviewing the Disabled Facilities Grant programme, Bristol: School for
Policy Studies.
153

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
13.3 Integration of services can bring together other funding streams such as ICES,
wheelchair funding, assistive technology and telecare. Revenue costs can then
be shared between health, social care and housing. We have also seen very
effective council run services, like HEART in Warwickshire, Dorset Accessible
Homes Service and Lightbulb in Leicestershire, that are making a real
difference in their communities through using these pooled funding
arrangements.
13.4 A different solution to the funding issue is for new integrated home
independence services to be arms-length from local authorities. This has been
done in a few areas such as Sunderland
131
. This enables council-run services
to bring in funding from a wider range of sources. Being arms-length from the
council could also make the service feel more welcoming to home owners,
private tenants and private landlords. Evidence is shown in Chapter 16 on
‘Developing a market’ that these groups do not always think of turning to the
council for help with adaptations. If adaptation services were clearly about
investment in housing and independence, rather than welfare, it would give
them a completely different look and feel from current DFG services. This might
be an option to pursue in some areas.
Risk sharing contingency fund
13.5 As was discussed in Chapter 12 in relation to national DFG funding allocations,
from year to year grant spending is not always even. Across county authorities
or regions some districts may have underspend, while others have waiting lists.
Given the difficulties in fine tuning allocations to need, there should
consideration of more collaborative DFG funding arrangements among BCF
partners.
13.6 With a Housing and Health Partnership Board in place, with better strategic
oversight and integrated working, it should be possible to set up a partner-wide
contingency fund. This can cover:
Demand over and above the expected level
Higher than anticipated numbers of completions
More complex and expensive adaptations, such as extensions.
13.7 Up until now, many authorities have been loath to share budgets or pay into
contingency funds because they worry that the money might be absorbed into
general social care funding, especially when social care is under so much
financial pressure. Provided DFG funding remains properly ring-fenced in BCF
budgets, and the BCF and HWB are required to report on DFG funding
separately each year, it should be possible to allay these fears.
131
Mackintosh, S. and Collingbourne, L. (2015) Home Adaptations for Disabled People Good Practice
Case Study: Sunderland, Home Adaptations Consortium.
https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-of-good-practice-sunderland-
care-support.pdf.
154

Disabled Facilities Grant (DFG) and Other Adaptations Main Report
13.8 It is important that contingency funds are set up to ensure that disabled and
older people get access to adaptations when they need them, and do not have
to wait when one area has run out of funding while a neighbouring one has
underspent resources. It would also allow long-term planning for the disabled
person and their family, rather than decisions being budget-driven.
13.9 Holding on to funding may have been justified when local authorities were
putting in their own capital resources, but not when nearly all of it comes from
central government. A more collaborative approach would fit with mandatory
RRO policy as it does not fetter discretion, and still allows each decision to be
made on its own merits.
Joint decision-making and combined funding
13.10 Complex cases, particularly those that are more expensive, need a different
approach to decision-making, as was discussed in Chapter 11 ‘Working Better
Together’. They also need a different approach to funding.
13.11 A housing and health business case should consider the relative costs of
different adaptation options, the alternative costs of care if adaptations are not
provided and the appropriate mix of funding from different budgets (Table 13.1).
Housing providers need to be part of the strategic Health and Housing
Partnership Board to ensure the business case can include options to move to
alternative accommodation (an existing dwelling, or new adapted property).
Table 13.1 Costs of care for adults and children
Provision Type
Annual Cost
Private sector nursing homes for older people
£41,912
Private sector residential care for older people
£32,864
Residential care homes for adults requiring learning disability
support
£69,524
Private sector residential care homes for adults requiring
physical support
£46,488
Care home for children — local authority own-provision
£210,444
Voluntary and private sector care homes for children
£171,496
Foster care for children
£33,592
–
Source: PSSRU Health and Social Care Unit Costs 2017
13.12 This type of good practice in the delivery of larger and more complex
adaptations is already happening in local authority areas where partnership
working and effective RRO policies are already in place.
155
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Personal health budgets
13.13 The Department of Health and Social Care, and NHS England may extend the
right to personal health budgets as part of a plan to think differently about the
links between health, work, housing and disability
132
. Personal health budgets
and personal social care budgets could be joined together into a single budget.
13.14 There is potential for DFG funding to be included to allow people “a single,
holistic plan that meets both health and wellbeing needs”. This could improve
outcomes and quality of life and reduce admission to hospitals and care homes.
As part of this process, there is a programme of work looking at how this might
change specifications for wheelchairs. An example is provided below of how
joint decision-making about wheelchair funding and DFG funding can provide
better solutions.
Personal budgets - a joined up approach
Personalised wheelchair budgets give disabled people more choice over the
specification to allow them to get freedom from pain, better posture and achieve
their own goals for independence
133
. This can be effectively combined with
decisions about adaptations as the following example demonstrates.
A wheelchair user with a small child needed home adaptations - two options:
1. Adapt both the bathroom and kitchen - this would require lowering the
kitchen surfaces which might prove a hazard for the toddler.
2. Only adapt the bathroom and provide a wheelchair with a riser function to
allow the current kitchen to be used without adaptation.
Option 2 was preferred as the customer needed a replacement chair. The
higher specification would also allow greater independence outside the home,
such as being able to go supermarket shopping. Unfortunately, the higher
specification chair was not one that was normally provided by that local
authority, so the case went to a decision-making panel.
The county council suggested using a number of different budgets to provide
the optimal solution. ICES funding could meet the basic wheelchair costs and
flexible DFG funding could meet the costs of the higher specification alongside
the bathroom adaptation costs. However, there was no agreement in place to
allow this to happen quickly. An alternative plan was therefore adopted with
ICES paying the basic wheelchair costs, the County Council providing top up
funding and the DFG covering the adaptation costs.
This shows the type of pragmatic decision-making and flexible use of budgets
that is required to give outcomes that maximise people’s independence.
132
Department of Health and Social Care, and NHS England (April 2018) A consultation on extending
legal rights to have for personal health budgets and integrated personal budgets, p13.
https://consultations.dh.gov.uk/commissioning-integration-and-transformation/extending-rights-to-
personalised-budgets/.
133
https://www.england.nhs.uk/personal-health-budgets/personal-wheelchair-budgets/.
156

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Recommendations – other funding issues
That integrated services seek funding from a wider range of sources.
That risk-share funds are set up to deal with uneven demand for grants and
that very expensive adaptations are jointly funded by housing, health and
social care.
That the DFG is included in personal budgets to provide solutions that meet
people’s own goals.
157

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 14 The means test
14.1 The application of means testing for housing grants was introduced at the same
time as the Disabled Facilities Grant, in the Local Government and Housing Act
1989. The aim of the “test of resources” was to “target grant aid on the most
needy households”
134
.
14.2 The test largely mirrors the system of calculating entitlement to Housing Benefit.
The assumed weekly needs of the household (the “applicable amount”) is
calculated taking into account the number of people, their ages and other
circumstances. This is then compared to actual income, and where income is
greater than the applicable amount, a "loan generation factor" is applied to the
‘excess income’ to arrive at a notional "affordable loan". This is the amount by
which the grant is reduced, or the contribution expected from the applicant. The
reduction in grant caused by this test is lower for tenants because it is assumed
that loans will be available on less favourable terms than owner occupiers. The
underlying calculation assumes that owners will be able to acquire loans
repayable over 10 years, while for tenants the period is assumed to be five
years.
14.3 The formula used for calculating grant entitlement for those with incomes over
their needs level is:
Amount of grant = cost of work – (actual income – applicable amount) x loan
generation factor
14.4 The loan factor makes use of four bands, which ensure that the contribution
assessed for those with low excess incomes is lower, for each pound, while for
those with higher levels of excess income, the contribution is greater.
14.5 The current legislation allows for circumstances where it is assumed that
income does not exceed the applicable amount, and in these cases a test of
resources is not carried out. This includes applications on behalf of a disabled
child and where the disabled person receives one of the “passporting” benefits:
Income Support
Income-based Employment and Support Allowance (not contribution-
based ESA)
Income-based Jobseeker's Allowance (not contribution-based JSA)
Guarantee Pension Credit (not Savings Pension Credit alone)
Housing Benefit
Working Tax Credit and/or Child Tax Credit provided that the annual
income for the purposes of assessing entitlement to the tax credit is less
than £15,050
134
Wilson, W. (1996) Housing renovation grants, House of Commons Library Research Paper 96/34
596/34. https://researchbriefings.parliament.uk/ResearchBriefing/Summary/RP96-34.
158
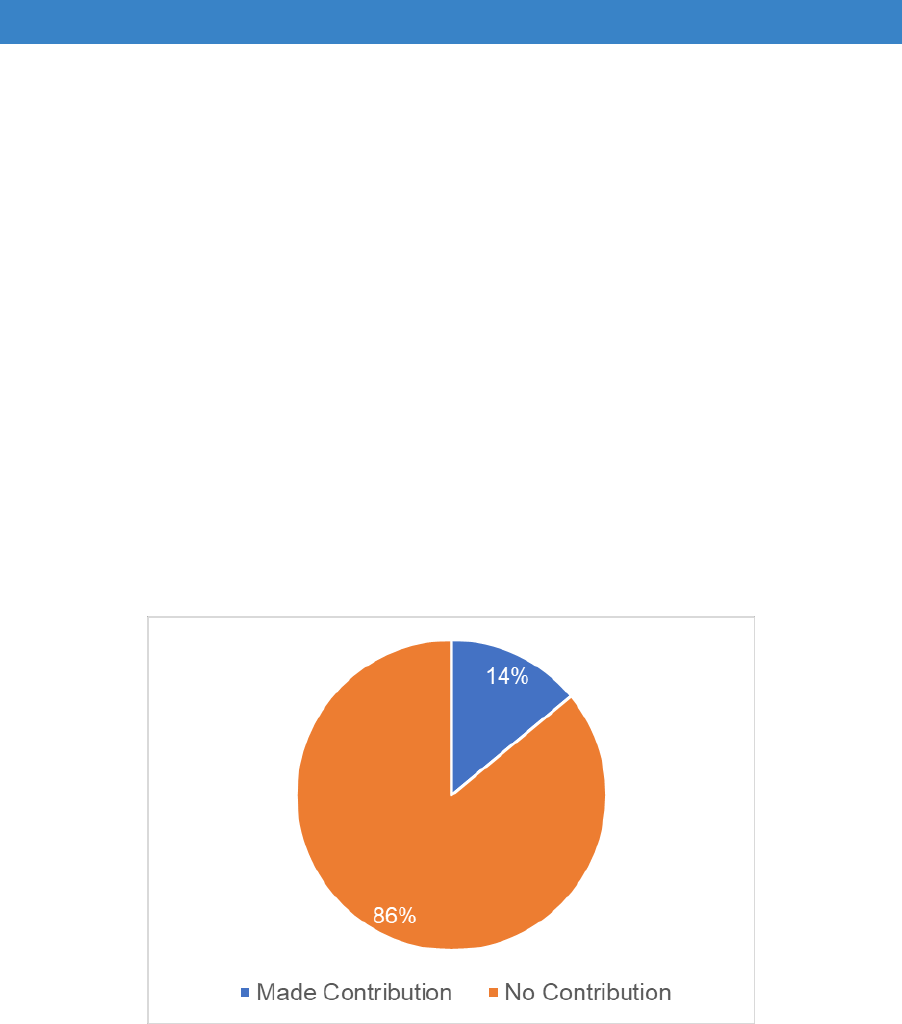
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Universal Credit (this includes any amount of Universal Credit which is
being introduced from 2013 onwards as a replacement for working age
benefits and tax credits).
14.6 Where an applicant is not passported, then the legislation introduces an
alternative “statutory means testing regime” to be used, such as the Care and
Support (Charging and Assessment) Regulations 2014.
Means testing in practice
14.7 From data submitted to Government, we know that in 2016/17 only 14% of
approved grants were reduced due to means testing (Figure 14.1). Those 14%
had their grant reduced by an average of £1,500 – contributing a total of £9.2m
or just over 2% of the overall spend.
Figure 14.1 Means testing in practice
Source: LOGASnet
14.8 From talking to local authorities, we know that typically the means test is not
carried out on 70 to 75% of applications due to passporting benefits or because
the works are for disabled children, which make-up about 7% of grants. Further
FOI data shows that 34% of grant applications do not proceed, and a quarter of
these are due to the result of the means test (Figure 14.2). We do not know
how many people are deterred from enquiring entirely by the prospect of a
means test.
159
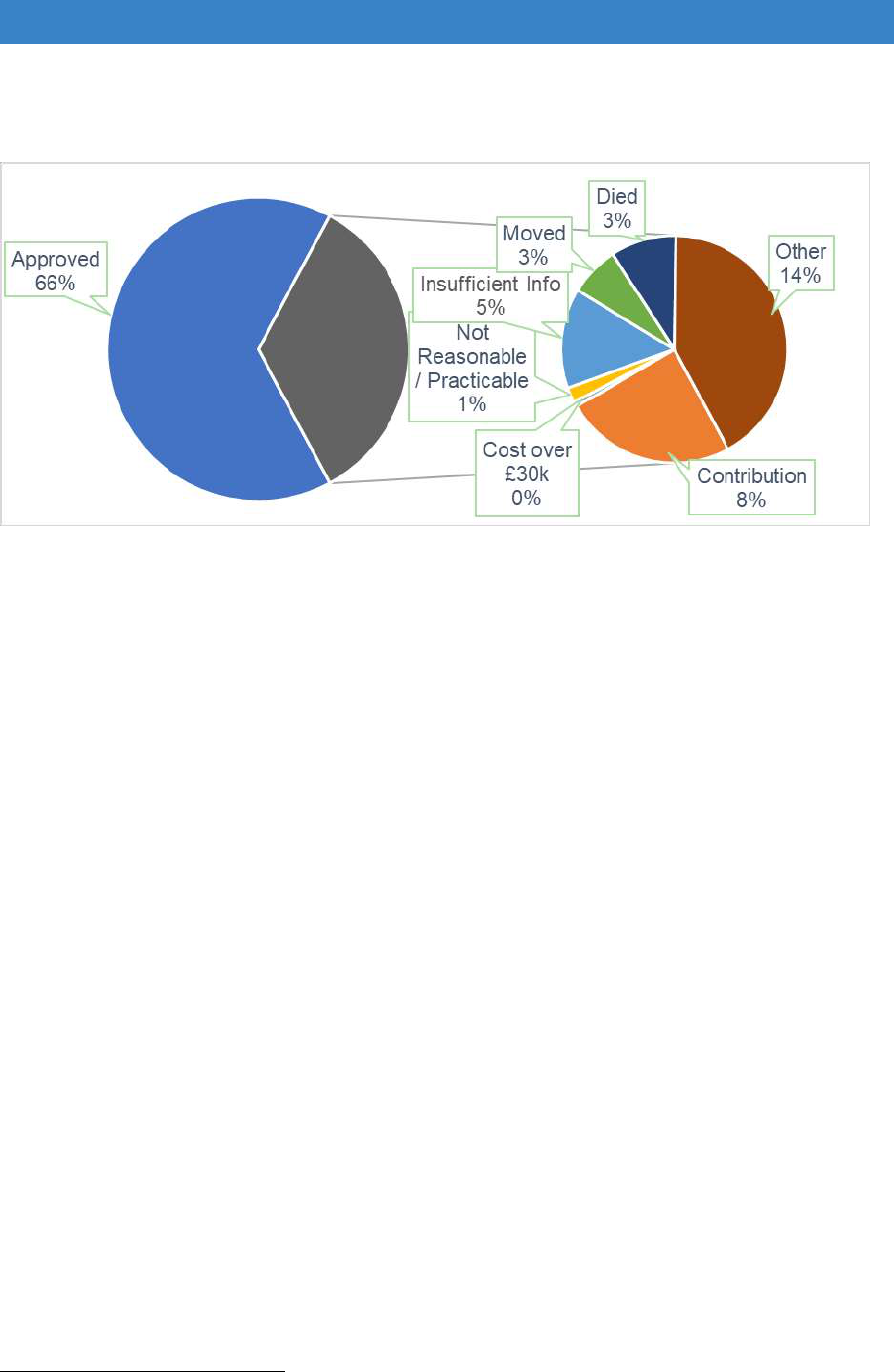
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 14.2 Reason for applications not proceeding
Source: Foundations FOI 2018
The options
14.9 For the purposes of this Review, we have considered 4 options for how the
means test could operate in the future. For each we set out the rationale. Where
we consider it a viable option we estimate the impact in terms of number of
people eligible and the cost to meet that need. The options are:
1. Remove means testing completely
2. Just use passporting
3. Update the existing means test
4. Adopt the Care and Support Charging Regulations
Remove the Means test Completely
14.10 The simplest option would be to do away with means testing entirely. This would
clearly have a large impact on potential eligibility – some 340,000 households
have not already made adaptations due to financial reasons
135
- but it is unclear
how many would actually apply for a Disabled Facilities Grant. At a time of
financial stringency, particularly in social care funding, there are strong
135
Ministry of Housing, Communities and Local Government (2016) English housing survey 2014-
2015: Adaptations and accessibility of homes report, ibid.
160

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
arguments against providing funding to those who would be clearly seen to be
able to afford their own provision.
14.11 Some Local Authorities have experimented with using their discretionary
powers to exempt certain additional groups of people (e.g. registered social
landlord tenants) or works costing less than a specified amount (e.g. £5,000)
from means testing altogether. This usually occurs where a local authority has
sufficient budget to meet additional demand in the short-term but is rarely
sustained in the longer term as demand increases or budgets are re-allocated.
14.12 Several small-scale research projects have shown the investment in
adaptations can provide excellent value for money, but these typically report
savings in social care costs, which is also means tested. Another difficulty is the
current lack of evidence to provide robust estimates of potential cost savings
that may arise from the installation of most different types of home
adaptations
136
. Therefore, we have rejected this proposal except for stairlifts,
where there is a clear return on investment.
Passporting for stairlifts
14.13 Falls are the largest cause of emergency hospital admissions for older people,
and significantly impact on long-term outcomes, e.g. being a major precipitant
of people moving from their own home to long-term nursing or residential
care
137
. Falls that results in injury can be very serious - approximately 1 in 20
older people living in the community experience a fracture or need
hospitalisation after a fall. Falls and fractures in those aged 65 and above
account for over 4 million bed days per year in England alone, at an estimated
cost of £2 billion
138
.
14.14 The location of falls is often unrecorded, but where this information is collected
it shows that the most serious injuries are caused by falls from stairs or steps,
with more than half of deaths recorded in 2015
139
.
14.15 Looking into the return on investment of home adaptations, BRE found that
mitigation of hazards on stairs has the best potential payback period of all –
quoting an overall payback of 0.61 years
140
. Taking into account the cost of a
136
Building Research Establishment (2017) Client Report: Cost benefit analysis of home adaptations
[online] https://www.ageing-better.org.uk/sites/default/files/2017-
12/Appendices%2C%20the%20role%20of%20home%20adaptations%20in%20improving%20later%2
0life.pdf.
137
Department of Health (2012) Improving outcomes and supporting transparency. Part2: Summary
technical specifications of public health indicators.
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_1
32358. Last Accessed 03/04/2015.
138
Royal College of Physicians (2011), NHS services for falls and fractures in older people are
inadequate, finds national clinical audit. https://www.rcplondon.ac.uk/news/nhs-services-falls-and-
fractures-older-people-are-inadequate-finds-national-clinical-audit. Last Accessed 03/04/2015.
139
https://www.rospa.com/rospaweb/docs/advice-services/home-safety/falls-prevention-factsheet.pdf.
140
Building Research Establishment (2017) ibid.
161

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
stairlift (rather than lower cost handrails), the payback period would still be
under two years.
14.16 Traditionally, the purchase of new stairlifts has been funded using the DFG,
with ongoing servicing and maintenance provided by Social Care. This split in
responsibility has often meant that the whole life cost of a stairlift has not been
fully considered under any procurement process and also limited the potential
for refurbishment and recycling of existing stairlifts.
14.17 We recommend that the cost benefit of stairlifts is such that a grant should be
awarded without being subject to means testing (subject to an application
meeting the tests of Necessary, Practicable, Appropriate and Reasonable). We
further recommend that this only applies where a Local Authority has
established a stairlift refurbishment and recycling scheme as discussed later in
Chapter 16.
14.18 Where an applicant wants to guarantee a brand new stairlift, this would fall
outside of the eligibility for a DFG.
Passporting for palliative cases
14.19 A small number of local authorities have used the RRO powers to introduce a
non-means tested grant for palliative cases. The business case is fairly
straightforward: where adaptations can be installed that will enable a person to
remain at home for longer at end of life; it can save £280 per day compared to
specialist hospital care
141
. In just one month these savings are equivalent to the
average cost of a DFG. However, another study noted that further work is
needed to gain a more complete understanding of the costs of palliative care
142
.
14.20 We recommend that further consideration is given to grant for palliative cases
being awarded without being subject to means testing.
Use of Passporting Only
14.21 As previously described, the majority of DFG applications are already
passported due to receipt of certain benefits or the adaptations benefiting a
child. We are also recommending that applications for stairlifts, and possibly for
palliative care, should also be passported in the future.
141
Marie Curie Cancer Care (2014) Understanding the cost of end of life care in different settings.
https://www.mariecurie.org.uk/globalassets/media/documents/commissioning-our-
services/publications/understanding-cost-end-life-care-different-settingspdf.
142
Gardiner C, Ryan T and Gott M. (2018) What is the cost of palliative care in the UK? A systematic
review BMJ Supportive and Palliative Care, http://dx.doi.org/10.1136/bmjspcare-2018-001519.
162

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
14.22 However, this would mean that many people with low earned incomes or small
private pensions would be unfairly disadvantaged, and so we have rejected
using passporting only.
Update the Existing Means test
14.23 Aspects of the existing means test have been criticised since it was introduced
in 1989. The Government carried out a review of the operation of the new grant
system in 1991/92, where local authority associations described it as
“bureaucratic, difficult to understand and costly to administer”
143
.
14.24 The review in 2005 stated that “The Test of Resources, in limiting who is eligible
for help, excludes some people in great need, especially … adults of working
age. For these people, it bears no relation to real outgoings and severely
discourages those who work by requiring a level of contribution that for many
represents an unsustainable burden.”
14.25 Research carried out by BRE in 2011 listed the key criticisms, including:
The use of a standard housing allowance for all households disadvantages
those with higher housing costs; particularly those with mortgages.
The taper system used by the Loan Generation Factor acts as a disincentive
to take on paid work or additional hours or move to a better paid job.
‘Allowable’ income should be set rather higher than just the basic amounts
of income support and pension credit allowances.
It is very different to means testing for other services (e.g. care) which
causes confusion amongst applicants and agencies.
14.26 Our online survey echoed these concerns, particularly cases of families where
having enough income to sustain a relatively modest mortgage is too much to
make them eligible for a grant.
14.27 A more recent criticism is that none of the amounts used to calculate the
applicable amount have been updated since May 2008, whereas actual prices
have increased by nearly 30% due to inflation. The consequence is that more
people will have a weekly income higher than their applicable amount and
receive a lower or nil grant. Figure 14.3 below shows the percentage of grant
applicants who received a full grant in one Local Authority falling by around 15%
over the last decade.
143
Wilson, W. (1996) ibid.
163
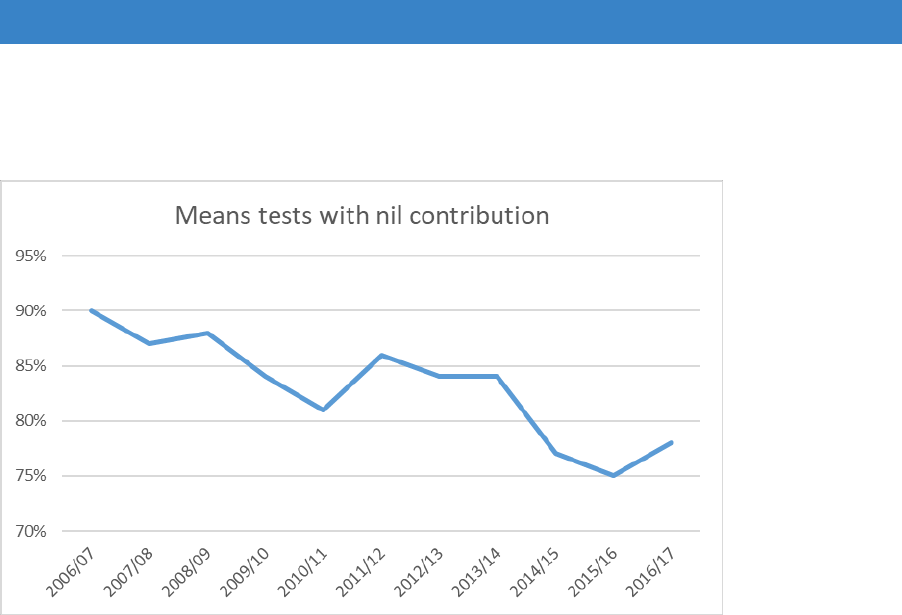
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 14.3 Applicants receiving full grant
Source: Information from one local authority
14.28 The passporting arrangements in the current regulations are also out of date,
not taking into account the fundamental changes introduced in the wider
benefits system over the last few years including Universal Credit.
14.29 We have looked at the options for updating the current means test by
considering four aspects: assessing need, assessing resources, assessing
entitlement and passporting.
Assessing need
14.30 The assessment of needs and resources is based on that of the Housing Benefit
(HB) scheme, but the rates used in the assessment of need have not been
increased in line with the uprating of HB.
14.31 Originally the contribution to cost of works represented the value of a notional
loan with weekly payments which was calculated by subtracting ‘allowable
income’ (the amount a household needs to live on) from actual income along
with a tariff for savings. In the case of owners, the loan period was assumed to
be ten years, in the case of tenants five years.
14.32 Prior to the 1996 changes, the main criticism of this method was that low
amounts of excess income produced disproportionately high contributions. This
placed people on low incomes or those with a limited ability to raise the required
amount of contribution at a disadvantage.
164
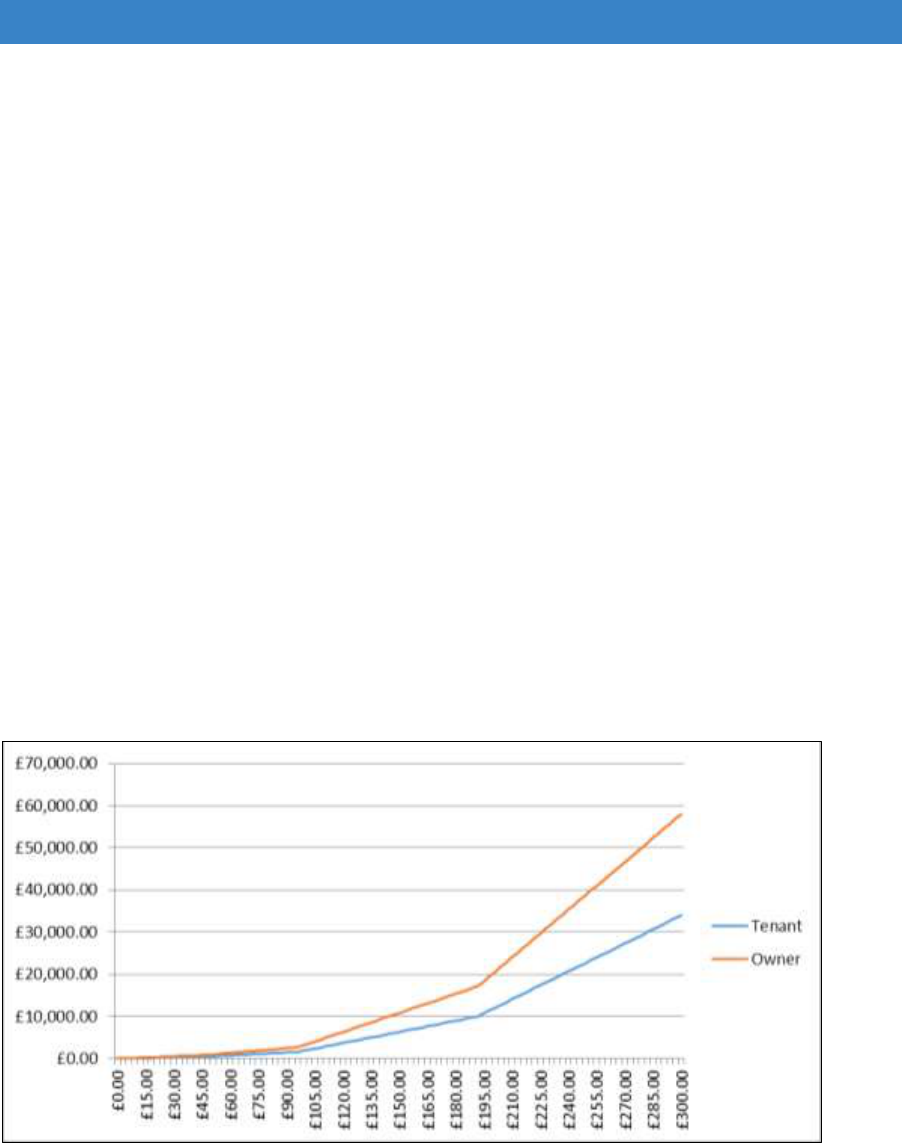
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
14.33 In 1996, the method of calculation was changed. It still relied on the notional
loan principle, but the rates of contribution varied depending on excess income.
The “changeover points” were set at £2,500, £5,000, and £10,000 per year of
excess income.
14.34 Contributions are initially set fairly low, they increase between £47.95 per week
(£2,500 p.a.) and £95.90 (£5,000 p.a.) and sharply between £95.90 per week
and £191.80, and again above this amount. The total contribution is made up
by adding together individual contributions for each band (where necessary).
14.35 We have understood that the reason for treating tenants differently from owners
is that tenants would have to seek an unsecured loan to pay for the works
themselves, whilst owners could increase their mortgage and therefore borrow
more cheaply. Those who live in caravans or houseboats, pay at the lower,
tenant’s multiplier because it is considered difficult to get a mortgage on a
caravan or a houseboat.
14.36 The chart below (Figure 14.4) demonstrates the contribution levels under the
current means test for excess income, from £0 to £300 a week.
Figure 14.4 Increasing owner and tenant’s contribution under current bands
14.37 It can be seen that relatively modest levels of excess income can reach the
current maximum grant level, at least for owners.
14.38 The freezing of the needs rates has had the effect of increasing the amount of
excess income in individual cases. As the levels of income taken into account
have increased over time, it is more difficult (because of the method by which
the notional loan is calculated) to determine what effect continuing indexation
would have had on grant levels.
165

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
14.39 The means test is applied to the disabled person and partner. There are
different rates for those above pension credit age and, unlike most current
means tested benefits, an additional pensioner premium for those aged over
60. There is a standard housing allowance of £61.30 which is added to the
personal allowances and premiums. Capital rules, for assessing notional
income, match those of HB, themselves unchanged for many years.
Re-establishing the link with HB rates
14.40 Table A3.1 in Appendix 3 shows the current rates of allowances and premiums
used in the grant scheme and those used for HB.
14.41 In addition to the allowances and premiums, the assessment of needs also
includes a fixed housing costs amount, currently £61.30. This is recognised as
failing to take account of differing housing costs across local areas and sizes of
property.
14.42 Examples 1 to 5, below, and in Appendix 3, show the effect of uprating, in a
variety of scenarios, to the current housing benefit rates, including an inflation
linked increase to the housing element, bringing it to £79.25.
14.43 We considered ways in which real housing costs could be included as part of
the needs assessment. Actual housing costs would be both difficult to
determine and would not, in themselves, reflect genuine housing costs on a
‘greenfield ‘basis. Differences between rented and owned properties, those with
and without mortgages, those with ground rents or service charges, and other
factors make this impractical.
14.44 It would be possible however, and relatively simple, to make use of the Local
Housing Allowance (LHA) rates as a comparison factor between different areas
and housing sizes. LHAs were calculated using the lowest third of private local
market rents for properties with different numbers of bedrooms, although they
are now CPI linked. The values are used as part of the HB assessment, so the
appropriate tier of local authorities is very used to working with them, and they
are simple to find for individual properties using the LHA-Direct website.
14.45 The overall average LHA figure for England (excluding the single room rate) in
April 2018 was £159.45. The figures for different room sizes are shown in this
table. There is a cap on the LHA figures which affects, in particular, inner
London. The figures take no account of the number of properties in each band
or in each area.
166
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 14.1 Using Local Housing Allowance (LHA) rates
LHA April 2018
Property size
1 Bed
2 Bed
3 Bed
4 Bed
Average LHAs England
£113.31
£140.77
£166.69
£217.05
Maximum
£268.46
£311.40
£365.09
£429.53
Minimum
£69.73
£85.00
£97.81
£123.58
14.46 If an LHA linked factor, for example 50%, of the LHA for the size of property
and the area (determined by a postcode lookup on the LHA-direct website) then
some rough account of a housing cost link for each area could be incorporated
into the assessment.
14.47 This would provide a crude average of £79.73, but with a potential range from
£39.87, for the smallest property in the least expensive area to £214.77 for the
largest property in the most expensive area.
Assessing resources
14.48 Resources rules have been largely unchanged for many years for HB.
Consequently, the current DFG scheme differs little from the assessments that
would apply under HB. Capital limits and tariff income figures are identical, as
are earnings disregards. There is a small difference in the rules applying to
income from sub- tenants.
14.49 As excess income is determined solely by the test of whether resources are
greater than needs, the effect of uprating the current means test to use the HB
figures will reduce the amount which can be assessed as contributing to the
cost of works. As each assessment depends upon the circumstances of the
individual and their household, it is not possible to make any accurate estimate
of the amounts involved.
14.50 Unlike most means tested benefits, there is no capital cut-off in the current grant
scheme. Currently Guarantee Pension Credit also has no capital cut-off. There
is an argument that adaptations could be paid for from any substantial capital
resource, but careful drafting would be needed to ensure that, for example,
personal injury awards and monies required for future care were treated
appropriately.
Assessing entitlement
14.51 The four-band calculation of a notional loan value, although complex, seems to
be widely accepted as a pragmatic solution. The previous criticism of over-
167
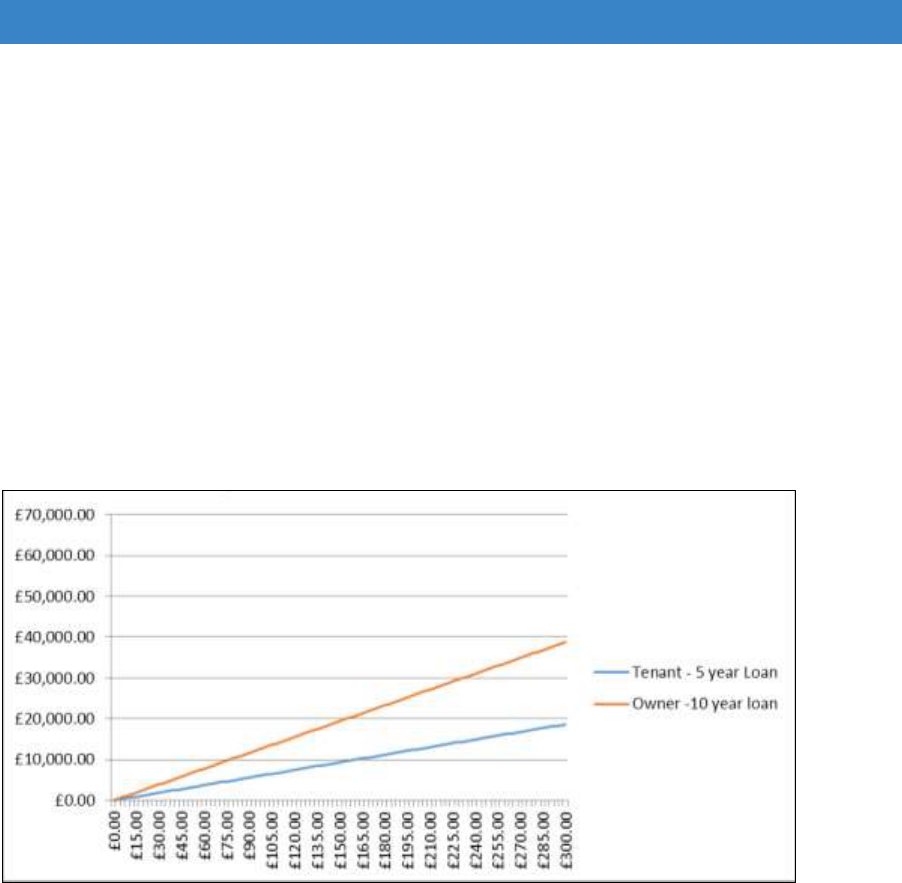
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
contribution by those with small amounts of excess income and the smaller
contribution of those better-off seem to have been satisfied.
14.52 Other interest linked assessments, such as the new Loan for Mortgage Interest
scheme in means tested benefits, and the notional pension’s income
assessment in the same benefits, make use of the Gilt rate on government
bonds. We modelled a fixed Gilt linked contribution system as shown in the
chart below (Figure 14.5). The gilt rate used is that of 4
th
May 2018 – 1.67% –
rounded down, as in other existing uses, to the nearest .25%.
Figure 14.5 Increasing owner and tenant’s contribution using gilt linked loan value of
1.5%
14.53 It can be seen that a linear Gilt linked system could face the same criticisms of
the system that existed pre-banding. People with small amounts of excess
income would face higher contributions, while there would be reductions in
contribution for those with higher incomes.
14.54 Gilt linking in means tested benefits has the advantage of automatically
amending relevant amounts as rates change. This removes any need for
frequent amendments of regulations and provides a greater level of
administrative simplicity. While a banded Gilt linked assessment would not be
difficult to introduce or operate, it is unclear whether there is enough need to
reflect day-to-day changes in rates.
Passporting
14.55 Passporting plays an important role in the administration of the current scheme.
Passporting is widely used across many assessment schemes in means tested
168

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
benefits and other social welfare areas. It permits trusted assessments of need
for one scheme to be used in other domains.
14.56 The current DFG scheme passports recipients of most means tested benefits
to a full grant. A very high proportion of grants are passported, about two thirds,
in the current scheme.
14.57 Changes in means tested benefits, following the introduction of Universal Credit
(UC) would suggest that some changes should now be considered. The rate of
introduction of UC and the fact that the bulk of initial claimants have been
healthy young single people has meant that an interim decision to passport by
any receipt of UC has caused few problems.
14.58 As UC rolls out further however, we suggest that it is now appropriate to
consider its use in passporting in more detail. UC can be paid to people
regardless of their hours of work or health condition. This means that it may be
paid to households with relatively high levels of income. Working Tax Credit,
the legacy benefit for those in full-time work, and Child Tax Credit passports
only where they are awarded on an income of £15,050 or less. UC might seem
to be amenable to a similar approach. It should be noted that the Government
has chosen to passport UC recipients to an entitlement to free school meals,
only where earnings are £7,400 or less. However, UC can vary on a monthly
basis which needs to be taken into account.
14.59 Another area where passporting might be extended is where domiciliary care is
being provided. Only 16% of grant cases are also in receipt of domiciliary care,
and passporting could help reduce any instances of the same excess income
being used for two assessments.
14.60 Receipt of Council Tax Reduction as another passport, as in Wales, may seem
to be a logical extension. In England, however, the benefit (or more precisely
the charge reduction) has been devolved to local authorities and is increasingly
divergent from the original model within different authorities. The maximum
reduction varies from 50% to 100% of the Council Tax charge, there are very
different treatments of capital and substantially different rule sets which could
lead to a postcode lottery.
14.61 There are some advantages to maintaining the existing means test structure,
one of which is familiarity. It has established eligibility for a DFG for nearly 30
years, and despite its complexity is widely understood by Local Authorities, if
not by the public. Any change would necessitate system changes and training
needs for staff and create winners and losers in those being assessed.
14.62 The link to HB rules, where there will be a great deal of experience in the
administering department in the same tier of local government, can help
minimise issues of error and fraud.
169

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
14.63 Disregarding disability benefits as income allows them to continue to be used
for their intended purpose while recognising, from their receipt, the increased
need likely to be caused by the claimant’s disabilities.
Adopt the Care and Support Charging Regulations (CSCR)
14.64 The Care and Support (Charging and Assessment of Resources) Regulations
2014 were introduced as part of the Care Act 2014; largely mirroring the Fairer
Charging regime they replaced. As set out in the statutory guidance
144
, the
principles are that the approach to charging for care and support needs should:
Ensure that people are not charged more than it is reasonably practicable
for them to pay
Be comprehensive, to reduce variation in the way people are assessed and
charged
Be clear and transparent, so people know what they will be charged
Promote wellbeing, social inclusion, and support the vision of
personalisation, independence, choice and control
Support carers to look after their own health and wellbeing and to care
effectively and safely
Be person-focussed, reflecting the variety of care and caring journeys and
the variety of options available to meet their needs
Apply the charging rules equally, so those with similar needs or services are
treated the same and minimise anomalies between different care settings
Encourage and enable those who wish to stay in or take up employment,
education or training or plan for the future costs of meeting their needs to
do so
Be sustainable for local authorities in the long-term
14.65 These principles could equally apply to “charging” for adaptations, and there
are several advantages to aligning the two systems. The CSCR is the
mechanism used to assess the level of financial support someone receives
towards care provided in their own home. Many DFG applicants do not currently
receive care and the adaptations provided should delay the need for this in
many cases. The current differences in charging arrangements are difficult to
understand. Adopting a similar means test for the DFG would make it simpler
for social care staff to understand possible entitlement to a grant. However, the
means test would still have to be applied for each application.
14.66 The 2005 Review of Disabled Facilities Grants recognised that the Fairer
Charging model addressed two of the key criticisms of the existing test for DFG
by (a) disregarding earned income entirely; and (b) incorporating actual housing
costs instead of notional costs. The same would apply under the Care and
Support Charging Regulations (CSCR) today.
144
Statutory guidance, Care Act 2014: supporting implementation [online].
https://www.gov.uk/government/publications/care-act-statutory-guidance.
170

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
14.67 Other key differences between CSCR and the current system are:
• Only the income of the disabled person is taken into consideration, not any
belonging to their partner/spouse.
• Allowances are set to income support / pension credit plus a buffer of 25 per
cent rather than at the base levels. This buffer level is still in place in the
current scheme figures, but it is no longer statutory. This ensures that
recipients are left with an individual income above benefit levels.
• Anyone with capital above an upper limit, currently £23,250, does not
receive any assistance until/unless the value of their means tested assets
subsequently drops below that level through, for example, paying towards
their care.
• There is no passporting of entitlement.
14.68 CSCR also makes it clear that certain benefits are intended to help pay for care
(Attendance Allowance, Disability Living Allowance - Care, Constant
Attendance Allowance, Exceptionally Severe Disablement Allowance and a
Severe Disability Premium with Income Support) and therefore should be
counted as income.
14.69 In their response to this review, ADASS noted: “Given that the link is being more
directly made for the DFG to support adult social care achieve the outcomes
expected through the Care Act, evidenced by it being channelled through the
Better Care Fund (BCF) then aligning a means test to the Care Act would be a
sensible approach.”
14.70 The impacts of changing to a CSCR based test were fully explored by the BRE
in their 2011 paper. In summary they found that:
The use of actual housing costs would mean a slight reduction in the number
of people eligible for DFG as it impacts negatively on those, mostly older
households, who own their home outright. However, it would mean more
help to those of working age and in work who are paying at least some of
their own rent/mortgage.
The 25% buffer above income support/pension credit levels would increase
the number of people eligible for DFG by around 7.5%. The majority (82%)
of the ‘winners’ were aged over 60.
Incentivising Personal Responsibility and Preventative Adaptations
14.71 There is a growing body of evidence and recognition that reducing hazards in
the home will lead to fewer accidents and associated injuries and ill health.
However, it is often the case that a person only becomes eligible for a DFG
after an injury, at the point when they are permanently and substantially
disabled.
14.72 Government has said that it wants to improve the risk pooling offer for
individuals and signalled that the Social Care Green Paper will include an
171
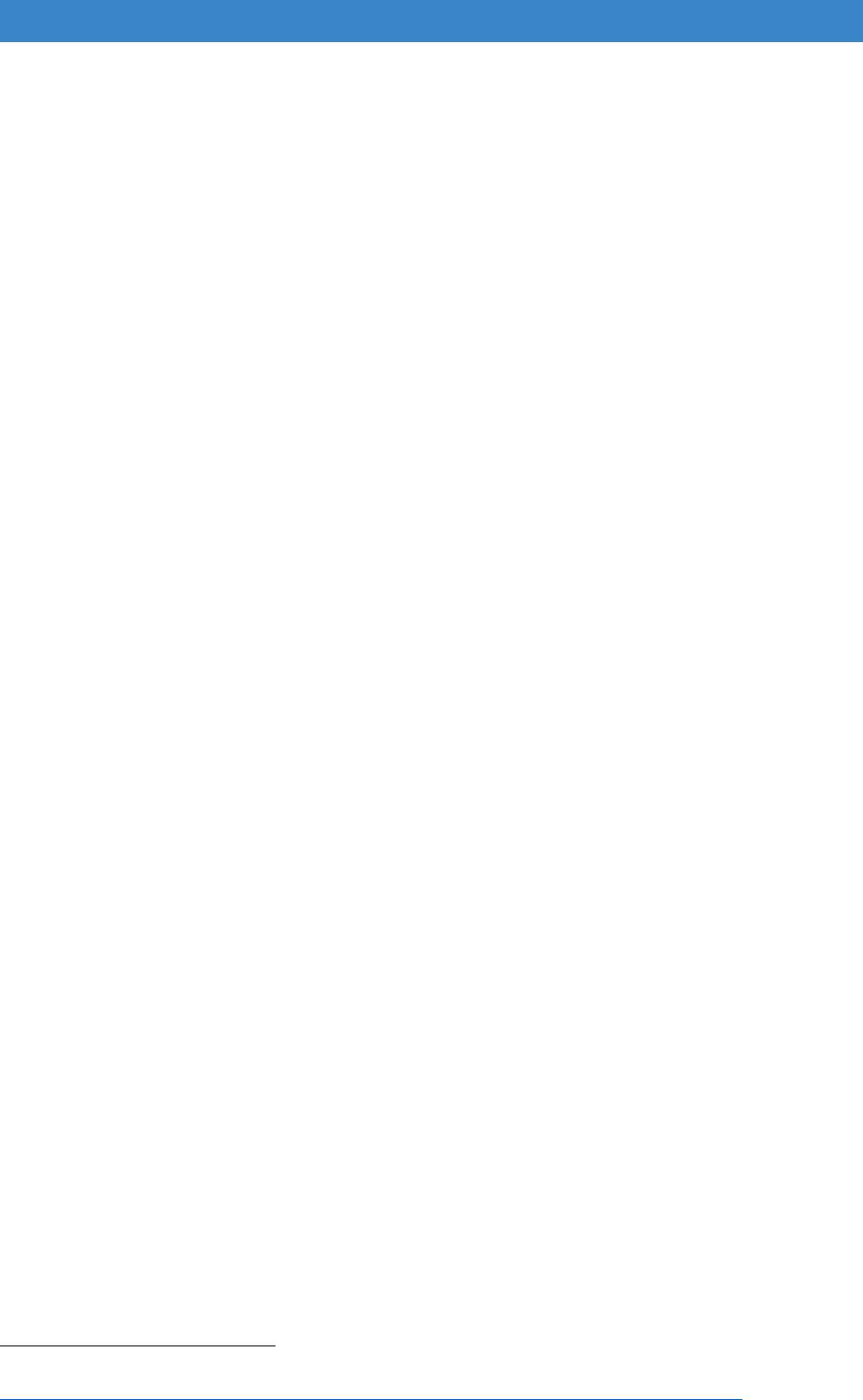
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
absolute limit on the care costs individuals face. If a cap on lifetime care costs
is brought forward to meet this commitment, this would offer one opportunity to
align the means testing regimes for DFG and social care, while also
incentivising individuals to make adaptations.
14.73 The inclusion of adaptations within the cap would deliver several key benefits:
• Raise public awareness of the benefits of preparing their home for old age
when considering home improvements
• Encourage people to carry out appropriate adaptations to enhance their
independence instead of paying for domiciliary care – limiting their overall
spend and reducing the likelihood of ever reaching the capped level
• Reduced numbers of people reaching the care cap will limit the cost of social
care services to the state
• Adapted homes will present fewer hazards leading to less injuries and calls
upon the NHS.
14.74 A light touch assessment process would be required to ensure that any
adaptation was appropriate and reasonable, but we recommend that this
proposal is given consideration within the forthcoming Social Care Green Paper
on the care of older people expected to be published in the autumn of 2018.
Further Considerations
14.75 CSCR is usually used to calculate a weekly contribution towards ongoing care
costs. A mechanism similar to the existing DFG Loan Generation Factor would
be required to convert this weekly amount into a one-off contribution towards
the cost of an adaptation. The scenarios in Appendix 3 show that levels of
excess income under the two tests would be substantially different. We suggest
that further modelling is necessary to devise a contribution formula that takes
account of this and of the other uses for the assessed excess income.
14.76 The need for care and adaptations are unlikely to start at exactly the same time.
FOI data shows that only 16% of DFG applicants are already receiving social
care funded domiciliary care at the time of their application
145
.
14.77 Where someone has been means tested for a DFG and made a contribution,
we recommend that the contribution is taken into account by social care in any
future means testing. Looking at existing local CSCR policies the simplest
approach would be to assume the benefit of the adaptation lasts for 500 weeks
and divide the contribution by 500 to turn into a weekly amount.
14.78 We also recommend that the current passporting arrangements that exist for
means tested benefits (revised as suggested previously) as well as disabled
145
Foundations (2016a) Linking Disabled Facilities Grants to Social Care Data.
http://foundationsweb.s3.amazonaws.com/4210/foundations-dfg-foi-report-nov-2015.pdf.
172

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
children are incorporated for DFG purposes to minimise the impact of adopting
CSCR in terms of administration costs and potential delays.
14.79 During the workshops, a number of delegates raised the issue of assessing
Disability Related Expenditure under CSCR for DFG purposes. This aspect of
the test can require detailed information about spend on personal items that
would not always be appropriate to discuss as part of a housing grant
application. This aspect of the test is also open to local discretion, which
introduces significant variation across the Country. We recommend that a
standard minimum amount is used for assessments under DFG. For example,
the Leicestershire CSCR policy
146
allows:
A standard minimum allowance for 2017/18 for a single person of £20 per
week.
A standard minimum allowance for 2017/18 for a member of a couple of £15
per week.
A standard minimum allowance for 2017/18 for a couple of £30 per week.
14.80 It has been suggested that existing CSCR capital limits may be increased in the
future, which would mitigate the differences with the existing DFG means test.
However, this should be taken into consideration in any revised CSCR test.
Example scenarios
14.81 These are included to demonstrate the differences between the current and
uprated schemes and the quite different calculation used in the social care
domiciliary support means test. In the DFG means test, there is only a
contribution towards the cost of works where the assessment finds an excess
of income over needs. The detailed figures, and analyses and notes underlying
the charts are in Appendix 3.
146
Leicester City Council (2017) Adult Social Care Charging Policy [online]
https://www.leicester.gov.uk/media/179202/charging-policy-2017.pdf.
173

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 1
Single, aged 55, disabled, receiving high rate DLA or PIP for care needs. No
income other than state benefits
Under the DFG, this applicant is passported to the maximum grant because
they are entitled to a relevant means tested benefit. CSCR takes into account
the means tested benefits and the disability benefits as income, generating an
excess income used to assess a contribution (unless passporting is also
applied for means tested benefits - as recommended for DFG applications)
Scenario 2
Couple eldest aged 55, one disabled, receiving high rate DLA or PIP for care
needs. No income other than state benefits.
Under the DFG scheme this applicant is passported by receipt of a relevant
benefit, while CSCR takes that benefit and disability benefits into account as
income (unless passporting is maintained for relevant benefits- as
recommended for DFG applications). The social care means test is applied only
to the individual client. In the case of couples, the personal allowance in the
assessment is reduced. Joint income, including means tested benefits, is
similarly proportioned.
174
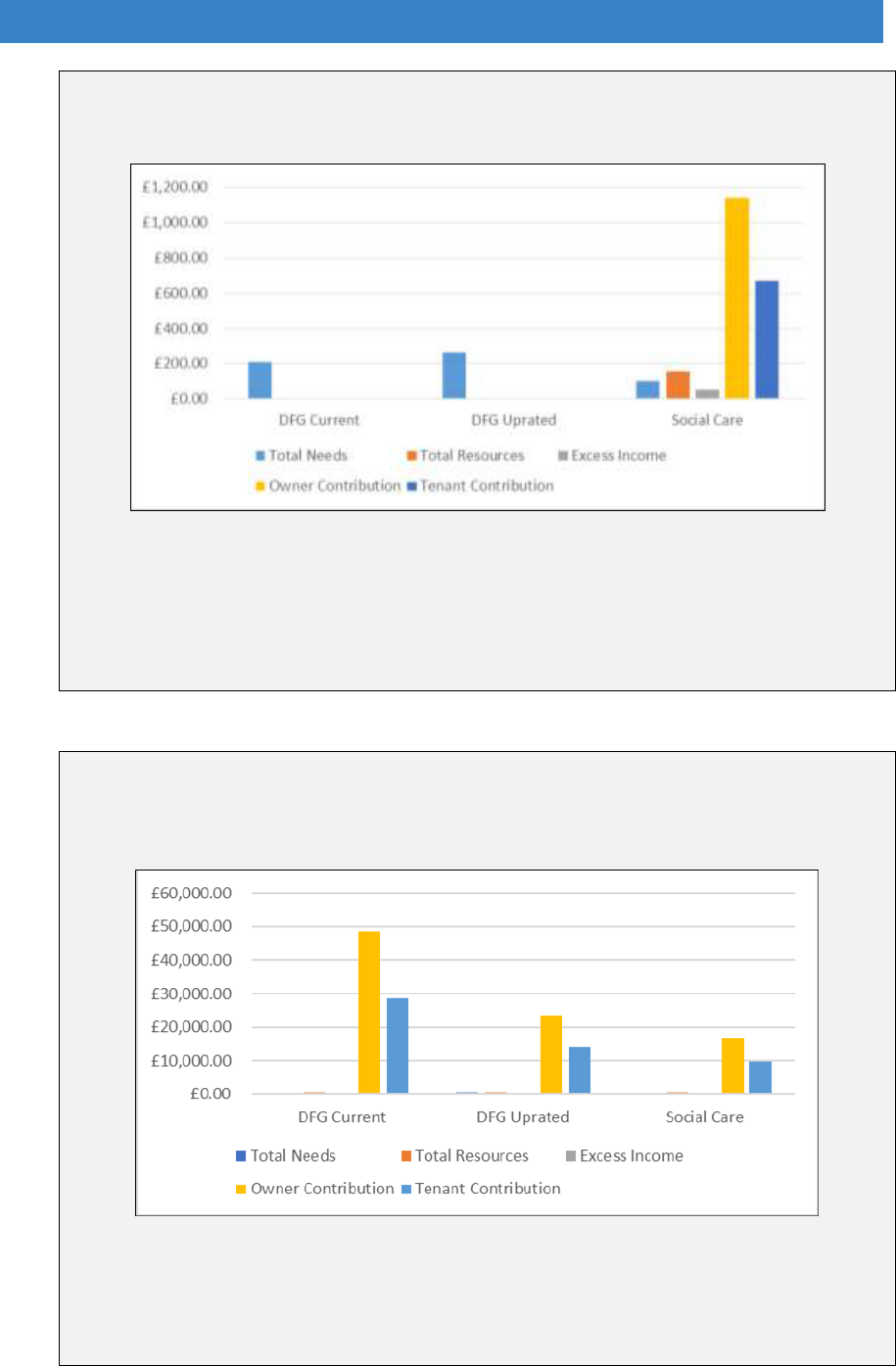
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 3
Single, aged 75, disabled, receiving high rate DLA or PIP for care needs. Full
Basic State Pension of £125.95 a week plus £200 net private pension a week.
Even though an excess income figure has been calculated in the existing and
uprated DFG assessments, they would still be passported by a small amount
of housing benefit which has been calculated. CSCR produces a substantially
larger amount of excess income, and thus a bigger contribution, than the other
assessments (unless passporting is applied for means tested benefits - as
recommended for DFG applications).
Scenario 4
Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week.
The increase in income, coupled with the loss of premiums that would be
applicable to a single claimant, has removed entitlement to means tested
benefits and therefore to passporting. In this scenario, contributions are higher
under the DFG scheme as the social care assessment only takes half of the
real income into account for the individual.
175
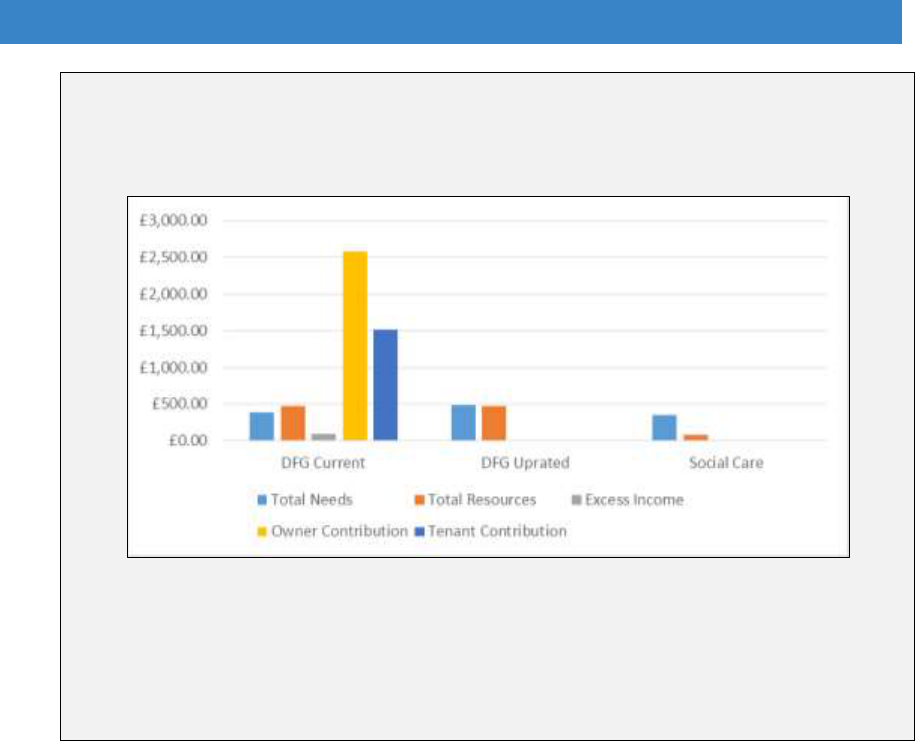
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 5
Couple both aged 55, three children aged under 16, one partner disabled,
receiving high rate DLA or PIP for care needs, other partner working full-time
and earning £400 net a week.
In this scenario, there is no passported entitlement as, although Child Tax
Credit is payable, the earnings figure is above the £15,050 annual threshold.
Child Tax Credit and Child Benefit are disregarded for social care charging.
The complete disregard of earnings and the limiting of assessment to the client
alone, in the social care assessment, produces a much lower resources figure
in this scenario than for the other examples.
Detailed examples showing the effects of capital are also included in Appendix 3.
Choosing a preferred option
14.82 The final decision between: 1) updating the existing DFG means test; and 2)
adopting a modified version of the Care and Support Charging Regulations, will
largely depend on how charging for social care is framed within the forthcoming
Green Paper on social care for older people. Any significant changes in
approach could affect the assumptions on which the options have been based.
14.83 Where an applicant has already been means tested under CSCR and is
contributing towards that care, we recommend that they are passported for the
purposes of an application for DFG.
14.84 The main differences between the two preferred options are summarised in
Table A3.2 in Appendix 3.
176

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Recommendations – the means test
That including assessment for DFG within Care and Support Charging
Regulations is part of the Social Care Green Paper – including passporting
arrangements and a standard minimum amount for Disability Related Expenditure
– and the DFG Regulations are amended accordingly.
That alternatively the existing regulations are updated – re-establishing the link
to HB rates, using LHA rates for the Housing Allowance and updating the
passporting benefits lists.
That stairlifts are removed from means testing where an authority has set up
an effective stairlift refurbishment and recycling scheme.
That further work looks at removing the means test for palliative care.
177
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 15. Regulation and the upper limit
The legislation
15.1 The primary legislation for the DFG is set out in the Housing Grants,
Construction and Regeneration Act 1996, supported by a number of pieces of
secondary legislation in the form of regulations, orders and general consents.
As revised, the legislation is relatively short and sets out the 20 main
requirements:
The Grant
1. Grants are available from local housing authorities.
2. The grant is means tested as set out in regulations
3. There is a maximum amount that can be awarded – this is currently set at
£30,000 as set out in regulations.
The works
4. There are a number of purposes for which a grant ‘must be approved’:
Getting in and out of the property
Making the property safe(r) for everyone living there
Access to the living room
Access to a bedroom
Access to a toilet
Access to a bath or shower
Access to a wash basin
Preparing and cooking food
Improving or providing heating if needed by the disabled person
Controlling power, lights and heating
Access around the property to care for someone else
Making an application
5. An applicant must be over 18
6. An applicant must already be the owner or tenant of the property, or intend to be
(the grant can’t be approved until they are)
7. There must be a disabled person living in the property
8. Disabilities include substantial impairments in sight, hearing or speech, any
‘mental disorder or impairment’ and any substantial physical disability whether
from birth or through illness or injury.
9. The applicant must sign a certificate to say the disabled person intends to live
there for 5 years or more
10.An application must be in writing and include the address of the property, the
proposed adaptations, 2 estimates of cost and details of any other fees or
charges as set out in regulations.
178
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Determining an application
11.The local authority must assess whether the works are ‘necessary and
appropriate’ to meet the needs of the disabled person, and then if those works
are ‘reasonable and practicable’ given the age and condition of the property, e.g.
if the property is in a fit state.
12.For district councils, they must ask for the county council’s opinion on whether
the works are ‘necessary and appropriate’.
13.The grant can’t be approved if the works have already started – unless there is a
good reason why. A grant cannot be approved if the works have already been
completed.
14.The council shall approve or refuse an application as soon as they can, but no
longer than 6 months after the application was made. For approvals, the council
has to say what adaptations it is funding and how much they cost including and
fees or charges. These can be revised if circumstances change. For refusals, the
council has to say why.
Making payments
15.The council can defer payment by up to 12 months.
16.The works must be carried out within 12 months of the approval date (unless
payment has been deferred) – but this can be extended with the council’s
agreement.
17.The grant can either be paid in instalments as the works progress or in full on
completion.
18.The council will only make a payment if they’re satisfied with the works and
receive an acceptable invoice – that isn’t from a member of applicant’s family.
19.The works should be done by a contractor who provided one of the estimates for
the application – unless the council agrees otherwise.
20.If the grant applicant agrees, the council can pay the contractor directly. If the
applicant isn’t satisfied with the works, and the council agrees, the council can
pay the applicant instead.
15.2 The Secretary of State can also impose other conditions. For example, there is
a general consent which allows councils to set a condition that allows them to
reclaim specialised equipment like stairlifts if they are no longer needed.
15.3 Another consent from 2008 says that if the applicant is an owner, the council
can place a local land charge against the grant – for the portion of the grant that
is over £5,000. The charge can be for up to £10,000 and applies if the owner
wants to sell the property within 10 years. In that case, the council has to
consider if the owner is moving because of their work, wellbeing or caring
responsibilities and whether it would cause financial hardship.
179
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
The upper limit
15.4 The maximum DFG is currently £30,000, but some adaptations cost more than
the upper limit, usually the more complex cases, and particularly cases for
disabled children and young people. These often involve the building of
extensions and/or major reorganisation of the internal layout of the home.
15.5 Councils can use discretion to pay extra costs, but the evidence shows that
most try to work within the existing limit. When adaptations are budget-driven,
they may not provide a person-centre approach that caters effectively for future
needs. The Local Government Ombudsman has highlighted cases where this
has not resulted in the best decision for the disabled applicant or their family
147
.
In London, costs appear to be much higher than the limit, at an average of
£55,000, reflecting higher building costs.
15.6 The Royal College of Occupational Therapists in their guidance for the 2014
Care Act said that they would like to encourage authorities to look imaginatively
at their discretionary funding and top-up options, including the options available
in the use of the Better Care Fund and under the RRO 2002
148
.
The 1996 legislation states:
The Secretary of State may, if he thinks fit, by order specify a maximum amount or
a formula for calculating a maximum amount of grant which a local housing
authority may pay in respect of an application for a grant.
An authority may not pay an amount of grant in excess of a specified maximum
amount.
15.7 In May 2016, in answer to a parliamentary question, Brandon Lewis, the
Minister of State for Communities and Local Government re-affirmed that:
“Local authorities can provide additional top-up funding which can be
used to fund adaptations where the cost exceeds the grant limit per
applicant”
149
.
15.8 The upper limit has not been fixed at the same level since it was introduced, as
is shown in Figure 15.1. In 1989 there was no limit. Four years later it was set
at £50,000 but felt to be too high and reduced to £20,000 the following year. In
2002 it was raised to £25,000. The 2005 review proposed raising it to £50,000
147
Local Government Ombudsman, ibid.
148
Royal Collage of Occupational Therapists (2016) Care Act 2014: Guidance for Occupational
Therapists, The Disabled Facilities Grant, London: RCOT. https://www.rcot.co.uk/practice-
resources/rcot-publications/downloads/care-act-2014-dfg.
149
Royal Collage of Occupational Therapists (2016) ibid.
180
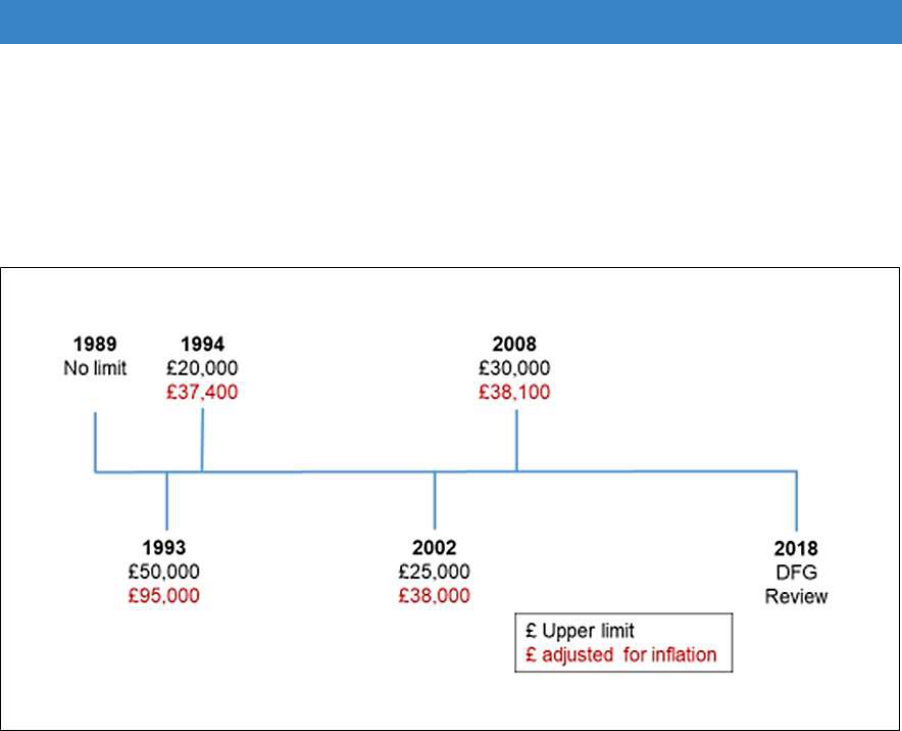
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
and taking away the means test for children. The means test proposal was
accepted and the limit raised, but only to £30,000 and it was removed for
children. If it had risen with inflation it would be around £38,000 today.
Figure 15.1 Upper limit maximum since 1989
15.9 That the upper limit was a problem was raised in discussions at the workshops
for this review, by national organisations and in previous think tanks. It is clearly
not covering the cost of work, particularly in London. Some authorities have
responded to this by raising the limit in their local area. For example, in
Portsmouth, North Kestevan and Rochdale it is £40,000; Dorset and
Manchester have raised it to £45,000 and £50,000 respectively. Other places
provide top up funding, but in many this is the form of a loan which may not be
affordable for people with high mortgage costs.
15.10 Finding the additional funding can lead to long delays for people with some of
the most severe impairments or most restricted levels of mobility who are most
urgently in need of help. For families with disabled children, already near
breaking point, any delays need to be avoided.
Options for change
15.11 The question the review was asked to address was: is £30,000 the correct
level to:
Deliver value for money to the public sector?
Support as many people as possible?
Maintain the financial viability of the grant?
181
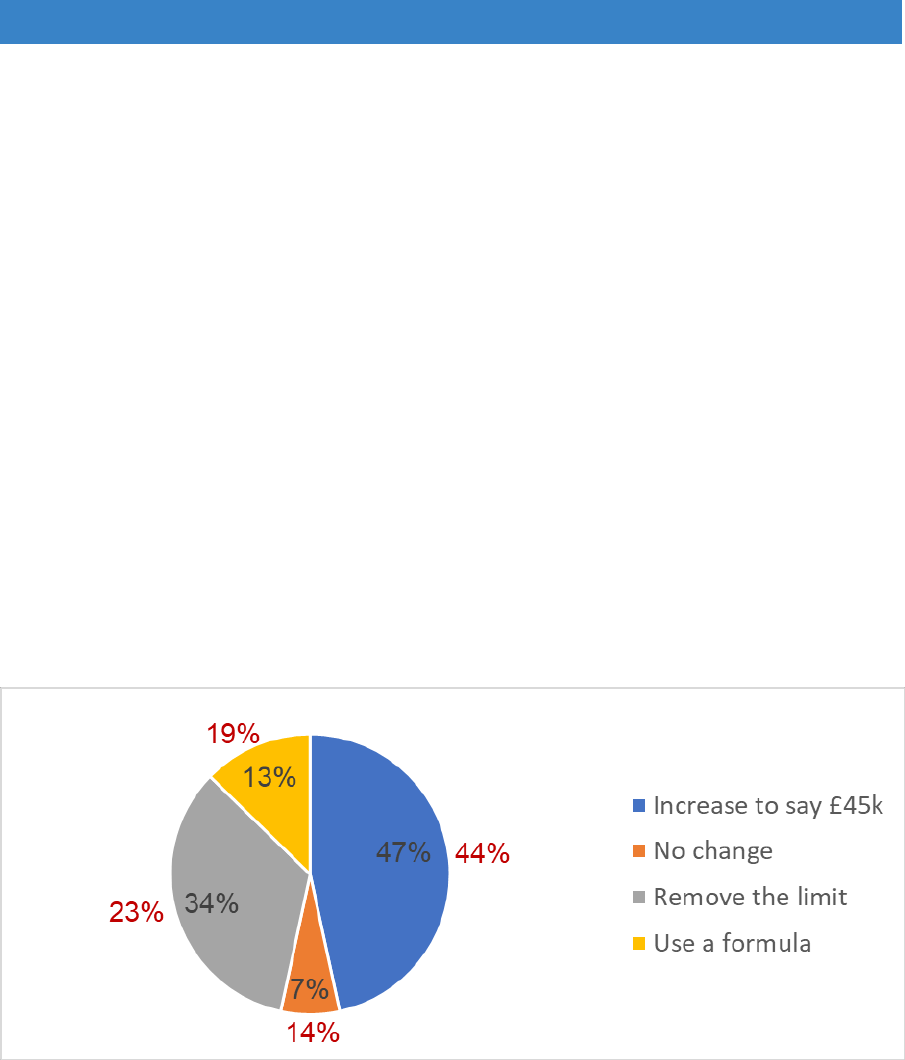
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
15.12 To find out what people delivering the DFG thought should happen, four options
were given to the people attending the consultation events and in the online
survey. These included:
No change
Raising the limit to, say £45,000
Removing the limit
Using a formula.
15.13 The results showed that only a small proportion wanted to keep the limit as it is
(Figure 15.2). The majority (47% at the workshops and 44% online) were in
favour of keeping a limit but raising it to £45,000 (or an agreed amount). Just
over a quarter of the online respondents and a third of the workshop participants
wanted to remove the limit entirely. The original legislation stated that the
Secretary of State could specify a formula. This option got a more muted
response with only 13% of workshop participants and 19% of online
respondents in favour.
Figure 15.2 Results of consultation – upper limit
Source: voting at consultation events / online survey
The evidence for change
15.14 The LOGASnet data show that most grants are quite small. The average was
between £6,000-8,000 until 2016/17 when it jumped up to about £9,000. This
was probably an adjustment to accommodate rising building costs when
additional funding was introduced and the increasing complexity of cases as
discussed in Part A. Costs vary between unitary and district authorities,
probably because higher costs in London raise the averages for the unitaries
(Figure 15.3).
182
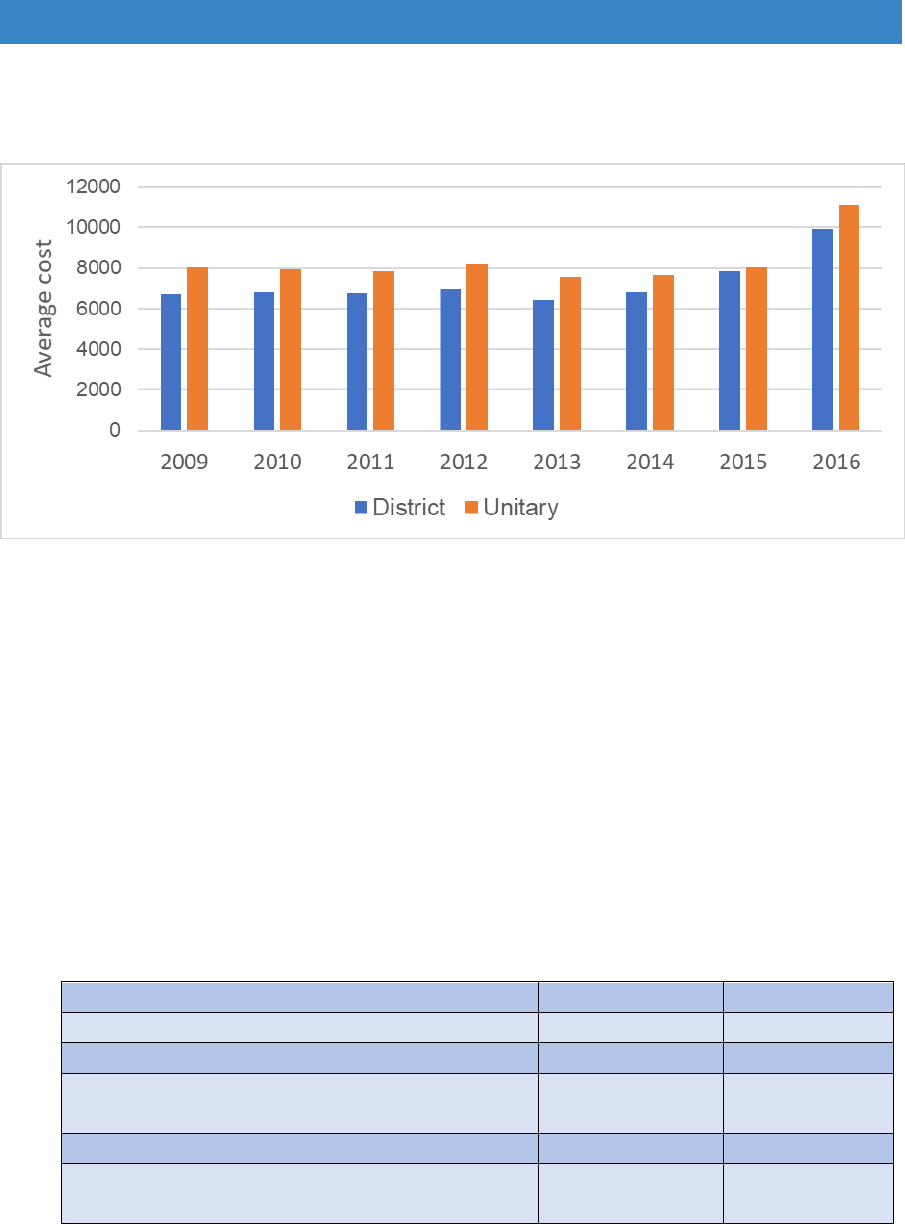
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 15.3 Average size of grant by type of authority
Source: LOGASnet
15.15 Table 15.1 reveals that very few maximum grants are approved in any authority
(district or unitary) when compared to both allocations and expenditure. Overall
unitaries and districts award around 2.5 max grants per £1m spent. Unitaries
were more consistent in the numbers of maximum grants given in 2016/17. Only
11% did none, but districts were more varied and almost a third (32%) did none
at all. The propensity to give maximum grants does not seem to relate to overall
spending levels (Figures 15.4 and 15.5).
Table 15.1 The variation in numbers of maximum grants by type of authority
Districts
Unitaries
Maximum grants per £1m DFG allocation
2.47
2.44
Maximum grants per £1m DFG
expenditure
2.56
2.55
Number of maximum grants in 2016/17
32%
(44 out of 147)
11%
(10 out of 88)
Source: LOGASnet
183
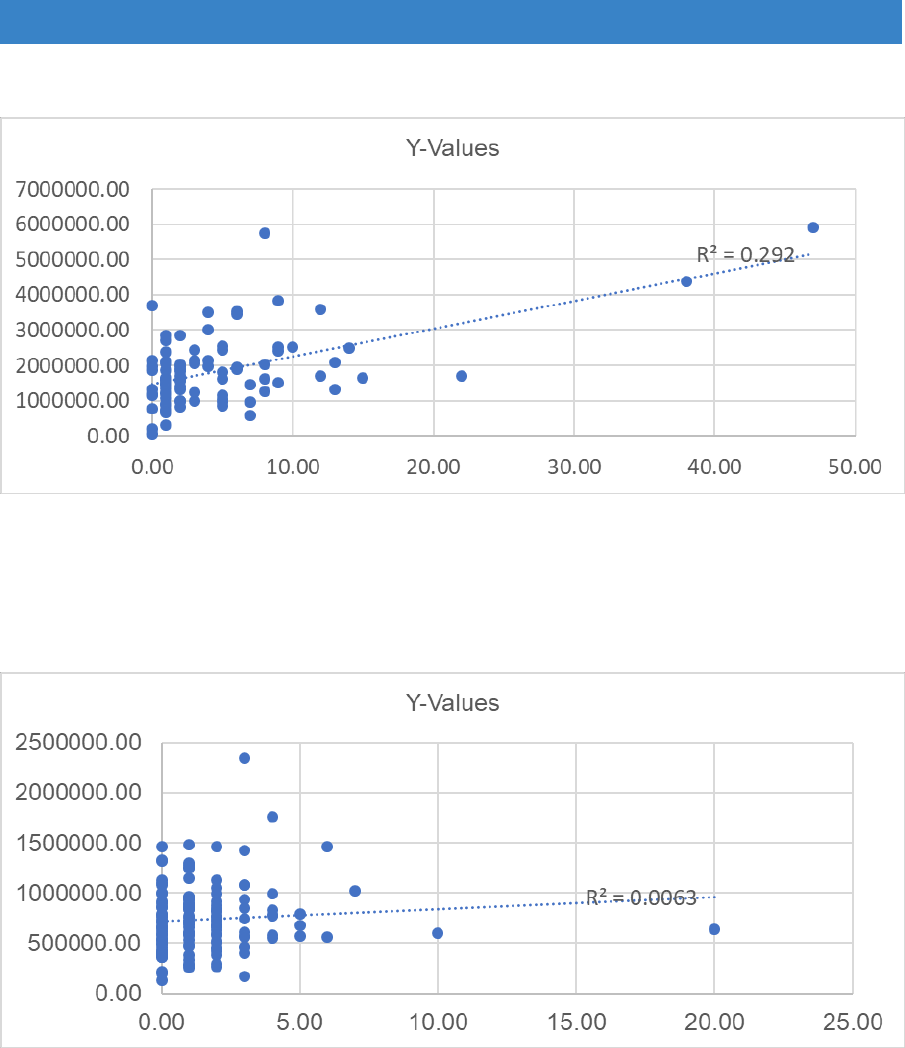
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 15.4 Unitary – spend v max grants 2016/17
Source: LOGASnet
Figure 15.5 District spend v max grants 2016/17
Source: LOGASnet
15.16 As we revealed in Part A, there is significant variation in the cost of
bedroom/shower room extensions across the country (particularly in London)
(Figure 15.6).
184
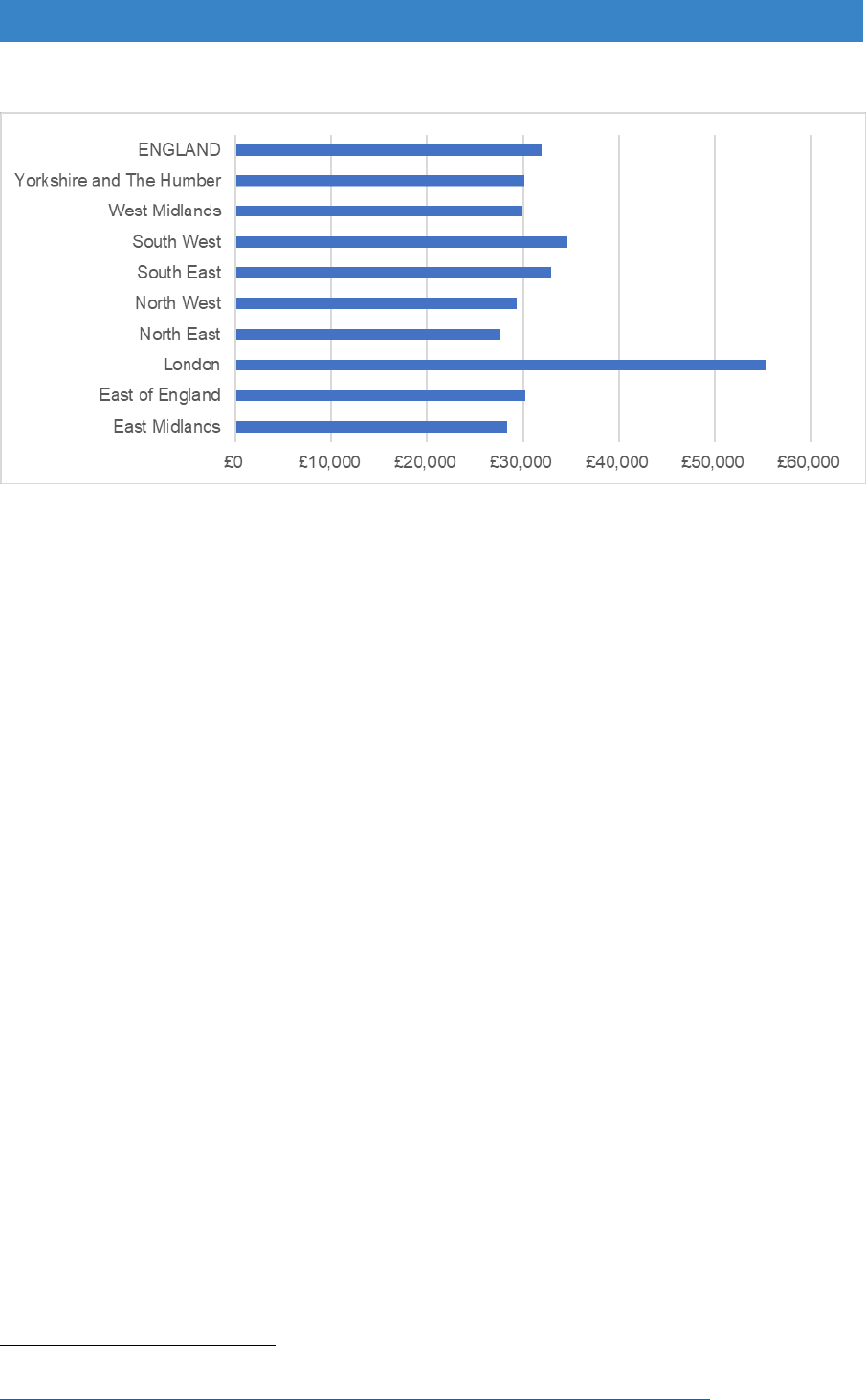
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 15.6 Average extension costs by region 2016/17
Source: Foundations FOI 2018
15.17 In the feedback we received from the workshops and online survey, two other
issues were highlighted as significant issues:
VAT - For most adaptations involving access or bathing, building works
are zero rated. But where space is created for a new bedroom, or a
kitchen, that proportion of the project is subject to VAT at the standard rate
of 20%. For a typical extension it can add over £4,000 to the total cost. We
heard examples of different interpretations of the rules taken by different
contractors and agreed with inspectors. For example, one ingenious
contractor successfully argued that 40% of a bedroom should be zero
rated because it was also the access to an en-suite shower room.
An alternative way of dealing with VAT is proposed in the 2018 London
Housing Strategy
150
. This points out that the VAT on home improvements is
charged at the standard rate of 20%, compared with a lower rate of 5% on
building a new home. The report suggests that lowering the rate for home
improvements to 5% would incentivise homeowners to undertake more
building work which would add to employment, economic activity and tax
revenues; offsetting losses from the lowered rate.
Fees - larger adaptations can be complex construction projects which
require knowledge and expertise to deliver successfully. A typical fee for
design and project management is around 10%-12%, adding another
£3,000+ to an extension costing £30,000. We heard a number of examples
of projects proceeding without professional support due to the fees taking
costs above the upper limit but suffering from significant delays and other
problems as a consequence.
150
Greater London Authority (May 2018) London Housing Strategy, Section 5.39, p. 145 [online]
https://www.london.gov.uk/sites/default/files/2018_lhs_london_housing_strategy.pdf.
185
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
The problems of under-specification and lack of professional support
In an online survey of 76 disabled people (74% families with children) in 2017, by the
charity Inclusive Home, 52% had experienced problems with the design, building
work or equipment installed as part of their adaptation scheme. These are some
examples of the comments:
"Wet-room floor tiles have come up and the bathroom often floods...."
"Toilet in wrong place windows not fitted properly toilet flooring bubbling."
"Ramp unsuitable so have to move, so no work can be completed."
"Toilet needs re-positioning but can't face the upheaval at the moment."
"Designed wrongly so can't have tracking hoist. Toilet system installed wrong, so
waste comes up shower and toilet."
"3 years later I am still suing the 'professionals' involved for breach of contract
and poor workmanship. House ruined, some rooms still unusable. So stressful
and upsetting."
The builder messed up the foundations “so front of extension narrower than back
but apparently was too late to sort when building inspector turned up - we didn't
find this out until it was built. Shoddy workmanship wet room floor had to be relaid
as done incorrectly. He didn't put electric shower in as discussed at pre-build
meeting."
"Back patio laid above damp course of conservatory so we had to pay for
drainage."
Source: Inclusive Home
Move away from one size fits all delivery
15.18 Reviewing the evidence, there are few expensive grants, and they seem very
different from the main work of adaptation teams which is to provide showers,
stairlifts, ramps and other adaptations under £10,000. The nature of expensive
cases is usually much more complex. They are often children with complex
needs, people who have had strokes, those involved in major accidents or
people with long-term conditions such as motor neurone disease, multiple
sclerosis or Huntington's disease.
15.19 At the moment, decisions seem to be cost-driven, as so many are around or
within the £30,000 upper limit. Raising the limit and changing the way decisions
are made could alter the thinking about these grants from ‘expenditure’ to
‘investment’. It would allow a much more person-centre approach which could
provide long-term solutions to increase disabled people’s independence.
Setting a maximum amount
15.20 Taking an investment approach means that the beneficiaries of the investment
must have a meaningful role in the decision-making process. In the case of
large and complex adaptations, the beneficiaries will be: 1) the disabled
186
Disabled Facilities Grant (DFG) and Other Adaptations Main Report
person, their families and carers; and 2) local health and social care
commissioners.
15.21 For commissioners, this means a number of considerations, including:
1. Alternative interventions that may achieve the same or better outcomes,
such as specialist equipment or alternative living arrangements
2. The anticipated costs of care and support if suitable adaptations aren’t
provided
3. An appropriate level of investment in the circumstances.
15.22 We considered developing a standard formula using these factors but didn’t
consider it viable given the wide range of potential circumstances. We also
discarded the option of removing the upper limit completely, as it could negate
the need for commissioners to engage and place undue strain on Housing
Authorities, particularly on smaller District Councils.
15.23 The remaining option is to increase the maximum limit. However, the variation
in building costs across the country means that a one-size-fits-all figure is going
to be problematic. We therefore recommend that the maximum amount is raised
in line with inflation, with a regional weighting based on building costs.
15.24 Due to the importance of professional expertise on these larger projects, we
also recommend that the regional upper limits are increased by a further 10%
to ensure that support is provided.
Table 15.2 Maximum Grant Formula
Region
Existing
Max
With
Inflation
Cost
Variation
Net
Grant
Upper Limit
inc 10% fee
North East
£30,000
£38,500
100%
£38,500
£42,250
North West
£30,000
£38,500
97%
£37,250
£41,000
Yorkshire and
Humberside
£30,000
£38,500
95%
£36,500
£40,250
West Midlands
£30,000
£38,500
92%
£35,400
£39,000
East Midlands
£30,000
£38,500
94%
£36,250
£40,000
East Anglia
£30,000
£38,500
100%
£38,500
£42,250
South West
£30,000
£38,500
100%
£38,500
£42,250
South East
£30,000
£38,500
109%
£42,000
£46,250
Outer London
£30,000
£38,500
105%
£40,500
£44,500
Inner London
£30,000
£38,500
111%
£42,750
£47,000
Source: https://www.costmodelling.com/regional-variations - Inflation from April 2008 to April 2018
187
–
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
15.25 The main beneficiary is the disabled person and their family, and it is essential
that they are involved in the decision-making process from the outset.
15.26 With the significant discretion that Local Authorities hold to make appropriate
decisions around investing in large scale adaptations, it is important to ensure
that discretion isn’t fettered, and grant applicants know how decisions have
been reached. We therefore recommend that, in cases where the cost of
meeting an assessed need exceeds the new upper limits, a notice must be
issued explaining the decision.
15.27 To ensure that potential applicants know the maximum amount for their area,
this should be stated on the Local Authority website. It will also be listed on the
national www.adaptmyhome.org.uk website which also includes the contact
details of every local authority in England for DFG.
15.28 As noted previously, a number of local authorities already routinely fund
applications in excess of the current upper limit, and not all cases would
necessarily increase in cost if the limit were raised. This makes it difficult to
estimate the cost of these recommendation but in the worst-case
scenario the additional annual cost would be around £25m.
Joint funding, risk sharing and joint decision-making
15.29 In Chapter 13 ‘Other funding issues’ we discussed the need for risk sharing
using contingency funds held by county authorities or a regional grouping of
authorities, so that smaller authorities are not overburden by the financial costs
of providing expensive grants. As highlighted in Part A, the number of grants
awarded in excess of £15,000 is relatively small, but they are often the cases
that are subject to the longest delays, as alternative sources of funding are
sought. A risk sharing arrangement would ensure that the risk is shared, rather
than falling on a single district with a limited budget to ensure:
Funding is always available.
To allow longer term planning for the disabled person and their family,
rather than decisions being budget-driven.
In some cases - to enable the right specialist expertise to be provided,
which might not otherwise be available in a relatively small authority.
15.30 The funding chapter also showed that different decisions that are of more
benefit to the disabled or older person may be possible if funding is combined
in different ways. For example, instead of adapting a kitchen, a riser
wheelchair could be provided which would not only give independence in the
home but would also allow more freedom in other setting such as shops and
supermarkets. It is also possible to bring in resources from other budgets if
there is a business case for savings to health and care services.
188

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Moving rather than adapting
15.31 Rehousing is an alternative to providing adaptations where it would provide a
better solution, where the household is willing to move and if costs are likely to
very high. Adapting an alternative property is allowed under an RRO and the
costs of moving can be included.
15.32 Change management work in Bristol showed that it was possible to ask people
if they would consider moving at the point of initial assessment in social care.
Bristol employed a rehousing officer which allowed 26 households to move and
saved £477,000 in adaptation costs in the first 9 months it was in operation.
Incentives to move, such as removal costs and new carpets and curtains, were
seldom needed. The cost of DFG adaptations in the new dwellings was very
much lower than improving the existing home, and it provided better solutions
to people’s needs
151
.
15.33 Rehousing requires close collaboration with registered providers, council stock
providers, other local landlords and estate agents to ensure that people can be
helped to move within reasonable timeframes. It is also necessary to keep
people on the DFG waiting list in case a move proves to impossible to achieve.
15.34 Housing options advice and rehousing services require added revenue funding
on top of that for DFG delivery. With pressures on local authority resources,
many of these non-mandatory services have been discontinued. In 2015/16
only 20% of authorities provided support for people to move rather than
adapting, and only 268 people were helped to move that year across the whole
country (Foundations FOI, 2016). Given the savings to DFG budgets, these
services could pay for themselves in a relatively short period of time, but again
it needs better strategic management at local level to enable this to happen and
the engagement of social housing providers and development planners on
those boards.
15.35 People also need time to think about moving. The current national advice
service, FirstStop, has a housing options tool and information about moving.
This web and telephone help facility needs to be updated so that more people
can get access to advice and information and begin the process of considering
their housing options. It also needs to address the needs of younger disabled
households who are more likely to want to move.
15.36 There is also scope to use volunteers. Evaluation of Care & Repair England’s
‘Silverlinks’ service showed that older people are looking for trustworthy,
impartial information and advice on housing options, plus the interconnected
151
Mackintosh, S. (2012) From Home Adaptations to Accessible Homes: Putting people at the heart
of redesigning the adaptation service in Bristol, Housing LIN Case Study no 62.
https://www.housinglin.org.uk/_assets/Resources/Housing/Practice_examples/Housing_LIN_case_stu
dies/HLIN_CaseStudy_62_Adaptations.pdf.
189

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
issues of care and finance
152
. The older volunteers have no agenda - they share
their own experiences but are not there to persuade anybody to make a
particular choice. A volunteer can allow space for the person to talk through
options and reach the decision that’s right for them without feeling under
pressure. When asked about why the Silverlinks approach works, volunteers
said that people find it much easier to relate to another older person who has
gone through similar experiences.
Summary about the upper limit
15.37 Larger adaptations are very different in nature to the relatively straight-forward
showers, ramps and stairlifts that make up the majority of the DFG programme.
A traditional one-size-fits all approach to delivery has not necessarily reflected
the expertise required to successfully complete a complex project.
15.38 Large adaptations have also been hampered by an often inflexible upper limit,
resistance to risk sharing and silo working. There should be a shared
understanding of the need to invest and the benefits that will accrue, not just
from DFG funding, but from the wider housing, health and social care economy.
15.39 The disabled person and their family should be party to the decision-making
process and understand the rationale for decisions made. They also need to be
given help to move where this might provide a better solution.
Regulatory Reform Order (RRO)
15.40 The Regulatory Reform (Housing Assistance) (England and Wales) Order 2002
enables authorities to offer financial assistance tailored to the needs of their
area. The Government provided guidance in 2003
153
and further changes were
made in 2008 following the last review of the DFG
154
. More recently,
Foundations has provided a guide to preparing a policy
155
.
15.41 The RRO allows authorities to meet people’s needs without going through the
full DFG process. The financial help provided by an RRO policy must provide
at least the same level of assistance as the mandatory DFG and not fetter
discretion in decision-making. For example, an authority cannot refuse a full
152
Care & Repair England (2016) Making the Housing Connections: An interim evaluation of the
Silverlinks Programme. https://silverlinksprogramme.files.wordpress.com/2017/01/silverlinks-interim-
report-1.pdf.
153
http://webarchive.nationalarchives.gov.uk/20120920034634/http://www.communities.gov.uk/docum
ents/corporate/pdf/145088.pdf
154
Department of Communities and Local Government (2008) Disabled Facilities Grant – The
Package of Changes to Modernise the Programme, London: DCLG.
155
Foundations (2016c) Preparing a policy under the Regulatory Reform Order (2002) Housing
renewal. www.foundations.uk.com/media/4696/preparing-a-policy-under-the-rro.pdf.
190

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
DFG to an individual who requests it, neither can they provide a loan to
someone who might otherwise be eligible for a grant.
15.42 Using an RRO policy allows more flexibility in the types of work that can be
provided. It can also be substantially quicker. Some authorities use the RRO to
dispense with the means test for all work under a certain amount to speed the
process. This also helps to remove any stigma people associate with means
testing to get more people to come forward. They have also reduced the grant
paperwork to make any forms much simpler and easy to fill in. The Cerebra
research discussed in Part A showed that forms can still be complex, and only
a few authorities have forms readily available online.
15.43 To use the freedoms contained in the RRO authorities must develop a policy to
set out how they intend to use their powers, what resources are available and
how these have been determined. The policy must be strategic and clearly
linked to overall objectives such as those for the Better Care Fund. It needs to
be equitable and fair, show the eligibility criteria and set out which groups of
people it intends to benefit. It must also have clear, measurable outcomes.
Once drawn up the policy must be approved, a notice published, a copy made
publicly available and a summary provided on request.
15.44 Grants can be given for a range of different types of work, including:
Relocation grants
Hospital discharge grants
Safe and secure grants
Handyperson services
Fast provision of ramps or stairlifts
Palliative care
Dementia grants
Adaptations for people with a learning disability
191
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Dorset RRO policy
The Dorset Accessible Homes Service (DAHS) covers four districts and two borough
councils (Christchurch, East Dorset, North Dorset, Purbeck, West Dorset and
Weymouth & Portland). Their RRO policy has been operating since 2016. It includes
four different discretionary grants or services:
Accessible Homes Grant - is a grant similar to the DFG but more flexible and easier
to administer. There is no means test for works under £5,000 (including fees and VAT).
For work costing more than £5,000 there is a means test (the part under £5,000 is
excluded) but passporting is used for people on a wide range of benefits. As with the
DFG, families with children are not means tested. Types of work are similar to the DFG
but have been extended to include sleeping space for carers and to cover reasonable
expenses in helping a disabled person and their family move home. To cover the full
cost of works the upper limit is set at £45,000 rather than the statutory £30,000. They
charge an agency fee of no more than 10% of the cost of works included in the grant.
Safe and secure grant - helps low income home owners and tenants carry out minor
adaptations, small repairs and the installation of assistive technology. Applicants must
be aged 50 and over and be disabled or the parent or guardian of someone disabled.
Low income is determined by being on at least one of a list of benefits. The aim is to:
reduce accidents around the home; allow independent living; and help with discharge
or prevent admission to hospital. However, the grant is not available where the works
would be considered the legal responsibility of a landlord. Grants range in size from
£50 to a maximum of £2,000 and are limited to £6,000 in total over a three-year rolling
period, including a 10% agency fee.
Handy Van Service – this is available for disabled people or those over 50 years of
age. People pay for the cost of materials: those on benefits pay no labour costs; those
who are not pay £20 per hour.
Loans - available from two councils (West Dorset and Weymouth & Portland) to help
people to: improve their homes to meet the Decent Homes Standard; remove
Category 1 hazards; address fuel poverty; bring an empty property back into use;
improve defects in park homes; or assist people where the maximum grant of £45,000
will not meet the cost of works and no other public assistance is available. The current
maximum loan is £15,000.
192
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Cheshire East RRO policy
A Regulatory Reform Order policy supports a holistic approach to help people live
independently. Key features include:
Maximum DFG of £50,000 so that expensive/complex adaptations can proceed
quickly without delays trying to get funding
Loans to help people to pay means tested contributions
Loans to extended family/separated parents so disabled people can be cared for
by their family
Relocation grants to help with the cost of moving
Grants and loans for foster carers to care for disabled children
Combining DFGs with other funding streams (including social care and charitable
funding) for urgent care needs including hoists and lifts
Affordable warmth grants to improve wellbeing
Combined grant and loan funding so people can adapt their homes in a way that is
more aspirational than functional
They work closely with occupational therapy teams, the visual impairment service, the
independent living centre, vulnerable people champions, hoarding practitioners’
group, community agents and local area co-ordinators. There is a Handyperson
service for minor adaptations and repairs. Individual partnership agreements enable
joint working with housing providers, including three transfer associations.
Early intervention through equipment and adaptations is delivered by a trusted
assessor who works across the HIA and the occupational therapy service. Clients are
referred by the occupational therapy referral & advice team and holistic assessments
are undertaken in the Independent Living Centre or the persons own home. There is
a separate priority pathway for urgent cases such as end of life care, transfer of care
and risk of injury.
Quicker service: A lean systems approach reduced adaptation timescales by four
months, which was reduced further by a framework agreement for level access
showers with a target for installation within six weeks.
Outcomes: They measure resident outcomes including: personal dignity, emotional
wellbeing, reduced reliance on informal carers and prevention of hospital admissions.
A small-scale research project after installation of level access showers showed that,
despite worsening health, most individuals had been able to live completely
independently in their own homes for the next two years.
15.45 All authorities that have developed integrated adaptation service also have an
RRO policy. However, in 2016/17 an FOI showed that overall only half of
authorities had an RRO policy. Many appear to be held back by lack of staffing
resources, absence of strategic management support or worries about the audit
process if they give discretionary rather than mandatory grants. There is a need
to encourage every authority to develop an RRO as part of the integration
process.
193

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Suitability of the 6-month time limit
15.46 The six-month time limit is not working as it was envisaged in the original
legislation. This said that the council shall approve or refuse an application ‘as
soon as reasonably practicable, and, in any event, not later than six months
after the date of the application’.’ It reflects a time when housing authorities
controlled the whole process as part of housing renewal work. When the service
is split between administrative departments, delays are not just with the housing
authority. It does not reflect the customer’s experience as they may have
already spent six months or more on a waiting list for an assessment before
they get to the application stage.
15.47 It is also a rule that people get around as was shown in Part A. When there are
waiting lists, authorities manipulate the dates by not allowing the application
until they know it can be approved within the timeframe.
15.48 As the 6-month time limit is part of the primary legislation, we recognise that is
it more difficult to revise and may be appropriate for a small minority of cases
where an applicant submits an application without prior consultation with the
local authority. However, we recommend that the requirement to approve or
refuse and application “as soon as reasonably practicable” is stressed within
revised guidance and should in most cases take no longer than 4 weeks.
Other regulation
The Services and Charges Order
15.49 The 1996 Services and Charges Order lists the services and charges which
may be funded using the DFG
156
. The current list includes:
Confirmation, if sought by the local authority, that the applicant has an
owner’s interest
Technical and structural surveys
Design and preparation of plans and drawings
Preparation of schedules of relevant works
Assistance in completing forms
Advice on financing the costs of the relevant works which are not met by
grant
Applications for building regulations approval (including application fee and
preparation of related documents)
Applications for planning permission (including application fee and
preparation of related documents)
Applications for listed building consent (including application fee and
preparation of related documents)
156
The Housing Renewal Grants (Services and Charges) Order 1996.
http://www.legislation.gov.uk/uksi/1996/2889/made
194

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Applications for conservation area consent (including application fee and
preparation of related documents)
Obtaining of estimates
Advice on contracts
Consideration of tenders
Supervision of the relevant works
Disconnection and reconnection of electricity, gas, water or drainage utilities
where this is necessitated by the relevant works
Payment of contractors
The services and charges of an occupational therapist.
15.50 To ensure that housing options are considered during assessment, we
recommend that the costs associated with moving home, including the
provision of practical support, should be added to the list. The requirement to
be ‘necessary and appropriate’ and ‘reasonable and practicable’ would still
apply, which means that moving would typically be a lower cost option than
staying put.
15.51 An omission from the current list is the funding of extending warranties on items
like lifts and hoists. It is cited as good practice within the current guidance and
therefore we recommend that the regulations are amended accordingly.
Other Funding Considerations
15.52 The guidance circular that accompanied the legislation in 1996 said that it was
for ‘housing authorities and social services authorities between them to decide
how particular adaptations should be funded’ either through what’s now the
2014 Care Act or through a DFG.
15.53 The guidance went on to note that it was common practice for equipment which
can be installed and removed fairly easily with little or no structural modification
to be the responsibility of the social services authority.
15.54 This demarcation between works with or without structural modification has
worked well for the most part but has caused issues where it has been rigidly
enforced. For example, we heard that in many areas it is common for a shower
adaptation to be funded from DFG, but a free-standing shower chair to be
funded by social services. In many cases, this means delays between the
completion of the adaptations and the delivery of the shower chair, with the
result that the disabled person either cannot safely use their new adaptation or
that they have to use a patio chair in the interim.
15.55 We also heard of cases where a ceiling track hoist is funded by a DFG but the
slings are funded by social services, resulting in separate orders and delays.
195

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
15.56 In Staffordshire they recognised this issue, and the housing and social services
authority decided that it was sensible for the initial purchase of items like shower
seats and slings to be included within the DFG – similar to the way ink is
included when you buy a printer. Replacements will be funded by social
services.
Need for clearer guidance
15.57 Throughout this review, it has become clear that the application of the
legislation, various regulations, general consents and orders, guidance, good
practice guides and use of the Regulatory Reform Order have created a
complicated system that few people fully understand. Much of the wording,
particularly from the legislation and original regulations, is old fashioned and
doesn’t properly consider issues around learning disabilities, behavioural
issues, mental health, and dementia. For anyone new to the delivery of DFG,
there is a very steep learning curve.
15.58 This review sets out a new way of approaching DFG, as part of joined up range
funding and services that puts the disabled person at the centre of the process.
It is recommended that the guidance is fully revised so that it clearly sets out
expectations for local authorities and rights of a disabled person making an
application.
Recommendations – regulation and the upper limit
That the maximum amount of the DFG is raised in line with inflation, with a
regional weighting based on building costs and an amount for professional
fees.
That the VAT rules are revisited for major adaptations.
Regulatory Reform Order (RRO) Policies have been developed in about half
of local authorities and need to be adopted in all areas to provide more
flexible use of the grant.
Each area to have simple application forms available on request.
Applications should be determined within four weeks where the Local
Authority has had prior involvement with the application.
That the guidance is fully revised to reflect integrated services, the
expectations for local authorities and the rights of the disabled person.
That the Services and Charges Order list is updated to include support with
moving and the funding of extended warranties.
That the national advice line is updated and improved to give people support
with housing options.
196

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 16. Developing a market
The current situation
16.1 The evidence from the review has been mixed. There are areas that have
transformed their services and have fast, flexible integrated delivery but there
are more traditional approaches elsewhere. Some areas allow DFG customers
to personalise the specification, and upgrade or add products at their own
expense, but others do not.
16.2 Innovation in design and the introduction of new products and materials is also
uneven. Restrictions on expenditure have made it difficult for staff to get to trade
shows and training events, research new products and designs, cost them and
get them into standard schedules. A focus on value for money has meant that
teams go for the lowest tender submission and do not look at the quality of the
outcomes that the price will deliver. We know that many people drop out of the
DFG process, but we don’t know how many never come forward at all because
of the stigma attached to out of date designs.
16.3 But change is happening, and interesting trends are emerging that could
revolutionise the types of adaptations that are delivered. New products are
market driven and mainstream which means that everyone can benefit, not just
the small proportion of disabled and older people who happen to get a DFG.
16.4 The chapter looks at the need to change the way building work and adaptations
installation is procured to make it more consistent and efficient and to drive
innovation. It looks at the revolution in personal assistive technology and the
‘internet of things’ that is allowing disabled people to control their home through
their smart phones. Finally, it looks at how to help people outside of the DFG
and the role played by both the market and the public sector.
Procurement
Need for Change
16.5 Construction procurement practice is recognised to be poor in the UK,
particularly in the public sector. This leads to waste and inefficiency. For DFG,
this is made worse by low levels of standardisation in home adaptations and
the fragmentation of local authority delivery.
16.6 The 2006 Good Practice Guide suggested that Local Authorities set up a
schedule of rates for carrying out adaptations works, noting that “once in place
the benefits of such a system are considerable: costings can be calculated
197
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
directly from the specification, a cost of works fixed and the level of grant
assessed without waiting for tenders to be returned and evaluated”
157
.
16.7 However, research by Foundations found that around two-thirds of DFG funded
adaptations are still costed by seeking two or three quotations from local
builders based on an ad-hoc specification. In turn, the builders will use local
subcontractors and source materials via builders’ merchants.
Figure 16.1 Typical DFG Supply Chain
Client
Local Authority
Main
Contractor
Subcontractors
Builders Merchants
Manufacturers
16.8 Over 80% of the annual DFG programme is delivered by building firms adapting
existing housing. The UK construction industry is highly fragmented, with over
300,000 businesses (of which 99.7% are small and medium-sized enterprises
- SMEs)
158
. The delivery of DFG is also disjointed, carried out through 326 local
housing authorities across England with little collaboration or consistency,
particularly around procurement practice.
16.9 In their report on the role of local authorities in housing for disabled people, the
Equalities and Human Rights Commission found that on average it took 14
157
Department for Communities and Local Government (2006) Delivering Housing Adaptations for
Disabled People: A Good Practice Guide. London: DCLG.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/78
21/138595.pdf.
158
HM Government (2018) Industry Strategy: Construction Industry Deal [online]
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/73
1871/construction-sector-deal-print-single.pdf.
198

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
weeks to install an adaptation after a DFG had been approved
159
. The biggest
challenge identified by local authorities was the difficulty in finding reliable
contractors to carry out the works. Typically, a local authority will have an
approved list of builders that has been built up over several years. There is
currently no consistent method of assessing the quality and suitability of
builders to carry out home adaptations.
16.10 The EU funded Seas-2-Grow project has also investigated the UK market and
found that “there are few mechanisms unifying suppliers of innovations
specifically for the elderly”
160
. This often means that equipment meant to help
make life easier has been designed more for a hospital rather than a home,
such as grey padded shower seats and white plastic support rails. During a
roundtable with manufacturers and suppliers we heard that a recent local
authority tender had a score profile of 10% for quality, 90% for price. Even for
a simple product such as a grab rail, the research and development and
subsequent tooling costs can run into thousands of pounds, which has to be
recovered in a unit cost “which LA's are not prepared to pay so where is the
incentive to change?”.
16.11 The Latham
161
and Egan
162
reports recognise the need for clients and suppliers
to improve their collaboration, working with fewer suppliers in a more settled
supply chain. In the wider construction industry this has generally been
achieved by the creation of frameworks which then stay in place for a fixed
period of up to 4 years. However, there can be a tension between the benefits
of working with fewer suppliers in a long-term relationship and the benefits of
maintaining a market which is accessible to new entrants with associated
competition and innovation. Frameworks can also stifle continuous
improvement and tend to lock out smaller local companies.
16.12 Some local authorities use frameworks and schedules of rates to improve the
efficiency of their procurement process, but this is generally done at a local level
with the intention of reducing cost rather than developing the market.
16.13 The challenge then, is to use the £0.5bn annual DFG budget to improve design,
shorten timescales and retain control of costs.
159
Adams, L., Morris, S., Thomson, D., Rossiter, H., Felton, J., Newbold P. and Hazel, Z. (May 2018)
Housing and disabled people: the role of local authorities, London: EHRC.
https://www.equalityhumanrights.com/sites/default/files/research-report-115-housing-and-disabled-
people-the-role-of-local-authorities.pdf.
160
Seas 2 Grow (2017) Silver Economy Accelerating Strategies: Market Study.
https://www.seas2grow.com/wp-content/uploads/2017/06/SEAS-2-Grow-Market-Study-EN.pdf.
161
Latham, M. (1994) Constructing the Team, London: HMSO.
http://constructingexcellence.org.uk/resources/constructing-the-team-the-latham-report/
162
Construction Task Force (1998) Rethinking Construction, London: Dept of Trade and Industry.
http://constructingexcellence.org.uk/resources/rethinking-construction-the-egan-report/.
199

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Procurement Reform
16.14 The main barriers to better design and innovation are the lack of integration in
the market, and the lack of standardisation and repetition in specification. The
traditional procurement processes of seeking multiple quotations has reinforced
these barriers. Addressing them calls for both reform of procurement processes
and greater efficiency in their operation.
16.15 Often, procurement is seen as a standalone process at the start of a
construction project. For home adaptations, it is worth considering whether the
inclusion of ongoing servicing and maintenance for equipment like lifts and
hoists should be included. There is also a question about whether design and
construction should be procured and/or provided separately when staffing can
cost up to 24% of an average DFG
163
.
16.16 From our research into best practice across the sector, we would like to
highlight the following as ways in which significant improvements can be
achieved at a local level.
Schedule of Rates
16.17 Chorley Home Improvement Agency use an online schedule of rates for all their
shower adaptations. They have set out a standard specification that has been
pre-priced by their list of approved contractors. For each project the HIA select
the appropriate items to build up the schedule of works, and in the background
the system adds up the rates submitted by each builder to provide instant
quotations. They select the successful contractor by looking at price and past
performance.
16.18 The process is quick and easy to carry out and saves three or four weeks
compared to a traditional paper-based approach. It also means that if a
contractor is unavailable for some reason, the HIA has alternative quotes
already prepared. The online system also allows for fixed price materials from
a framework and a series of alternative options to allow for client choice.
Flat-pack extensions
16.19 Where a DFG involves an extension, usually to provide a ground floor bedroom
with en-suite shower room, the construction will typically be based on a
traditional structure of bricks and blocks to match the existing property. This
tried and trusted approach has three significant disadvantages: 1) it takes many
weeks to build, with all of the inherent disruption; 2) it is very messy, particularly
if it rains when the foundations are being excavated; and 3) uncertain ground
conditions can lead to significant extra costs.
163
Curtis, L. and Beecham, J. (2018) A survey of Local Authorities and Home Improvement Agencies:
identifying the hidden costs of providing a home adaptations service. https://kar.kent.ac.uk/66433/.
200

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.20 A quicker and cleaner alternative is to use a flat-pack extension. These can be
completed in around 1 week by using factory manufactured Structural Insulated
Panels (SIP) and screw-pile foundations – an approach used in most episodes
of DIY SOS. This means less mess and disruption and much lower risk of
unexpected additional costs.
16.21 Another advantage with SIPs is thinner, but better insulated walls, which means
additional internal floor-space compared to a traditionally built extension of the
same external dimensions. In some cases, this could allow an extension to be
designed within permitted development limits and negate the need to apply for
planning permission.
16.22 In the few case studies we have seen, costs have generally been comparable
with traditional build, particularly when design and supervision costs are taken
into account. However, further development of this market would help to
enhance value for money in this area.
Stairlift loans and recycling
16.23 From Freedom of Information data, we know that around one third of social
services authorities no longer routinely pay for the servicing, maintenance and
repair of stairlifts for service users. For those that do, the number of lifts they
maintain is increasing year-on-year, with an average servicing cost of £82.50
and an average repair cost of £227.64 per year for lifts outside the
manufacturer’s warranty period.
16.24 Care and Repair Newcastle have an equipment loan scheme that effectively
provides disabled clients who have an assessed need with a stairlift on a free
loan for the duration that they need it. The scheme was introduced to make
better use of funding by recycling stairlifts
164
.
16.25 For the recipients the benefits include:
Speed of service – they have no waiting list for this service and a simplified
process means clients typically receive a stairlift between 3-6 weeks after
their initial enquiry.
Increased safety – client’s safety is increased as the period from
identification of need to installation has been radically reduced from over 12
months to 3-6 weeks.
Increased number of recipients – previously some clients would fail a means
test for a DFG and have to fund the installation, service and maintenance of
a stairlift themselves, or continue to struggle getting up and down stairs at
increased risk to their welfare.
16.26 The scheme started in June 2016 and they are now, on average, installing three
stairlifts each week and removing one stairlift each fortnight, which is then
164
http://www.careandrepairnewcastle.co.uk/how-we-help/equipment-loan-scheme/
201

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
recycled through the scheme. It is therefore recommended that stairlifts are
delivered through a non-means tested equipment loan service for speed of
service, increased safety and to reach more people in need.
Value for money, standards and cost benchmarking
16.27 To go from fragmented delivery to a more settled supply chain will require
significant co-ordination and engagement with Government and industry
stakeholders. If it is the intent of Government to use the annual DFG budget of
£0.5bn to shape the market, then it will need to lead the process, and focussed
effort will be required form all parts of the supply chain.
16.28 Improving the certainty of the forward programme by announcing a further five-
year funding profile for DFG, including local allocations, would encourage local
authorities to taker a longer-term view on procurement practice. However, we
recommend taking a lead from the UK Construction Strategy, by:
Establishing by benchmarking a challenging but realistic market price for
procurement.
Setting common standards for typical adaptations and communicating
requirements to prospective suppliers in a clear and consistent way.
Benchmarking
16.29 Cost benchmarking is required to establish better consistency of value for
money and a baseline for new cost/value-led approaches to procurement. The
benchmarking should also include project on-costs (agency fees, administration
costs, etc.) so that efficiency of the overall project is also plotted.
16.30 Clearly, where cost is a lead driver, there is a risk that the quest for the lowest
initial capital cost will take precedence over judgments made on value – and
particularly on the outcomes for the client. A vital part of benchmarking is
therefore a clear understanding of how a project will deliver benefits to the wider
public sector, so that cost benchmarks are not set at an artificially low level by
the inclusion of projects that fail to deliver wider social value.
16.31 The criteria for social value will need to be converted into standards and
specifications that can be passed to suppliers as part of the brief that they are
required to meet. There should be consistency across the country in how these
standards are set, and wherever possible they should be outcome based to
maximise the opportunities for innovation.
Common Standards
16.32 A number of frameworks for home adaptations already exist that set-out
common standards for materials. Some are let specifically for DFG projects,
202

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
typically at a local level, whereas larger scale frameworks are usually targeted
at works programmes of housing associations.
16.33 Further work is required to assess the effectiveness of these frameworks, to
ensure that they do not create a barrier to entry to the market, particularly for
SMEs at the local level, with some assurance that longer term relationships and
economies of scale will produce greater value for the taxpayer.
16.34 For builders, we recommend developing a national accreditation scheme
similar to the Certified Ageing in Place Specialists that operates in North
America. Builders undertake Trusted Assessor type training to understand the
requirements for fitting adaptations correctly as well as mentoring on how to
market and promote their services. With appropriate support this would help to
encourage more SME builders into the adaptations market for the benefit of
both local authorities and people looking for a trusted solution to carry out works
themselves. In the UK, this could be associated with the current Trustmark
registration scheme.
Assistive technology
Introduction
16.35 Technology has always been part of Disabled Facilities Grant – paying for
stairlifts, through floor lifts, and ceiling track hoists. The DFG legislation also
includes the less common control of power, heat or light as a “purpose for which
… a grant must be approved”
165
. These all form part of a wide range of
electronic assistive technology devices that function to compensate for
disabilities or impairments.
16.36 Assistive Technology has long been claimed to support independence of
service users, reduce unpaid carer ‘burden’ and to save Adult Social Care and
the NHS money by reducing need for care, preventing unnecessary
hospitalisation and delaying/preventing moves into residential care. For
example, early project evaluations generally concluded that telecare could
produce positive outcomes for people who used it, but these studies were
mostly small scale and used methods that meant their findings could not be
regarded as entirely reliable
166
. However, they did encourage more rigorous
research, including the ‘Whole System Demonstrator’ (WSD) project—a
randomised controlled trial that took place at three local authority sites. It
concluded that over a 12-month period, and using a wide range of indicators,
165
Housing Grants, Construction and Regeneration Act 1996
166
Kings College London, Background to the UTOPIA study [online]
https://www.kcl.ac.uk/sspp/policy-institute/scwru/res/utopia/background.aspx.
203

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
outcomes were not significantly different between telecare users and a control
group who received other services and support but not telecare.
16.37 Part of the problem is the way that businesses innovate for older adults and
disabled people generally. Too often these groups are seen as needing
solutions to their medical issues, like mobility or medication management. Any
concerns about self-image or style – significant concerns for any other sector
of society – are often seen as frivolous and only treated as an afterthought
167
.
As a result, a small-scale German study of telecare users found that only 14%
carried their emergency pendant with them at all times
168
.
16.38 But with the rise in smart technology, there is a growing range of solutions that
can be used to modify the home of a disabled person and increase their
independence. Excitingly, most of these solutions are part of the consumer
drive towards smarter homes and the emergence of the “Internet of Things” –
devices that are connected to the internet, can be controlled remotely and send
back data about their environment.
16.39 As the WSD study shows, we need to be aware that technology doesn’t always
deliver on its promise and we can’t realistically expect one universally designed
holistic solution or seamless integration with existing service delivery and other
devices. We’re also unlikely to see a clear reimbursement model based on
public health care financing or a clear metric for the specific impact on quality
of life at this stage. However, we could reasonably expect to see smarter
homes, targeted and personalised support for condition management,
rudimentary assessment of behaviour and a positive impact on engaging users.
16.40 When considering the role that Assistive Technology can play in DFG we have
considered only options that are:
Used in the home environment
Likely to improve the independence of the user
Available to use now.
Technology for Ageing Well
16.41 Some studies suggest ageing occurs in a predetermined order and can be
represented as a ‘curve of functional ability’ shown in Figure 16.2 below, which
167
Coughlin, J. F. (2018) The Longevity Economy: Inside the World's Fastest-Growing, Most
Misunderstood Market by Joseph F. Coughlin, Cambridge, MA: Massachusetts Institute of
Technology.
168
Heinbüchner, B., Hautzinger, M., Becker, C. et al. (2010) Satisfaction and use of personal
emergency response systems, Z Gerontol Geriat 43: 219. https://doi.org/10.1007/s00391-010-0127-4.
204
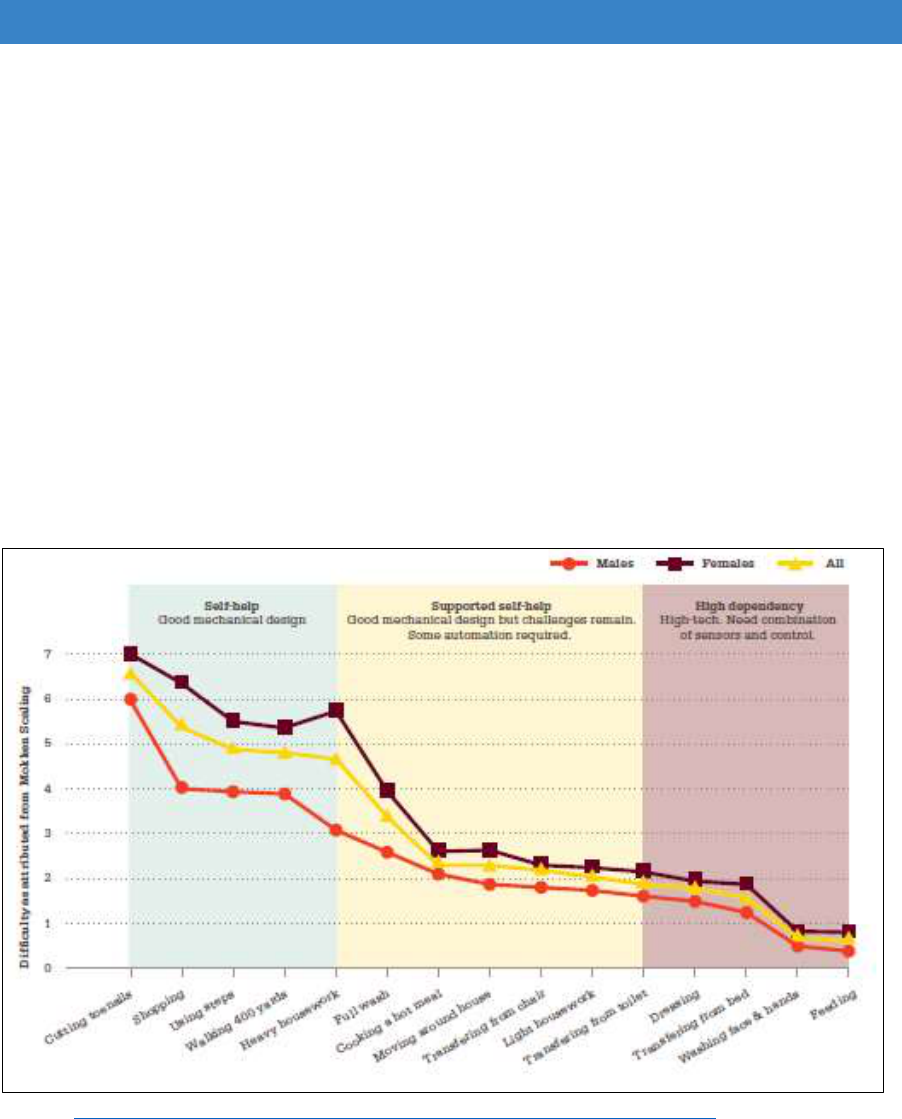
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
presents the level of difficulty the very old (85 years plus) have in performing
daily tasks of personal care, household chores and mobility. The Institution of
Mechanical Engineers defined a series of criteria for independence at home,
where the needs and applications of technology would vary depending on
where a person sits on the curve.
16.42 An opportunity exists to encourage greater activity through better home design
and adaptive and assistive technology for some tasks, such as shopping, using
stairs, housework, moving around the house, and transferring from chair, toilet
and bed. Automatic assistance could be made to help maintain maximum
activity, only providing what is necessary to encourage the older person to
maintain muscle exercise as long as possible, based on health and not age.
Figure 16.2 Curve showing decline in functional ability
Source: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0031665.
16.43 Eligibility for DFG is based on having a substantial disability and so most current
applications are for adaptations below 4 using Mokken scaling. Further
developments will require good mechanical design with some automation or
higher level of technology.
205

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Mainstreaming Assistive Technology
16.44 With the negative brand value associated with older age and disability
169
, the
growing market for the ‘Internet of Things’ is aimed at easing the lives of
mainstream consumers. It has significant potential to improve the lives of
people with disabilities by addressing issues they have identified as being
important concerns: being unable to undertake household chores; not wanting
to be a burden on family members; fear of being taken ill when alone; and fear
of accidents such as falls
170
.
Table 16.1 Amazon’s range of products and services as an example:
Amazon launched the Mayday button in
2013 – a simple click on a tablet
connects you to a tech adviser in 15
seconds or less
In 2015 they launched Home Services –
an online service where you can find
and hire vetted, licensed professionals
to come to your house and perform
services ranging from plumbing, to
cleaning, to tech support, and almost
everything in between
2016 saw the launch of the Amazon
Echo in the UK – a smart speaker that
can take voice commands to make calls
or control a range of other devices
And in 2017 they introduced Amazon
Key. A system that includes a smart
door lock that people can open and
close their doors without a key or give a
guest a code to enter their homes.
Combining these services means you could ask the Echo to contact you to the
Mayday response, arrange a cleaner through Home Services who could let
themselves into your home using Key.
169
DePoy, E. and Gilson, S. (2010) Disability Design and Branding: Rethinking Disability within the
21st Century, Disability Studies Quarterly, Vol 30, No 2.http://dx.doi.org/10.18061/dsq.v30i2.1247.
170
Doughty, K. (2004) Supporting independence: the emerging role of technology, Housing, Care &
Support 7(1), pp11–17. https://doi.org/10.1108/14608790200400004.
206

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.45 Local Authorities are starting to pick up on these opportunities. Working directly
with Amazon, Hampshire County Council has become the first local authority to
use new Amazon Echo technology to help older people live independently in
their homes for longer. It is providing 50 adult social care clients with a modified
version of the device to remind people when to take medication or check when
their carer is due to arrive. It will also connect to other technology in people’s
homes such as movement sensors, so it can remind people to have a drink
when they enter the kitchen.
16.46 Other Local Authorities are following suit. Norfolk have also started using
Amazon Echos, connected doorbells, sensors that tell if you have fallen, and
associated technologies and learning lessons from innovative approaches
elsewhere.
16.47 Geoff Connell, Norfolk’s head of information management and technology
said
171
:
“We’re now poised at a stage where it is about to go mainstream. We’re
looking at how we can learn lessons from places like Hampshire and
target self-funders to keep them out of the system and look at all of our
care packages to ask if they are suitable for a combination of tech and
people. We are aiming at the consumer tech, stuff that will integrate
easily and cheaply.”
16.48 Other “consumer tech” will allow you to remotely govern your heating, turn lights
on and off, and control most electrical devices using a mobile phone, a remote
control or even by voice commands. New switches are emerging that can also
control gas and water feeds which could be essential safety features for people
with a diagnosis of dementia or behaviours that challenge. The case study
below illustrates the impact of the creative use of existing technology.
171
Norfolk Council looks at Alexa for social care (Mar 2018) [online] http://www.ukauthority.com/UKA-
Local-Digital/entry/8023/norfolk-council-looks-at-alexa-for-social-care.
207
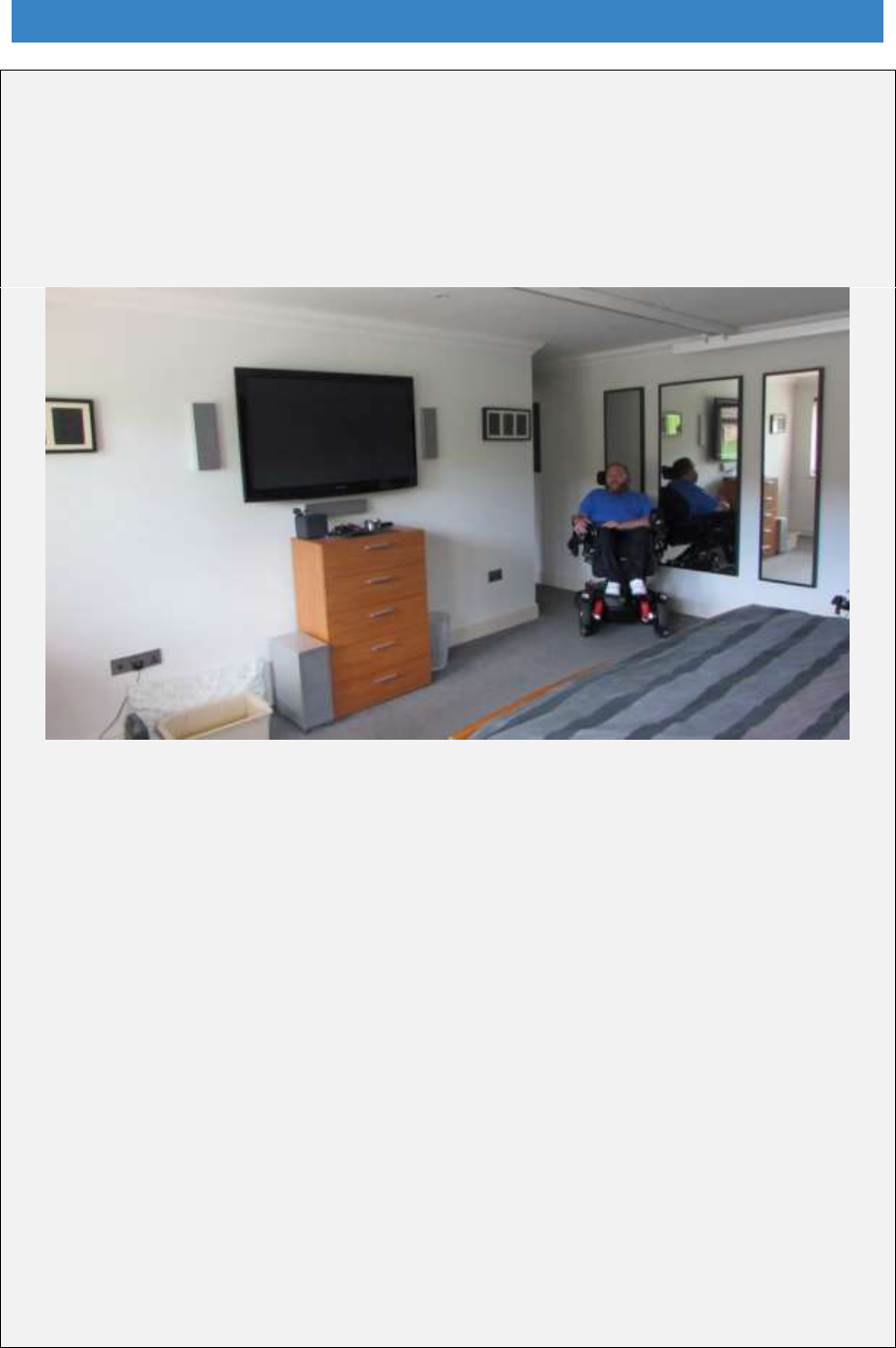
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
LightwaveRF Case Study
Ross Hovey’s mobile phone is his lifeline and in connecting LightwaveRF’s smart
home solutions he has transformed his home and way of life. A Liverpool football fan
and banking professional, he has a rare neuromuscular disorder, spinal muscular
atrophy – a genetic disease that causes muscle weakness and progressive loss of
movement. For 37 year-old Ross this means loss of strength in his arms and legs.
With support from his parents nearby, his specially designed wheelchair, a team of
dedicated carers and LightwaveRF smart home solutions, Ross lives independently in
his home in Cambridge.
How Ross uses Lightwave
“One of my friends recommended LightwaveRF and I have never looked back,”
reflects Ross. “It’s easy to install and not at all complicated. The retrofit is great.”
Ross says: “I sleep with my phone in my hand as it enables me to do everything – it is
my lifeline. The advent of smart phones has made tech easier to interconnect. I love
that I can control every LightwaveRF device from the free app. When I arrive home I
can turn on my outside light, open my front door and light my hallway all from my
phone. If I need to alert a carer in the middle of the night I can turn their bedroom lights
on at the touch of a button. My hallway has three PIR motion sensors. When a carer
gets up in the night to turn me, hall lights come on and go off again once they are back
in bed.”
Ross said: “I don’t endorse a specialist disabled world. The world should be normal
and accessible to everyone. The NHS advocate the Possum electrical assistive
technology, it dates back to the 1980s, is noisy, ugly, and powered by an impractical
PDA system. I didn’t want a special solution, I wanted stylish in my home which is why
I chose LightwaveRF. It is cool, modern, affordable, easy to use and non-intrusive.”
208

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Cognitive and dementia AT Case Study
16.49 There are a plethora of businesses providing consumer tech products and
services that can be utilised support independent and healthy living in old age.
It is predicted that over 130 million smart home devices were shipped in 2017,
and by 2020 the average home will have more than 500 connected devices,
ranging from washing machines to light bulbs
172
.
16.50 However, while the tech is generally quite easy and intuitive to use, it can still
be difficult to know what to buy and how to set it up. This is where handyperson
services are starting to develop expertise in providing and installing suitable
kit
173
.
Using the Data
16.51 As well as being easy to control remotely, this consumer tech also collects data
which can be sent for remote monitoring. This means that a smart home can
catch the ‘little things’ before they become major issues for the resident, and
ultimately a cost burden on the NHS. For example, increased toilet visits can
signal urinary infections or incontinence, deviations in gait over time can be the
precursor to an impending fall – all of which could, if left unchecked, result in
long stays in hospital for treatment. By detecting these signs early, the smart
home and its inbuilt technology can warn the resident or a doctor of an imminent
episode. With simple interventions such incidents could be mitigated or even
avoided.
16.52 Over the last 18 months Cascade3d have been using standard sensors to
monitor the stair usage of an 80-year old woman who had a hip replacement 10
years ago. They can track the number of times up and down per day, average
time, and the standard deviation for fastest/slowest. Further research is
required, but alongside listening to and being guided by clients’ wishes and
ensuring that clients understand the role of equipment and its relevance to their
needs, it could provide a diagnostic to identify when a stair-steady
174
or stairlift
should be considered.
16.53 In America, radar-based systems have been developed that are unobtrusive
but can measure body movement and vital signs at a distance, even through
walls, detecting falls and automatically raising an alarm. But their ability to
remotely sense heart rate and respiration rate (vital signs which can be
correlated with physical illnesses) means that this data can also be logged over
172
Johnson, C. (2016) The Future of Connected Home Health, Saffron Waldon: Plextec.
https://www.plextek.com/wp-content/uploads/2016/07/The-future-of-connected-home-health.pdf.
173
Coughlin, J. F. (2015) How the Internet of Things & On-Demand Services Will Change Housing in
Retirement [online] http://bigthink.com/disruptive-demographics/how-the-internet-of-things-on-
demand-services-will-change-housing-in-retirement.
174
https://stairsteady.net/
209

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
time and used to assess risk of falls, heart failure, Parkinson disease and
others
175
.
16.54 Another study has used radar sensors to monitor the gait speed of older people
as they move around their home
176
. A change in gait speed has a high
correlation with falls risk, and this system has an algorithm that can track
walking speed and alert a carer when the risk of a fall increases.
16.55 These systems show how non-intrusive and non-stigmatising systems can be
retrofitted to homes to allow people to live independently and safely.
User Acceptance
16.56 As society ages, more and more older people will be technologically savvy. A
recent survey of over 70’s by Silk Road
177
found that over 75% thought that
technology can make living in their home easier/better and prioritised
emergency response, enhanced alarms for visual and hearing impairment,
memory aids, medication assistance and video monitoring.
16.57 This suggests that the next generation of retirees will be redrawing Maslow’s
hierarchy of needs to include the new necessities of Wi-Fi and smart
technology
178
.
The Downsides
16.58 Most assistive tech makes it easier to perform tasks that a human would
otherwise do. A stairlift, for example, replaces the need to climb the stairs and
in doing so removes the inherent physical health benefits of the exercise.
Kaddour Bouazza-Marouf CEng FIMechE Mechatronics in Medicine
Loughborough University believes that user activity should be intrinsically
incorporated and encouraged within the living environment. He suggests that
when a stairlift is installed, the user would need to cycle using hands and/or feet
to move up or down the stairs. The stairlift will be electrically powered and uses
feedback from the cycling torque and speed of the user through a control
strategy; the restraining torque of cycling would be controlled to suit the ability
of the user.
175
Diraco, G., Leone, A., & Siciliano, P. (2017). A Radar-Based Smart Sensor for Unobtrusive Elderly
Monitoring in Ambient Assisted Living Applications. Biosensors, 7(4), 55.
https://doi.org/10.3390/bios7040055.
176
Phillips, C., Keller, J., Popescu, M., Skubic, M., Rantz, M., Cuddihy, P. and Yardibi, T. (2012).
Radar walk detection in the apartments of elderly. Conference proceedings of Annual International
Conference of the IEEE Engineering in Medicine and Biology Society.
https://doi.org/10.1109/EMBC.2012.6347327.
177
Silk Road (Jan 2018) Considerations when moving to a retirement style home [online]
http://www.wearesilkroad.com/pages/news/older_people.php?v3.
178
Coughlin, J. F. (2015) ibid.
210

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.59 There’s also the potential for technology to replace actual human interactions.
There’s significant research indicating that social isolation and loneliness have
a negative effect on health and wellbeing among older people, but contradictory
stories on the impact of technology. For example, research into internet use
and loneliness in older people
179
found that wellbeing increased where they
could get in touch with friends and family but decreased where they were trying
to make new friends.
Assistive Technology and the DFG
16.60 The UK Industrial Strategy
180
sets out Grand Challenges to put the UK at the
forefront of the industries of the future, ensuring that the UK takes advantage
of major global changes, improving people’s lives and the country’s productivity.
One of these Grand Challenges is the ageing society.
16.61 Most of the tech described here is relatively low cost – so unlikely to be part of
a DFG in isolation. However, one of the purposes of DFG is facilitating the use
by the disabled occupant of a source of power, light or heat by altering the
position of one or more means of access to or control of that source or by
providing additional means of control.
16.62 Routinely incorporating relatively low-cost consumer technology as part of a
DFG funded home modification would create significant potential for
widespread adoption, enhancing the UK’s potential to be a world leader in
assistive technology in accordance with the Industrial Strategy. It would also
improve the understanding of the benefits of these systems amongst social care
staff, including occupational therapists, with the potential to add further ancillary
sensors and devices in the future.
Support for people outside the DFG
16.63 There is a limited amount of information about what home improvement work is
done outside the DFG, but it appears to be substantial, with more people in
homes with downstairs toilets, showers instead of baths and full central heating.
But there is still unmet need, particularly in the older housing stock. In 2014/15,
9% of all households in England (around 1.9 million households) had one or
more people with a long-term limiting disability that required adaptations to their
179
Sum S, Mathews RM, Hughes I, Campbell A. (2008) Internet Use and Loneliness in Older Adults,
Cyberpsychol Behav. Apr;11(2):208-11. https://doi.org/10.1089/cpb.2007.0010.
180
HM Government (2017) UK Industrial Strategy: Building a Britain fit for the future.
https://www.gov.uk/government/publications/industrial-strategy-building-a-britain-fit-for-the-future.
211

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
home
181
. Most (81%) thought their homes were suitable for their needs and over
half of households (55%) that required adaptations in their home already had
them installed. However, around 45% of households lacked one or more of their
required adaptations.
16.64 Households with a person aged under 55 who had a long-term limiting disability
were more likely (32%) to state their accommodation was unsuitable than those
over 75 (12%). This demonstrates that services to help people with adaptations
should not be focussed solely on the old, but also on younger age groups. At
the moment these are the groups often excluded from the DFG because of the
failure to account for housing costs in the means test.
16.65 Health and social care are inevitably focussed on older people, as they are the
biggest users of services. There are some indications that people only go ahead
with adaptations after they had experienced a fall or other incident that made
them realise they were becoming less able to cope
182
. They may also be
deterred by the clinical appearance of adaptations
183
. As Part A of this review
indicated, they do not know where to turn for help.
16.66 An Age UK survey in 2015 indicated that about 1 in 5 people aged 60 to 69
were making adaptations to their homes to make them suitable for their needs
as they age
184
. Nearly a third of over-70s had made the changes to make caring
for a relative easier. However, a quarter of those interviewed said they would
only consider making changes if they had an accident that affected their
physical ability and a fifth would only think about adaptations if they were
advised by their GP. These findings suggest that people need more
encouragement to think ahead and ‘future-proof’ their homes before they get to
crisis point. It also indicates that GP surgeries could play a significant role in
getting people to think about planning their home and providing initial
signposting to advice services if these were available.
16.67 How attitudes are changing in the cohort in their 50s just entering later life is
difficult to judge. People who have cared for their parents in may be more aware
of the need to prepare their home for old age than previous generations. There
is a need to understand more about what people are already doing, how
effective that is, what holds them back and what might encourage them to do
more to ‘future-proof’ their homes. There is also a need to explore what is
happening with younger disabled people and what type of services they would
like to see.
181
Ministry of Housing, Communities and Local Government (2016) English Housing Survey:
Adaptations and Accessibility Report, 2014-15. Ibid.
182
Powell, et al. (Nov 2017) ibid.
183
Bailey, C., Hodgson, P., Aitken, D. and Wilson G. (July 2018) Primary research with practitioners
and people with lived experience – to understand the role of home adaptations in improving later life.
https://www.ageing-better.org.uk/sites/default/files/2018-07/Primary-research-with-practitioners.pdf.
184
Age UK survey 2015 http://www.ageuk.org.uk/latest-press/archive/1-in-5-older-people-adapting-
home-for-later-life/
212

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.68 Supporting people outside of the DFG relies on a number of factors:
Market provision
Good advice and information
Reliable tradespeople
Financial support
Market provision
16.69 The market for technical products is expanding rapidly, as the previous section
has shown. There is also considerable innovation in kitchen, bathroom and
stairlift design. There are a number of specialist suppliers, and inclusive design
is becoming more mainstream. Wet rooms are now aspirational and desirable
and found in retail showrooms. Adapted kitchens are also no longer solely the
preserve of specialists. Stairlifts are also getting sleeker and take up less space.
16.70 However, the problem is not the availability of age-friendly and inclusive
products, it is the lack of specialist sales staff able to advise disabled and older
people. Bathroom and kitchen showrooms tend to be male-dominated, sales-
driven spaces. Of those over 65, almost half of potential customers are single,
and a high proportion are women. Showrooms are not easy environments to
talk about disability needs or how to plan ahead for later life.
16.71 The sheer choice of products is bewildering and putting together a package for
a bathroom or kitchen that will suite individual needs is not easy, particularly
where room sizes are small or awkwardly shaped. Although there are plenty of
wet room designs, making sure the configuration is right for future needs,
finding easy to use controls, and making sure surfaces are non-slip is not
straightforward.
16.72 It is hard to know where to find reliable and knowledgeable information online
or to know where to turn for help. It is all too easy to be talked into buying the
wrong products. Most people will only have one opportunity to install a new
bathroom or kitchen and will not necessarily be able to afford to rectify what can
be costly mistakes.
16.73 At the top end of the market there are some innovative companies such as
Motionspot who are showing just how beautiful adapted bathrooms can be
185
.
There is also a lot that can be learnt from the design of hotel bathrooms. Hotel
chains are managing to put accessible bathrooms in relatively small spaces and
not only making them very attractive but also easy to clean and maintain.
16.74 Some mainstream retailers are becoming more aware of the need to cater more
effectively for this market. Bathstore has created an Easy Bathing range in
conjunction with specialist bathroom supplier AKW
186
. However, other retailers,
185
https://www.motionspot.co.uk/
186
https://www.bathstore.com/products/easybathing.
213

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
such as B&Q, have tried displaying inclusive bathroom products before but
eventually pulled out. It is still too early to tell whether the Bathstore initiative
will have a longer lifespan.
16.75 Better products and services will eventually emerge. Nesta estimates that the
spending power of the ‘silver economy’ in the UK will grow from £79 billion to
£127 billion by 2030
187
. At the moment, most general advertising spending is
aimed at younger age groups. There is little sophisticated market analysis of
the older demographic with the over 50s, or over 65s categorised as one age
group. There seems to be a perception that the older market segment is
unattractive and simply populated by low income people in poor health
188
.
However, the demographic bulge of the “Baby Boom” generation is now
entering their later years. They are more ethnically diverse, more educated,
more aware of design, used to doing up their homes, and familiar with searching
online and comparing ratings. They will eventually drive change, but it has not
happened yet.
The role of local authorities
16.76 At the consultation events participants were asked what role councils and
national government should play in helping people outside of the DFG or
whether it should be left to the market and personal responsibility:
1. Duty on councils - DFG duty should be extended to provide information,
advice and support to anyone with a substantial disability
2. Leave it to the market - if there is sufficient demand the market will
respond to provide appropriate services
3. National advice - advice and information is available from a national advice
centre (web/call centre)
4. Personal responsibility - We should leave people to do what they want in
their own homes.
16.77 There was reasonably strong support for councils to have a role in providing
information, advice and support (51%). A third of respondents also said there
should be some form of national advice website and/or call centre. Only 10%
said it was personal responsibility, and even fewer that it should be left solely
to the market (Figure 16.3)
187
https://www.businessgrowthhub.com/blogs/2017/05/profit-from-the-grey-pound.
188
http://www.ecipartners.com/news-and-insights/insights/the-grey-pound
214
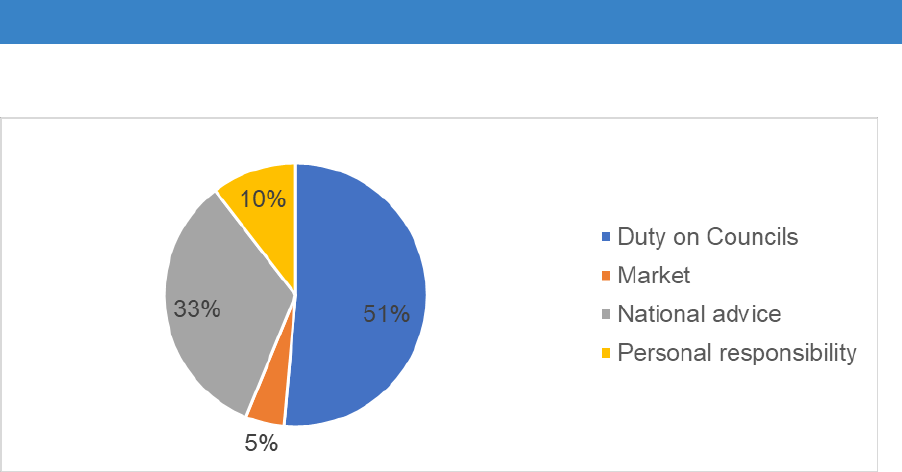
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 16.3 Options for support for people outside the DFG
Source: workshop responses
Where people go for information
16.78 The evidence suggests that there is a gap in terms of advice and information,
with the market not being able to provide it effectively, at least not at the present
time. However, local authorities are not the obvious alternative. In a small-scale
survey conducted for Care & Repair England respondents were asked where
they would turn for information about adaptations (Figures 16.4 and 16.5).
People renting would be most likely to go to their landlord, although social
housing tenants would be just as likely to go straight to the council. In
comparison, relatively few home owners or tenants in private renting would go
to the council.
16.79 Home owners (48%), private renters (23%) and people below retirement age
were more likely to say they didn’t know where to go than other groups. Home
owners were more likely than other groups to search the internet (46%) but this
was more commonly used by those aged 55-64, rather than older age groups.
A third (34%) of owners were as likely to go direct to a builder or advertised
home adaptations company as go to an HIA or an organisation like Age UK.
Few people in any tenure group who were under 75 said they would turn to
friends and family.
215
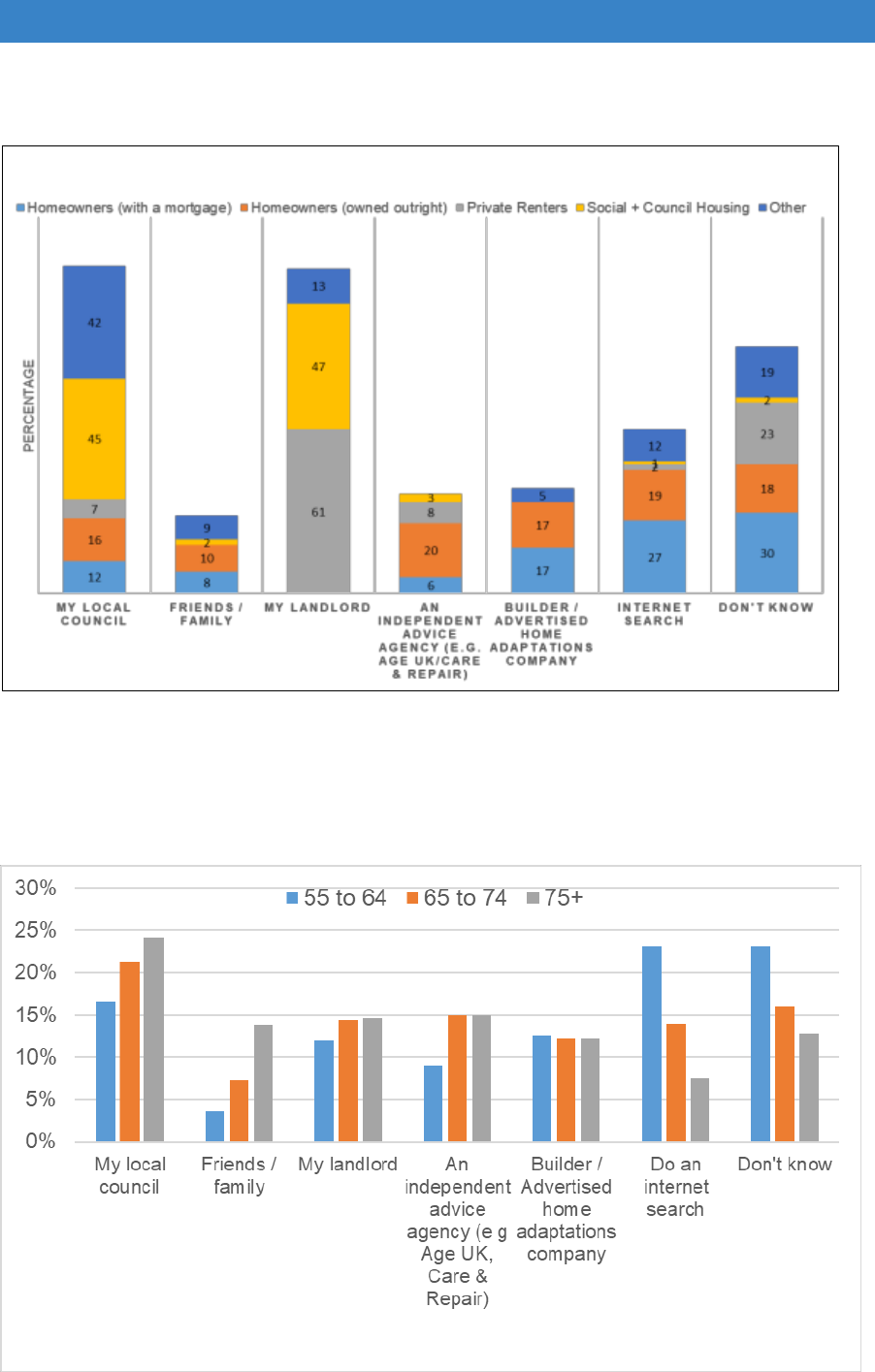
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 16.4 Where older people go for information by type of organisation and by
tenure
Source: BMG Survey for Care & Repair England, July 2017 (481 UK residents aged 55 and over)
Figure 16.5 Where people go for information by type of organisation and by age
Source: BMG Survey for Care & Repair England, July 2017 (481 UK residents aged 55 and over)
216
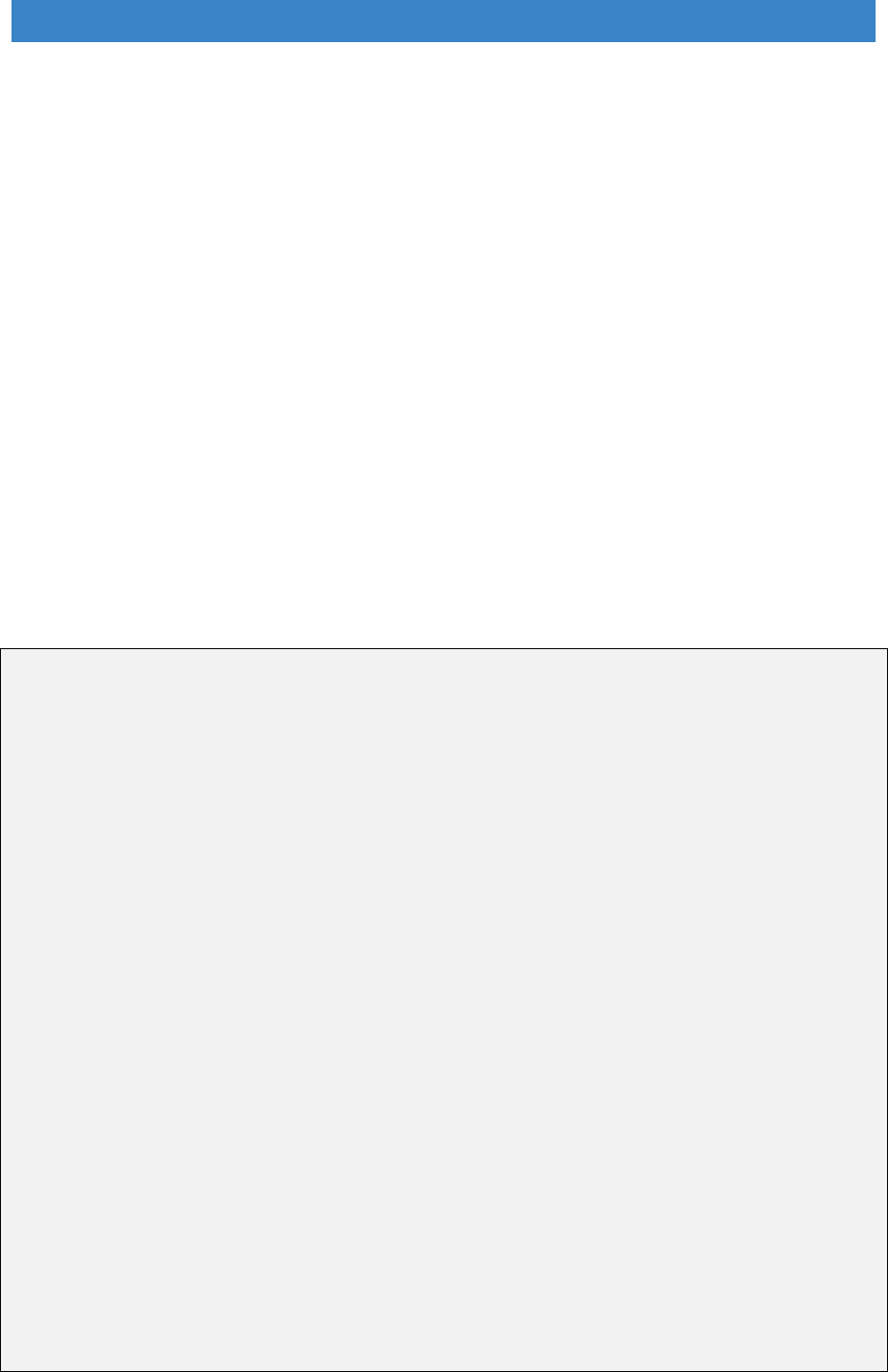
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.80 It is a key requirement of the 2014 Care Act to provide good quality information,
including housing advice. Areas which have retained a full home improvement
agency service are better equipped to provide advice and support to people
outside the DFG. However, some areas have lost this function as a result of
austerity measures and it needs to be restored as part of developing integrated
and holistic services. If councils are going to play a bigger role then some of the
ideas suggested earlier in this report, about having a more recognisable name
and branding for the service, also need to be implemented. It has to be about
‘investment’ not ‘welfare’ and be welcoming for all age groups.
16.81 There is also scope for some home improvement agencies and councils to use
their expertise in home adaptations to enter the commercial market as the
example of West of England Care & Repair demonstrates. However, it needs
to be delivered in a very different way from a traditional adaptations service. It
must be market-orientated, fast, efficient and offer attractive and aspirational
solutions. It needs to be delivered in a way that would be expected from a
mainstream market provider, but with the added advantage of a deep
understanding of people’s needs and expert adaptations advice.
West of England Care & Repair ‘Enterprises’ service
WE Care & Repair is a well-established home improvement agency operating
across: Bristol; Bath and North East Somerset; North Somerset; and
Gloucestershire.
Enterprises is their commercial arm. It provides a specialist design and installation
service for easy access bathrooms aimed at people who are not eligible for a DFG,
or who prefer to commission the work themselves. The service is designed to help
people maintain their quality of life and wellbeing, retain their independence and
reduce the risk of falls.
The service works alongside their contractual obligations to support people with
minor adaptations and repairs, home security, handyperson services, hospital
discharge and other more traditional home improvement agency services.
The development of the service was based on a thorough analysis of the local
market for bathroom adaptations and a detailed business plan. It builds on their track
record as a trusted local social enterprise. They offer assessment and support from
their own occupational therapist and end-to-end project management. The service
includes:
• Advice
• Design, visualisation, specification, quotation
• Site supervision and final inspection
• Installation of specialist equipment
• Warranty for building work
217
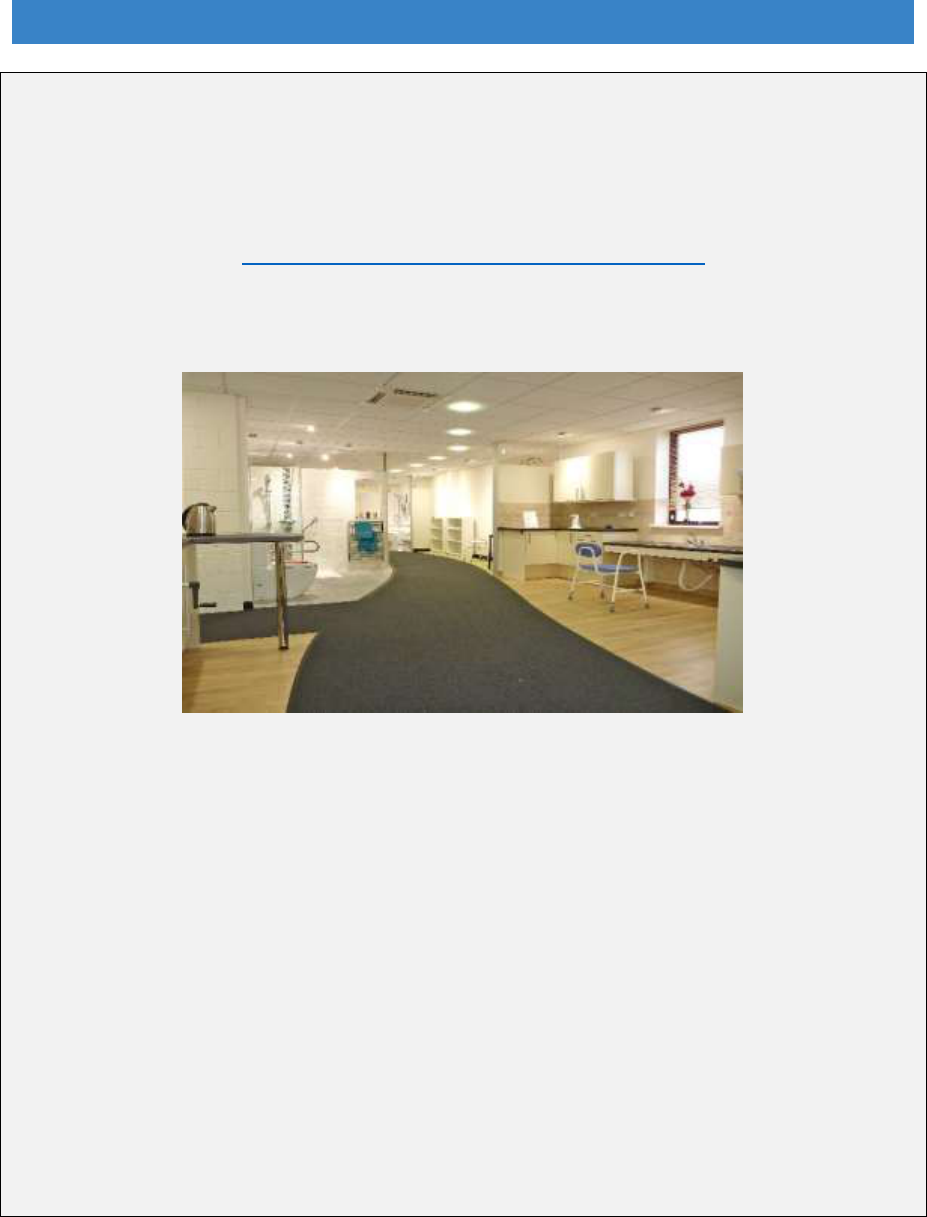
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
To build the service, they had to improve their networks and referral pathways,
provide support with financing, develop a different project management and
customer support role and work more effectively with the supply chain. There is
potential to develop the self-pay service to offer a wider mix of adaptation options.
A brochure is available in print and online which shows a range of design solutions at
different price points: http://www.wecr.org.uk/enterprisesbrochure.
The Home Independence Centre provides a showroom setting for people to view
and try aids and adaptations and have assessments.
Learning points:
• There is substantial opportunity for HIAs to operate more commercial models
• It requires development investment and a higher marketing overhead
• Risk to revenue/reputation if there is a lack of capacity to meet demand promptly
• Competition from the wider market may increase
• It is important to measure outcomes and impact to demonstrate results to
funders, future investors and commissioners.
As a not for profit organisation developing a commercial service helps:
Create profit to be reinvested in services for those on very low incomes
Delivers preventative services fast to reduce accidents in the home and pressure
on statutory services
Encourages people to take control of their future
Within WECR it helps drive efficiency in all other parts of their service
Paying for adaptations
Minor adaptations
16.82 Most of the adaptations required may be relatively low cost. The English
Housing Survey found that the four most common adaptations that households
said they needed were: hand rails inside (40%); a bath or shower seat or other
218

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
bathing aids (30%); a specialist toilet seat (25%); or a shower to replace a bath
(19%)
189
. However, the data needs to be treated with some caution as it is
based on self-assessment and lack of knowledge about different types of
equipment and adaptations may mean people are not always able to determine
what is needed. The evidence in Part A shows that minor adaptations are very
cost-effective and have a significant impact on falls and accidents.
16.83 There are two ways to deliver minor adaptations using market provision. One
is to use some of the new apps and online services to find people willing to do
small jobs, and the second, is to use local tradespeople. For these to be
effective requires accreditation, as was discussed above, and validated
customer rating systems.
16.84 There is an important role for a handyperson service run by a local authority or
home improvement agency. These are still the best way to provide a service to
people on low incomes. Handypersons are trained as trusted assessors and
can not only carry out the work requested but can spot if any other help is
required, so they are a very important preventative service. The 2018 CLG
Committee report recommended that these are made available in all local
authority areas
190
.
16.85 As a lot of people are not claiming all the benefits they are entitled to, making
sure that they get help from a home improvement agency caseworker or are
signposted to services such as Citizens Advice is also very important. If benefits
income is maximised, it would not only allow people to get minor adaptations,
but also to afford to heat their homes, improve their diet, take up hobbies and
go out, all of which improves health and wellbeing.
Major adaptations
16.86 Paying for more expensive work may be more problematic, particularly for
people who do not meet the DFG means test but have relatively limited
resources. This review has showed that a level access shower costs around
£5,000 but a self-funder is likely to have to pay more. The cost depends on local
building costs, the quality of the installation and the fact that private work will
probably be more expensive than prices negotiated as part of a DFG.
16.87 The English Housing Survey indicated that concerns about affordability appear
to be diminishing. Households that could not afford to install adaptations
decreased from 26% to 21% from 2011/12 to 2014/15. However, there has
been a long period of relatively stagnant wages and rising housing costs so
whether this remains the case is not clear. There are inevitably going to be
people in all areas who will struggle to fund basic bathroom improvements.
189
Ministry of Housing, Communities and Local Government (2016) English housing survey 2014 to
2015: adaptations and accessibility of homes report, ibid.
190
Communities and local Government Committee (Feb 2018) ibid.
219
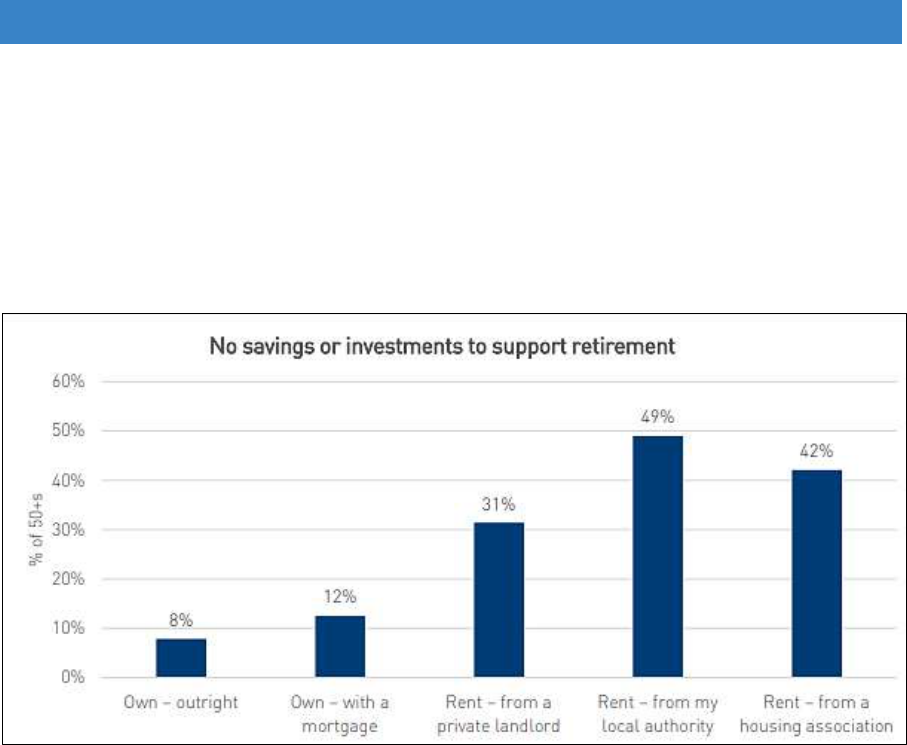
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
16.88 A YouGov survey by the National Housing Federation (NHF) in 2018 found that
8% of outright owners, 12% of those with a mortgage and 31% of those renting
privately aged 50+ had no savings or investment to support retirement (Figure
16.6). Proportions were even higher for those in the social rented sector, but
they might be more likely to get help from their landlord.
Figure 16.6 People 50+ with no savings or investment to support retirement
Source: NHF (2018) YouGov Omnibus Poll of 3936 adults aged 50+ in England
16.89 There are a number of options for people to obtain funding for major
adaptations:
Loans
Pension freedoms
Home equity
Lifetime mortgages
Local authority loans
16.90 Local authority loans are being used in some areas as part of RRO policies as
has been described in some of the case studies in this review. Loans are mostly
for larger jobs above the current £30,000 DFG threshold, but some are also
used for smaller jobs where work could not otherwise be carried out.
Repayment is made when the house is eventually sold. This is an important
source of funding for people unable to raise funds any other way.
220
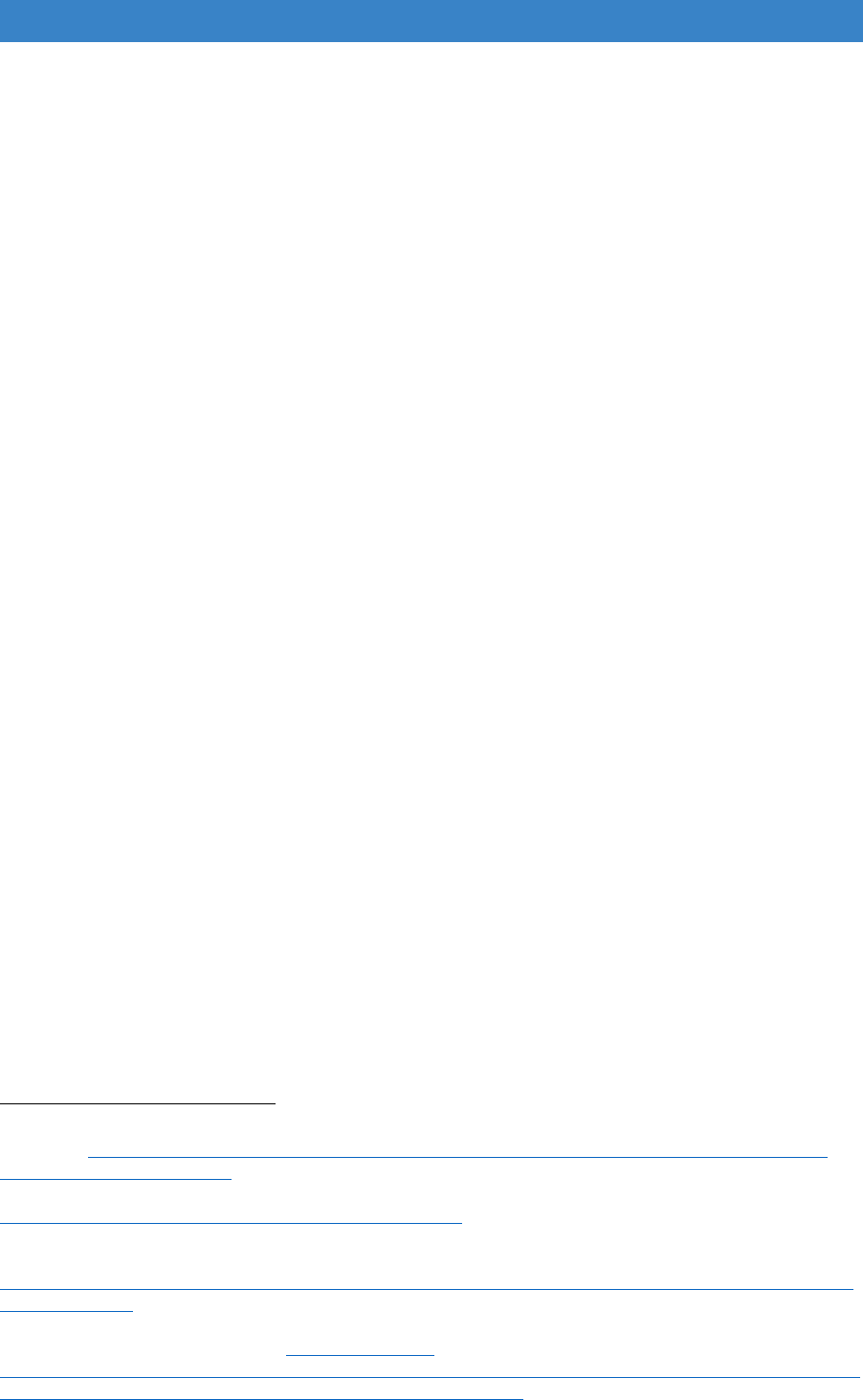
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Pension freedoms
16.91 People over the age of 55 now have greater freedom to withdraw lump sums
from their pension pots. Research shows that when this was introduced
700,000 people used those freedoms between October 2015 and December
2016. The majority transferred the money into another pension or bought an
annuity, but 28% took their 25% tax fee lump sum, and a further 15% took cash
in addition to the tax free lump sum, and 43% spent this money on home
improvements
191
. There is little detail of what improvements were carried out,
but it shows that people are wanting to invest in their homes as they approach
later life. There is some concern that pension drawdown will leave people with
insufficient funds to support themselves throughout later life, but people are
also working longer and may rely on their pension for a shorter period of time.
16.92 However, spending power will vary. The richest quarter of pensioners earn
three to four times more than the bottom quartile and more than one in seven
will retire with no pension other than what they get from the state
192
. Women in
particular have lower levels of pension savings and they predominate in the
oldest age groups.
Equity release
16.93 Using some form of equity release is another option. The BRE research into the
DFG in 2011 stated that “virtually all owner occupied households needing
adaptations have equity in their home that is estimated to be at least twice the
total costs of any adaptations required”
193
. With the continual rise in house
prices since 2011, the costs of adaptations may be a relatively small proportion
of equity. Figure 16.7 shows the average equity held by older households.
However, a disproportionate amount of housing wealth is held by households
in London and the South East, and lower proportions in the North East and
North West, which have higher rates of disability
194
.
191
Pension and Lifetime Savings Association (2017) Decumulation Decisions: Pension Freedom
Journeys. https://www.plsa.co.uk/Policy-and-Research/Document-library/Decumulation-decisions-
pension-freedoms-journeys.
192
Wallace, A., Rhodes, D. and Roth, F. (Feb 2018) Home owners and poverty, York: JRF.
https://www.jrf.org.uk/report/home-owners-and-poverty.
193
Building Research Establishment (2011) Disabled Facilities Grant allocation methodology and
means test: final report, London: DCLG.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/63
35/1850571.pdf.
194
National Housing Federation (2016) Can our homes pay for the care we need in older age? Asset
wealth and an ageing population. http://s3-eu-west-
1.amazonaws.com/pub.housing.org.uk/Can_our_homes_pay_for_the_care_we_need_in_older_age_-
_asset_wealth_and_an_ageing_population_PDF_for_web.pdf.
221
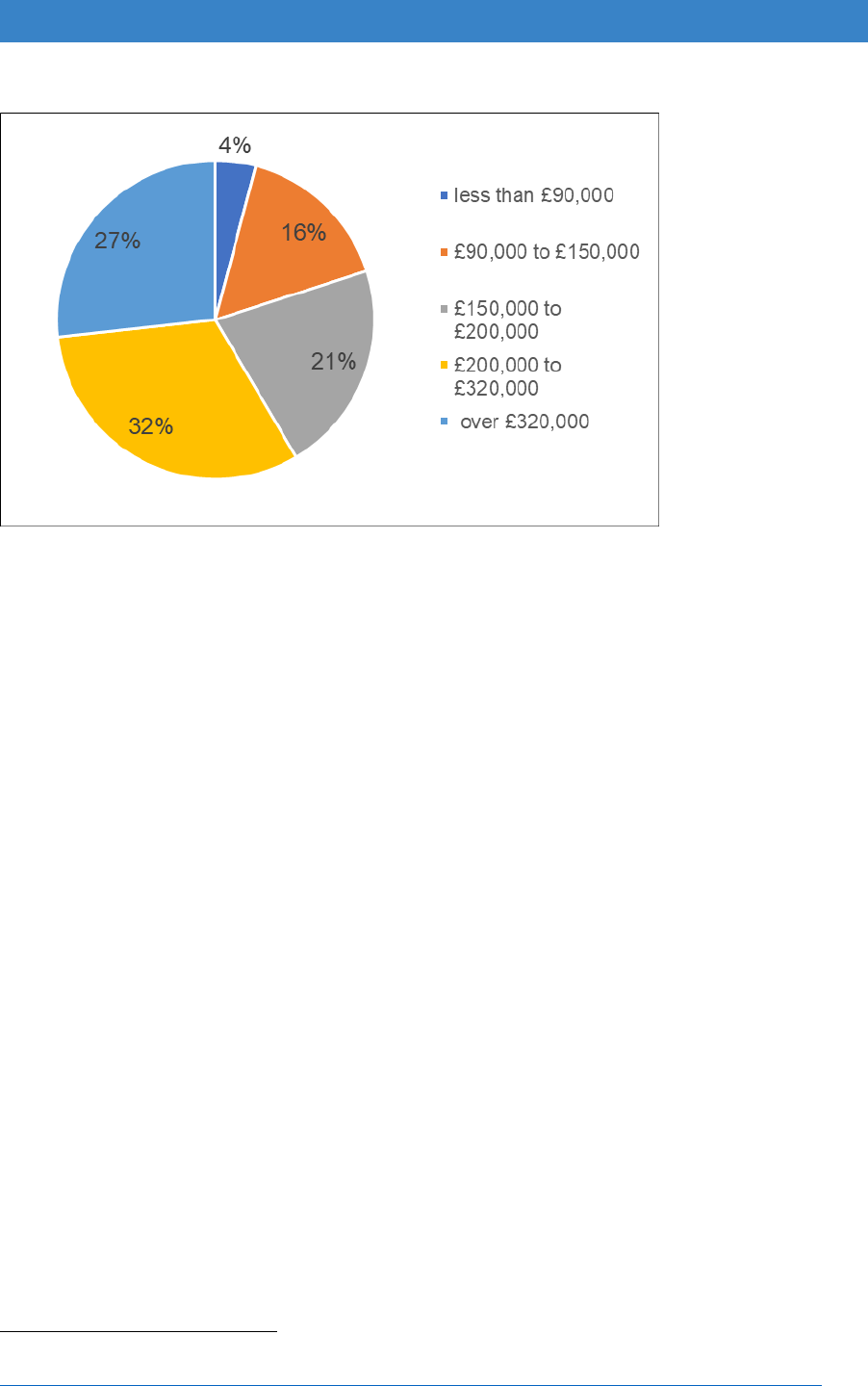
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 16.7 Housing equity held by home owners over 65 years, England 2014/15
Source: English Housing Survey – full interview survey.
Note: based on respondent valuation only
16.94 Equity release products used to have a bad name, but they seem to be
becoming more popular, with a greater variety of products, lower interest rates
and fewer penalties for making repayments. There are twice as many
customers as five years ago. Equity release is catching up with the use of
pension lump sums as a source of funding. In 2016, 38p of housing wealth was
released for every £1 of flexible payments from pensions, but this reached 56p
in Q4 2017. Single older women are an increasing part of this market
195
.
Lifetime mortgages
16.95 The lifetime mortgage market is also developing and becoming more accepted.
In the future, people may transfer directly from a residential to a lifetime
mortgage without ever owning 100% of their property or having a period when
they are mortgage-free
196
. This is particularly likely in the cohorts approaching
retirement who have experienced stagnant wages but still have substantial
mortgages. Interest-only mortgages may allow people to take lump sums.
Provided interest payments are maintained, there is no roll-up of the interest,
meaning it is only the capital that is repaid when the home is sold.
195
Equity Release Council (2018) Spring 2018 Market Report.
http://www.equityreleasecouncil.com/document-library/equity-release-market-report-spring-2018/.
196
Equity Release Council (2018) ibid.
222

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Incentivising home adaptations through the social care cap
16.96 There is potentially a lot of demand on equity, principally to pay care costs. It is
not an unlimited source of funding, particularly in some parts of the country
where house values are low. There is an argument for including spending on
adaptations as part of the social care cap, because removing hazards in the
home is likely to lead to fewer accidents and injuries, thus reducing costs for
health and social care. It would also help to raise awareness of the benefits of
preparing the home for later life or as an alternative to paying for domiciliary
care, reducing the likelihood of people reaching the care cap.
16.97 The previous Health and Social Care Secretary, Jeremy Hunt, in a speech
about the principles that will guide the Government’s thinking about the Social
Care Green paper, said a sustainable funding model for social care “will
specifically include looking at the role of housing, including how we can replicate
the very best models that combine a home environment with quality care and
how we can better support people through well-designed aids and
adaptations”
197
. Incentivising people through the social care cap might be one
way of delivering this support. Any parallel piece of work looking at social care
for working age adults also needs to address this issue
198
.
Summary – helping people outside the DFG
16.98 We don’t know enough about what people are doing to adapt their homes.
Home adaptations design is improving and there are some very good products
available from mainstream retailers. However, there is an information gap.
Local authorities and home improvements agencies could fill that gap, but they
need to become more visible and welcoming to people who are able to self-
fund. They need to ensure that they do not just focus on an older demographic
range, but appeal to younger disabled people, as this is the biggest group
requiring help with adaptations.
16.99 People with sufficient equity have more options if they wish to use the value of
their home to pay for improvements, but there are a lot of demands on that
equity. Incentivising adaptations through the social care cap seems a sensible
way forward.
16.100 People with low, or no equity and on low incomes have fewer choices.
Changes to the means test may mean more are eligible for the DFG, but there
will always be people who fall outside the criteria. Low cost handyperson
services provided by local authorities and home improvement agencies will still
be required and they need to be better known. They will also need access to
197
https://www.gov.uk/government/speeches/we-need-to-do-better-on-social-care.
198
House of Commons Library (Jan 2018) Social care: The forthcoming Green Paper on older people
(England), Briefing paper No 8002.
https://researchbriefings.parliament.uk/ResearchBriefing/Summary/CBP-8002.
223

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
good quality advice to ensure that limited resources are not wasted on
inappropriate adaptations.
Recommendations – developing a market
A further five-year funding programme for the DFG to improve certainty and
enable local authorities to invest in better procurement.
A national accreditation scheme for builders and tradespeople.
Use of an online schedule of rates to increase efficiencies and further work
to assess the effectiveness of framework agreements.
Flat-pack extensions to be used to provide a faster service with further
research to identify the best solutions.
A smart home starter kit as part of every DFG application.
Local authorities and home improvement agencies to provide advice,
information and handyperson services for people outside the DFG.
Further research on what people do outside the DFG to encourage more
‘future-proofing’.
Spending on adaptations outside of the DFG to be included as part of the
social care cap and considered in the Social Care Green Paper to incentivise
people to prepare their homes for later life.
224

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 17. Tenure and equality
“There are inequalities between tenures” “There is a void where policy on the funding
of housing association adaptations should be”
Heywood (2005)
199
17.1 Tenure issues were not in the brief and not explored in the consultation events
or online survey for this review. However, it is not possible to ignore tenure when
looking at the DFG. There are several issues that DHSC and MHCLG will need
to consider that may need a separate review. These include:
The high use of the DFG by registered providers relative to the size of this
part of the housing stock;
The decline in use by home owners despite the increase in numbers of older
people with disabilities;
The difficulties of providing DFGs for disabled people living in the private
rented sector who are some of the worst housed
Whether adaptations in the council stock should continue to be provided
through the HRA or brought into the DFG.
17.2 This chapter also addresses adaptations to the common parts of residential
properties such as entranceways, hallways, stairwells and emergency exits.
These are usually in rented or leasehold properties. Following a report by the
House of Lords Select Committee on the Equality Act 2010 and Disability, the
Government has made a commitment to review the remaining provisions of
Section 36 of the Act. The final section of this chapter looks at the potential
impact on the DFG if disabled people request improvements to the accessibility
of the common parts of their homes.
Inequality of access to the DFG by tenure
17.3 As Part A demonstrated, there appears to be inequality of access to the DFG. A
third of grants (34%) go to registered provider tenants when there are similar
numbers of people with long-term illness and impairments in the private rented
sector who may be in much poorer housing conditions (Figure 17.1). People in
the private rented sector only get 8% of DFGs. There may also be low income
home owners missing out on help because their needs are hidden, and few know
about the DFG. Registered providers tenants have a much clearer path to get
help with adaptations as their landlords will direct them to the council.
17.4 Lack of effective studies at local level mean that it is hard to know the latent
demand for adaptations and how this is distributed by tenure. Registered
provider usage may reflect the true demand for adaptations. Rather than
199
Heywood, F.et al. (2005), p.6- 7, ibid.
225
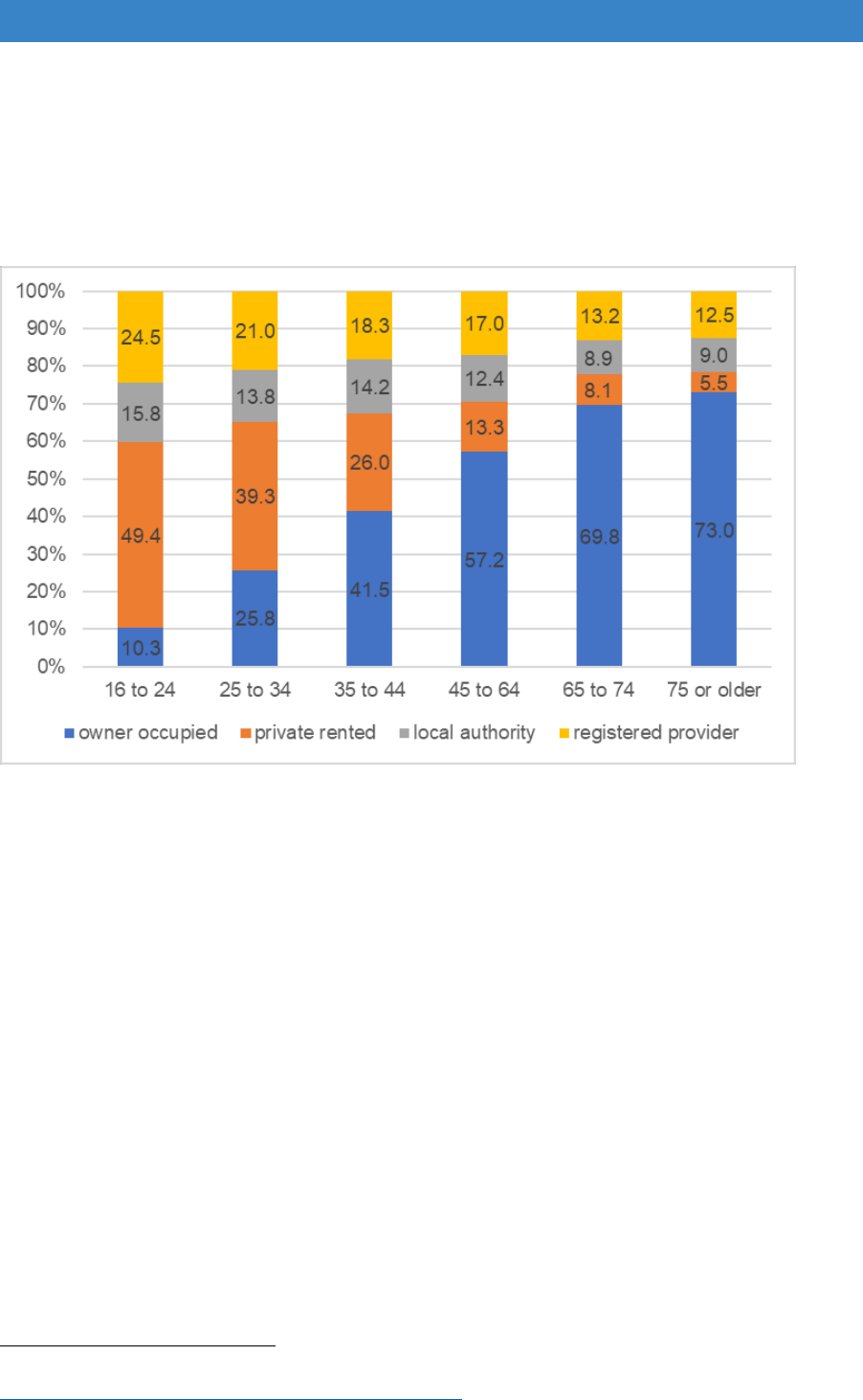
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
restricting access for registered provider tenants, ways need to be found to help
more people in the other tenures who are missing out on assistance.
Figure 17.1 Distribution of households with a long-term limiting illness by age of HRP
and tenure
Source: English Housing Survey 2014-15, full household sample
Home owners
17.5 It is often assumed that home owners are wealthier than tenants, but there is
still a considerable need for the DFG for people in this tenure. Overall rates of
relative poverty are lower for home owners than other tenures, particularly when
housing costs are taken into account (Figure 17.2) but looking at those with a
long-term illness or disability, home owners are just as likely to be in relative
poverty as people in social renting (Figure 17.3)
200
.
200
Wallace, A., Rhodes, D. and Roth, F. (Feb 2018) Home owners and poverty, York: JRF.
https://www.jrf.org.uk/report/home-owners-and-poverty.
226
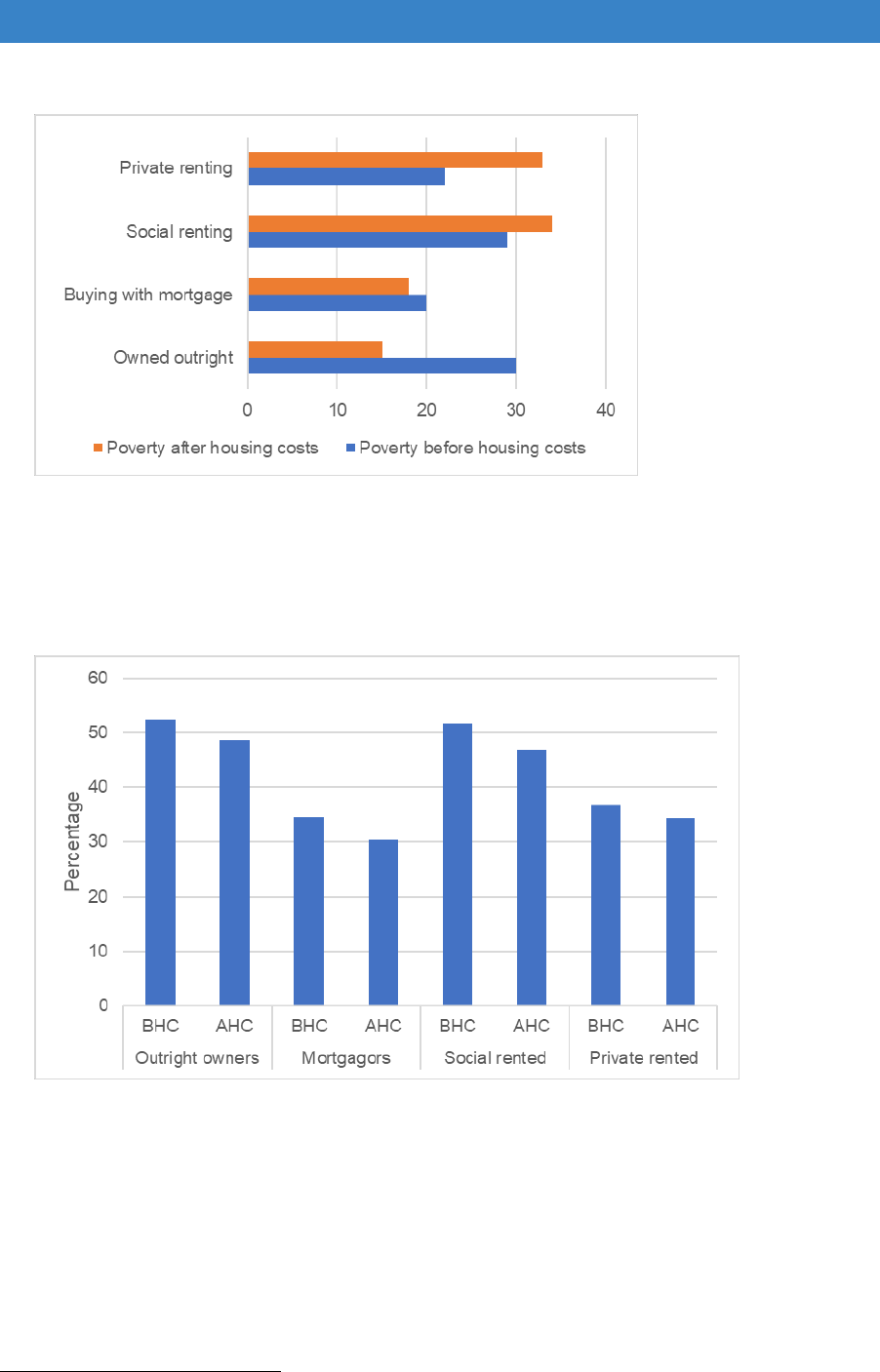
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 17.2 Relative poverty by tenure 2013/14
Source: Wallace, A., Rhodes, D. and Roth, F. (Feb 2018). Note: figures for United Kingdom.
Poverty defined as below 60% of median equivalised income.
Figure 17.3 Households with long standing illness or disability by poverty status
and tenure 2014
Source: Wallace, A., Rhodes, D. and Roth, F. (Feb 2018), Table 13.
Note: figures for United Kingdom. Poverty defined as below 60% of median equivalised income.
17.6 Most people over 65 live in pre-1980 properties not built to current accessibility
standards. Category 1 hazards, which include excess cold and risks from falls,
affect 13-14% of homes occupied by older people
201
. The homes of older home-
owners in relative poverty (before housing costs) require significant investment
(£2 billion) to bring them up to the Decent Homes Standard
202
. The amounts
201
Ministry of Housing, Communities and Local Government (2016b) ibid.
202
Wallace et al. (2018) ibid.
227

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
needed per property are only a small proportion of the level of housing equity,
however, equity varies both within and between regions and is not always easy
to tap into, as was discussed in the previous chapter. Home owners therefore
need continued access to the DFG and need to be made aware that this help is
available.
Registered providers
17.7 Guidance from 2008 states that it is expected that registered providers
contribute to the costs of adaptations in their own properties, but this ‘needs to
be negotiated and established through formal agreement’
203
,
204
. The diverse
nature of this sector makes it difficult to develop effective partnership
agreements as it ranges from national organisations with 50,000 properties
which operate across many authorities, to local organisations with less than 100
homes.
17.8 Where there are local adaptation agreements, some of the costs of work to
registered provider properties may be claimed back by local authorities, either
after work has been completed, or at the end of the financial year. Payments
from housing associations or transfer organisations are not included as a
separate item in LOGASnet returns so it is difficult to know how much gets
returned.
17.9 Local funding agreements appear to have become less common, as registered
providers have been dealing with uncertainty about income levels due to a 1%
cut in rents, a cap on housing benefit and the loss of direct rent payments due
to the transfer of tenants to Universal Credit. Contributions are therefore likely
to have reduced.
17.10 Major repairs expenditure has fallen by 11.3% from £524.5m in 2015/16 to
£465.5m in 2016/17 among the top 100 registered providers
205
. One provider
in its annual report said: “The budget decreases were achieved by reducing
planned expenditure on boundary works and environmental programmes,
disabled adaptations, external wall insulation and slowing down expenditure
on various planned maintenance schemes where lifetimes of components may
203
Heywood, F. and Mackintosh, S. (2008) Housing Associations and Home Adaptations: Making it
Work Smoothly, London: Habinteg.
https://www.habinteg.org.uk/download.cfm?doc=docm93jijm4n432.pdf&ver=519.
204
Wilson, W. and Fears, C. (Dec 2016) ibid.
205
Hilditch, M. (May 2018) Repairs and maintenance spend tracker: what did your association do in
2016/17? Inside Housing Insight. https://www.insidehousing.co.uk/insight/repairs-and-maintenance-
spend-tracker-what-did-your-association-do-in-201617-
56310?utm_source=Ocean%20Media%20Group&utm_medium=email&utm_campaign=9493587_IH-
THE-FRIDAY-LONG-READ-18-5-2018-GR&dm_i=1HH2,5NHAR,L7J0AM,LZEN1,1
228
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
be extended without breaking Decent Homes requirements”
206
(bold type added
for the purposes of this report).
17.11 Adaptation agreements do not just deal with the payment for adaptations. They
also help with the flow of information about the needs of disabled and older
people in the locality, the type of new adapted homes required, and ensure that
home choice and transfer systems work effectively for disabled people. This
helps people relocate if they are in homes that are unsuitable for adaptation.
Adaptation agreements therefore need to be a key part of the DFG process.
17.12 Registered providers are increasingly developing agreements with health
207
.
Some have hospital discharge schemes or do preventative work with tenants,
such as identifying those with dementia or working to combat loneliness
208
.
Some are doing more to support vulnerable people with their tenancies,
particularly as Universal Credit is introduced. Some also have very good
development policies and are trying to build as many accessible homes as
possible. But home adaptation issues seldom appear on the agenda because
cases are passed to local authorities for the DFG
209
.
17.13 The situation is further complicated by the changing designation of registered
providers. They are sometimes considered public bodies, such as in 2016 when
the ONS said their borrowing was on the Government balance sheet, but in
2017 they were again deemed to be private organisations
210
. Many are
becoming much more commercial and market-driven.
17.14 Local authorities can often get agreements with local registered provider
landlords but find it hard to get the big regional and national and organisations
round the table. It is unrealistic to expect organisations working across
numerous authorities to sign up to different agreements in each area. In order
to make agreements work, they need to be standardised.
17.15 The London Housing Strategy says that “The Mayor will work with councils and
housing associations to agree a protocol to ensure that housing associations
206
Thirteen Group Annual Report 2016/17 (2017) [online]
https://www.thirteengroup.co.uk/uploaded/thirteen/files/Thirteen%20Financial%20Annual%20Report%
2016-17.pdf
207
Buck, D., Simpson M. and Ross S. (2016) The economics of housing and health: The role of
housing associations, London: Kings Fund.
https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Economics_housing_and_he
alth_Kings_Fund_Sep_2016.pdf.
208
Andrews, J. and Molyneux, P. (2013) Dementia: Finding housing solutions, London: National
Housing Federation. https://www.housing.org.uk/resource-library/browse/dementia-finding-housing-
solutions/
209
Mackintosh, S. and Heywood, F. (2015) The Structural Neglect of Disabled Housing Association
Tenants in England: Politics, Economics and Discourse, Housing Studies, 30:5, 770-791,
https://doi.org/10.1080/02673037.2015.1044947.
210
https://www.ons.gov.uk/news/statementsandletters/statementonclassificationofenglishhousingassoc
iationsnovember2017.
229

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
contribute to the cost of adaptations”
211
. But local agreements take a long time
to develop. A national agreement would be a better solution, but there needs to
be more research about how this might be developed.
Council stock
17.16 The council stock has not been looked at in any detail in this report since
adaptations in this stock sit outside the DFG. The 2005 review recommended
a single funding pot covering all tenures. We are unable to make any
recommendations without doing further work to look in more detail at Housing
Revenue Account funding and whether this is working effectively. Council
landlords are under the same pressures as registered providers due to rent cuts
and welfare reform. How this has affected adaptation budgets is unknown. The
same teams often deliver both the DFG and council stock adaptations. It might
make sense to bring it all into one funding pot, but it needs further research.
Social housing generally
17.17 Further research is required across the social housing sector to see if access
to adaptation services are tenure-neutral. Anecdotal evidence presented to the
review team indicates that social housing tenants are sometimes given little
choice about adapting or moving. If they are under-occupying, or in a ‘general
needs’ property, they may be expected to move. This may be a good solution
for some younger people, but it is unknown whether this is also used for the
very old, those with dementia, or people with learning difficulties. It is also
unknown how much support people get and the effect a move has on those
tenants.
17.18 Only 22% of local authorities have an accessible housing register and some
home choice and home swap systems are not very good at recording adapted
and accessible homes or matching disabled people to suitable properties
212
.
Some landlords are better than others at giving adequate time to view
properties and make decisions, and not penalising people for turning down
properties that are not suitable. Co-production techniques should be used to
involve disabled tenants in changes to the system.
17.19 Heywood said in the 2005 review “there are no rewards for good housing
association policies”
213
. Perhaps there should be an annual award to give
adaptations and accessible housing policies in social housing greater
211
Greater London Authority (May 2018) London Housing Strategy, Section 5.39, p. 145.
https://www.london.gov.uk/sites/default/files/2018_lhs_london_housing_strategy.pdf.
212
Adams, L., Morris, S., Thomson, D., Rossiter, H., Felton, J., Newbold P. and Hazel, Z. (May 2018)
Housing and disabled people: the role of local authorities, London: EHRC.
https://www.equalityhumanrights.com/en/publication-download/housing-and-disabled-people-role-
local-authorities
213
Heywood, F., et al. (2005) ibid.
230
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
prominence. The Equalities and Human Rights Commission might be interested
in taking this forward following their report on housing for disabled people
214
.
Private rented sector
17.20 Figures from Part A show that the number of disabled people in the private
rented sector is increasing. Couples with children are now the most common
household type in this sector and half a million (510,000) children live in
privately rented homes that are unsafe. One in three disabled people in private
renting feel their home is not suitable for their needs. However, tenants may be
reluctant to come forward to get adaptations if their tenancy is insecure. We
also know that permission to adapt the property is refused in 10% of cases.
17.21 There is an urgent need for longer and more secure tenancies. The DFG
currently requires a tenant to state that they will remain in the property for five
years, when the average length of a tenancy is usually much shorter. There
may also need to be discussions with mortgage providers as some buy-to-let
mortgages specify a 12-month maximum tenancy
215
.
17.22 In a survey of 2,517 private landlords across the UK, 93% owned fewer than 5
properties, although the other 7% accounted for 38% of the stock. Dealing with
so many small landlords makes it very difficult for local authorities to have much
control over this sector
216
. The Homes (Fitness for Human Habitation and
Liability for Housing Standards) Bill 2017–19, may help to resolve some the
worst house condition problems for tenants.
17.23 There is potential for local authority licensing of private landlords to include
clauses about allowing permission for adaptations. However, authorities will
also need active strategies to deal effectively with landlords if they refuse
permission.
17.24 The CLG committee report on Housing for Older People recommend that
discretionary grants are given to private landlords for the costs of reinstatement
or removal of adaptations once a tenancy ends
217
. An alternative approach
would be to improve the design of modification solutions to encourage more
landlords to allow adaptations that do not need removal.
17.25 Housing and Health Partnership Boards could play an important role in co-
ordinating a local approach to private landlords. It would also provide a way to
rehouse people into the social housing sector where a privately rented home
would be difficult to adapt or is in poor condition.
214
Equalities and Human Rights Commission (May 2018) ibid.
215
Equalities and Human Rights Commission (May 2018) ibid.
216
Council of Mortgage Lenders (Dec 2016) The Profile of UK private landlords.
file:///C:/Users/white/Downloads/the-profile-of-uk-private-landlords-08.05.17%20(1).pdf.
217
Communities and local Government Committee (Feb 2018) ibid.
231
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
17.26 Foundations has a good practice guide on adaptations in the private rented
sector which could be updated to provide local authorities with ideas about how
to deal with this sector
218
. However, without central government legislation to
give tenants better security of tenure and prevent ‘retaliatory eviction’, it is
difficult to see how some of the issues relating to adaptations in this sector will
be resolved.
Adaptations without delay
17.27 The Royal College of Occupational Therapists publication ‘Minor Adaptations
Without Delay’
219
provided guidance to landlords about minor adaptations. This
publication aimed to reduce unnecessary referrals to occupational therapy
teams and provide tenants with a quick pathway to adaptations. The publication
is currently being revised and updated and needs to be made widely available
to all landlords
220
.
Common parts grants and the Equality Act
DFG for adaptations to communal areas
17.28 Following a report by the House of Lords Select Committee on the Equality Act
2010 and Disability, Government has made a commitment to review the
remaining provisions of Section 36 of the Act. These provisions would enable
disabled people to request disability related adaptations to the common parts
of residential properties such as entranceways, hallways, stairwells and
emergency exits to improve the accessibility of their homes.
17.29 As well as improving the quality of life for people with disabilities, adaptations
to common parts have the potential to reduce care costs and NHS expenditure,
through fewer hospital admissions from falls, less bed blocking and/or use
residential care. Inaccessible common areas can leave a disabled person
isolated within their home.
17.30 As stated in the Government response to the Women and Equalities Committee
inquiry into disability and the built environment
221
,
218
Foundations (2016b) Supporting people in private rented sector housing: A good practice guide,
Glossop: Foundations. http://www.foundations.uk.com/media/4441/prs-good-practice-guide.pdf.
219
Royal College of Occupational Therapists (2006) Minor Adaptations without Delay [online]
https://www.rcot.co.uk/practice-resources/rcot-publications/downloads/minor-adaptations-without-
delay.
220
Royal College of Occupational Therapists (in press) ibid.
221
Minister for Women and Equalities (2016) Government Response to the House of Lords Select
Committee Report on The Equality Act 2010: The impact on disabled people, London: HMSO.
232

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
“The Government Equalities Office, Ministry of Housing, Communities
and Local Government and the Department of Health and Social Care
have been closely engaged on this review. In light of this work,
Government intends to commence Section 36, subject to Parliamentary
passage of any regulations, should these prove necessary. Further work
on identifying and assessing any additional burdens on local authorities
is first required, after which an announcement on timing of the
commencement will be made”.
17.31 This review of the DFG is, therefore, required to consider how the future
commencement of Section 36 of the Equality Act could impact on DFG demand
and potential funding requirements.
17.32 The Impact Assessment on the Equality Act 2010 (Annex H)
222
estimates that
there would be increased demand for DFGs to carry out adjustments to
commons parts resulting in around 8,000 being paid at an annual cost of up to
£27m. It also estimates that half of the 57,000 disabled people it cites as facing
difficulties because of inaccessible common parts (29,000 people), will make
adjustments in the first year following the legislative change. This assumption
is based on 50% awareness of disability legislation among disabled people.
17.33 Regrettably, there is little available data that can help inform this aspect of the
DFG review. The following analysis mainly uses English Housing Survey (EHS)
data to provide contextual information regarding the potential demand for DFGs
in common parts and broad estimates of ‘worst case scenario’ potential
costs
223
. It also uses data provided through FOI requests to local authorities to
provide further information.
17.34 Of the 210 local authorities who responded to the FOI request, 193 had not
approved any DFGs to common parts in the 2016-17 financial year. Of those
17 local authorities that had, 11 had approved one DFG, while one local
authority had approved nine such applications (Table 17.1).
https://www.parliament.uk/documents/lords-committees/equality-act/Govt-Response-to-HoL-SC-
Report-on-the-EA2010.pdf.
222
Equality Bill Impact Assessment Version 3 (House of Commons Report Stage) (2009)
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/24
3602/9780108508677.pdf
223
The analysis uses 2014 and 2015 EHS datasets which provide a reference point of April 2015.
233
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 17.1: DFGs to common parts, 2016-17
Count of Common Parts
Applications
Number of local
authorities
0
193
1
11
2
0
3
1
4
3
5
1
6
0
7
0
8
0
Source: Foundations FOI request 2018
17.35 The EHS
224
collects information about whether flats have any common parts
such as shared entrances, lifts, corridors or staircases. It also records whether
flats have any shared facilities such as parking, as well as recording the
accessibility from the pavement to the main entrance used to access the flat.
17.36 The EHS estimates that there are around 4.7 million flats in England; 3.5 million
of these have common parts and 4 million have shared facilities. Table 17.2
and Table 17.3 show the regional distribution of flats with common parts and
shared facilities respectively. Not surprisingly, flats with common parts and/or
shared facilities are most commonly located in London.
Table 17.2: Flats with common parts by region, 2015
Frequency
(000s)
Percentage
distribution
North East
88
2.5
North West
318
9.0
Yorkshire and the Humber
200
5.7
East Midlands
129
3.7
West Midlands
222
6.3
East
329
9.3
London
1,370
38.8
South East
575
16.3
South West
304
8.6
Total
3,533
100.0
Source: English Housing Survey, 2015
224
The EHS is unable to provide analysis for dwellings and households at local authority level due to
sample sizes.
234

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 17.3: Flats with shared facilities by region, 2015
Frequency
(000s)
Percentage
distribution
North East
143
3.6
North West
443
11.2
Yorkshire and the Humber
282
7.1
East Midlands
169
4.3
West Midlands
298
7.5
East
350
8.8
London
1,301
32.9
South East
652
16.5
South West
320
8.1
Total
3,958
100.0
Source: English Housing Survey, 2015
17.37 As highlighted in the previous research into predicting need for DFG in common
areas
225
only very limited EHS data is collected that might indicate whether
households with disabilities who live in flats might require adaptations to these
areas or facilities. The indicators are:
Whether there is level access, and if not, whether it is possible to provide a
ramp.
Whether lifts are present and whether these are large enough to
accommodate a wheelchair.
The assessment of whether there are significantly higher than average risks
of harm from falls in common areas. This is the best proxy indicator of
whether the stairs are particularly steep or dangerous, or where corridors
have uneven surfaces/trip steps etc.
Level access in flats with shared facilities
17.38 Where applicable, the EHS records the number of steps from the pavement to
the main entrance used to access the flat. If steps are present, the survey
indicates whether there is space for a permanent ramp of 1:20 or shallower to
be installed. It is therefore possible to provide estimates of dwellings which
already have level access and those where a ramp could be installed relatively
easily.
17.39 Almost half (48%, 1.9 million) of flats with shared facilities already have level
access and it would be possible to provide this for a further 33% (1.3 million) of
225
Building Research Establishment (2011) Disabled Facilities Grant allocation methodology and
means test: final report, London: DCLG.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/63
35/1850571.pdf.
235
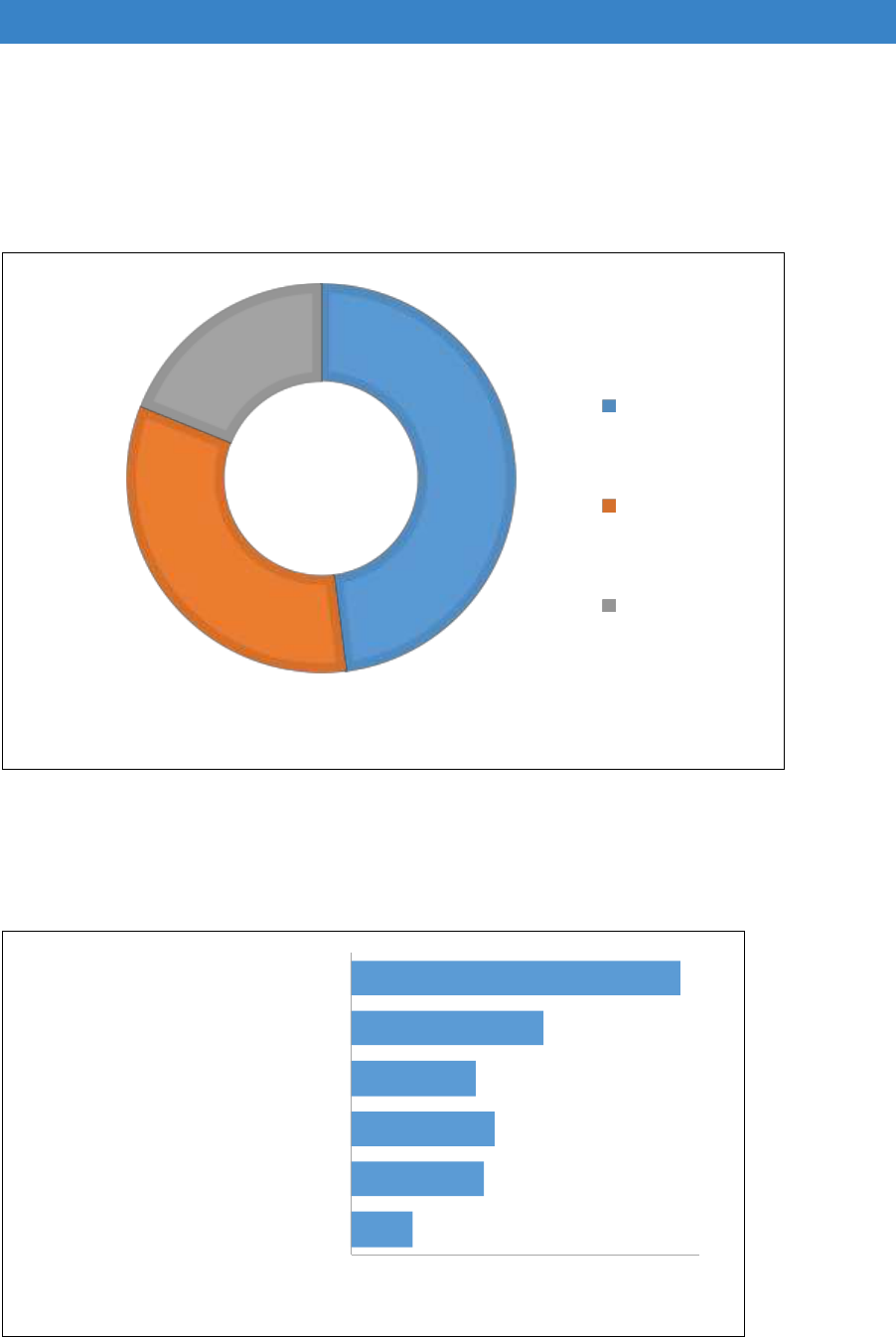
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
these homes by installing a straight ramp (Figures 17.4 and 17.5). This leaves
around 19% (749,000) of these flats where providing level access would be
more problematic, prohibitively expensive or simply not feasible.
Figure 17.4: Accessibility of flats with shared facilities, 2015
1,899
48%
1,311
33%
749,
19%
has level
access
could fit ramp
no level
access and
cannot fit
ramp
Note: dwelling numbers are thousands of dwellings
Source: English Housing Survey, 2015
Figure 17.5: Accessibility of flats, by flat level, with shared facilities, 2015
247
535
577
502
775
1,322
0 200 400 600 800 1,000 1,200 1,400
ground floor flat no level access and
cannot fit ramp
ground floor flat could fit ramp
ground floor flat has level access
upper/basement flat no level access and
cannot fit ramp
upper/basement flat could fit ramp
upper/basement flat has level access
number of flats (000s) with shared facilities
Source: English Housing Survey, 2015
236
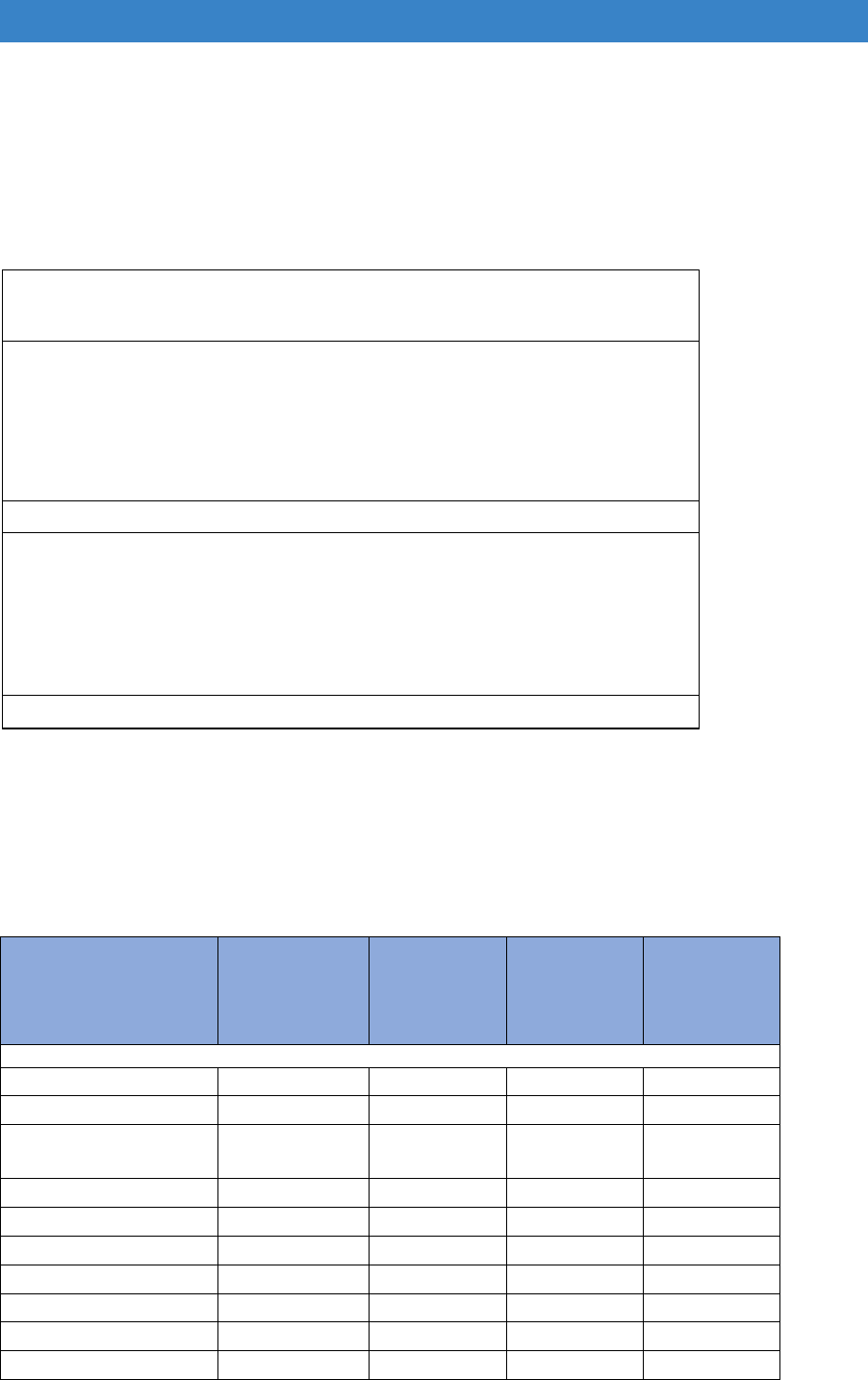
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
17.40 The presence of level access and the ability to create it varies by tenure (Table
17.4). Private sector homes, especially those in the private rented sector, are
less likely to already have level access. Registered provider homes are
generally easier to adapt.
Table 17.4: Accessibility of flats with shared facilities by tenure, 2015
no level access and cannot
fit ramp
could fit
ramp
has level
access
all dwellings
thousands of dwellings
owner occupied
213 286 460 959
private rented
308 570 546 1424
local authority
93 211 355 659
registered provider
134 244 537 916
all dwellings
749 1311 1899 3958
percentage of dwellings
owner occupied
22.2 29.8 48.0 100.0
private rented
21.6 40.0 38.4 100.0
local authority
14.2 32.0 53.8 100.0
registered provider
14.7 26.6 58.7 100.0
all dwellings
18.9 33.1 48.0 100.0
Source: English Housing Survey, 2015
17.41 There are also likely regional variations (Table 17.5 and Table 17.6), although
the findings should be regarded as indicative only due to small sample sizes for
some regions.
Table 17.5: Accessibility of flats with shared facilities by region, 2015
No level
access and
cannot fit
ramp
Could fit
ramp
Has level
access
All flats
with
shared
facilities
thousands of dwellings
North East
38
51
54
143
North West
66
186
191
443
Yorkshire and the
Humber
65
92
125
282
East Midlands
23
60
86
169
West Midlands
56
121
121
298
East
49
131
170
350
London
271
318
712
1,301
South East
116
270
267
652
South West
66
81
173
320
Total
749
1,311
1,899
3,958
Source: English Housing Survey, 2015
237

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 17.6: Profile of the accessibility of flats with shared facilities by region, 2015
No level
access
and
cannot fit
ramp
Could fit
ramp
Has level
access
All flats
with
shared
facilities
North East
26.8
35.5
37.7
100.0
North West
14.9
42.1
43.1
100.0
Yorkshire and the
Humber
22.9
32.7
44.4
100.0
East Midlands
13.6
35.4
50.9
100.0
West Midlands
18.6
40.8
40.6
100.0
East
14.0
37.3
48.7
100.0
London
20.8
24.5
54.7
100.0
South East
17.7
41.4
40.9
100.0
South West
20.7
25.3
54.0
100.0
Total
18.9
33.1
48.0
100.0
Source: English Housing Survey, 2015
17.42 This review also examined level access in flats with shared facilities for those
households where at least one of the following were reported for any household
member: a long-term illness or disability
226
, registered disabled or a wheelchair
user (outside their home or all the time). The EHS estimates that there are
around 1.2 million households
227
with these health issues living in flats with
shared facilities; these households are more likely to require some form of
adaptation. Over half of these 1.2 million households (57% / 712,000) live in
basement or upper floor flats.
17.43 Overall, around half of these 1.2 million households already have level access
(49% / 620,000) and it would be possible to create this for a further 33%
(414,000 households). Figure 17.6 breaks down these figures by households
living in ground floor/non- ground floor flats.
226
This may be a physical or non-physical illness or disability.
227
We need to bear in mind that illness, disability and wheelchair use are likely to be under-reported
in the EHS.
238
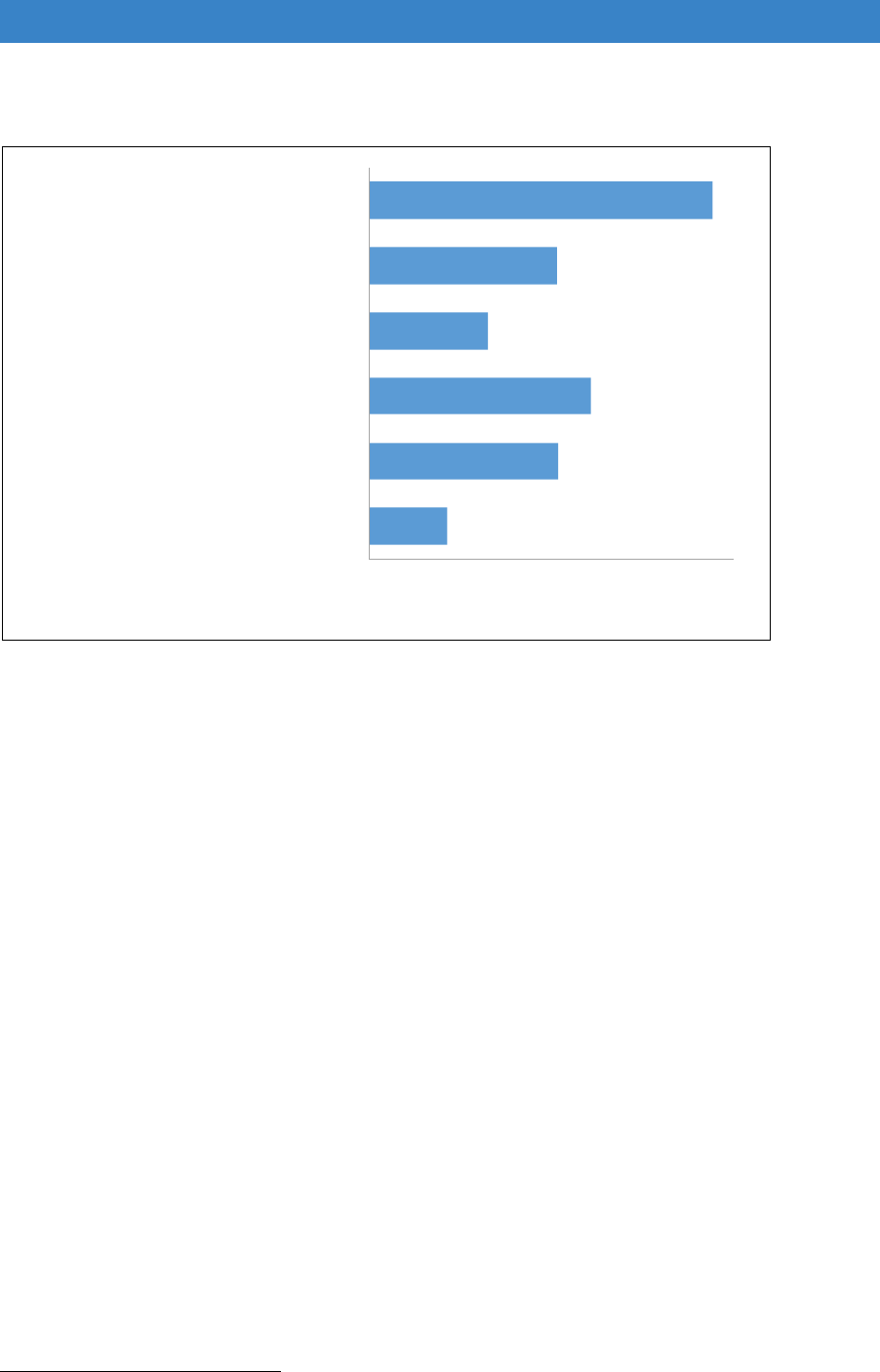
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 17.6: Accessibility of flats with shared facilities for households with illness or
disability, 2015
86
208
243
130
206
377
0 50 100 150 200 250 300 350 400
ground floor flat no level access and cannot
fit ramp
ground floor flat could fit ramp
ground floor flat has level access
upper/basement flat no level access and
cannot fit ramp
upper/basement flat could fit ramp
upper/basement flat has level access
households in flats with shared facilities (000s)
Source: English Housing Survey, 2015, household sub sample.
17.44 Due to small sample sizes, it is not possible to analyse the level access findings
in Figure 17.6 by tenure, region or other household characteristics. However,
for those households living in flats with shared areas who potentially need
assistance in accessing their home
228
, 34% are registered provider renters,
27% are private renters, 23% are local authority renters and the remaining 15%
are owner occupiers (Table 17.7).
17.45 The vast majority of these owner occupiers (87%) reported that they are
leaseholders. The tenure of some blocks can be very mixed, particularly in
council-owned blocks in London where, due to Right to Buy, there is often a mix
of local authority tenants, owner occupiers and private renters in the same
block. Many registered provider and privately owned blocks will also contain a
mix of owners and renters. Consideration of any adaptations needs to balance
the needs and interests of all concerned (the disabled person, other occupiers,
the freeholder and any leasehold owners). This involves having strategies and
policies on consultation and deciding how the works will be funded.
228
Households with either a family member with a long-term illness/disability, or a family member who
is registered disabled, or who uses a wheelchair outside their home or all the time.
239
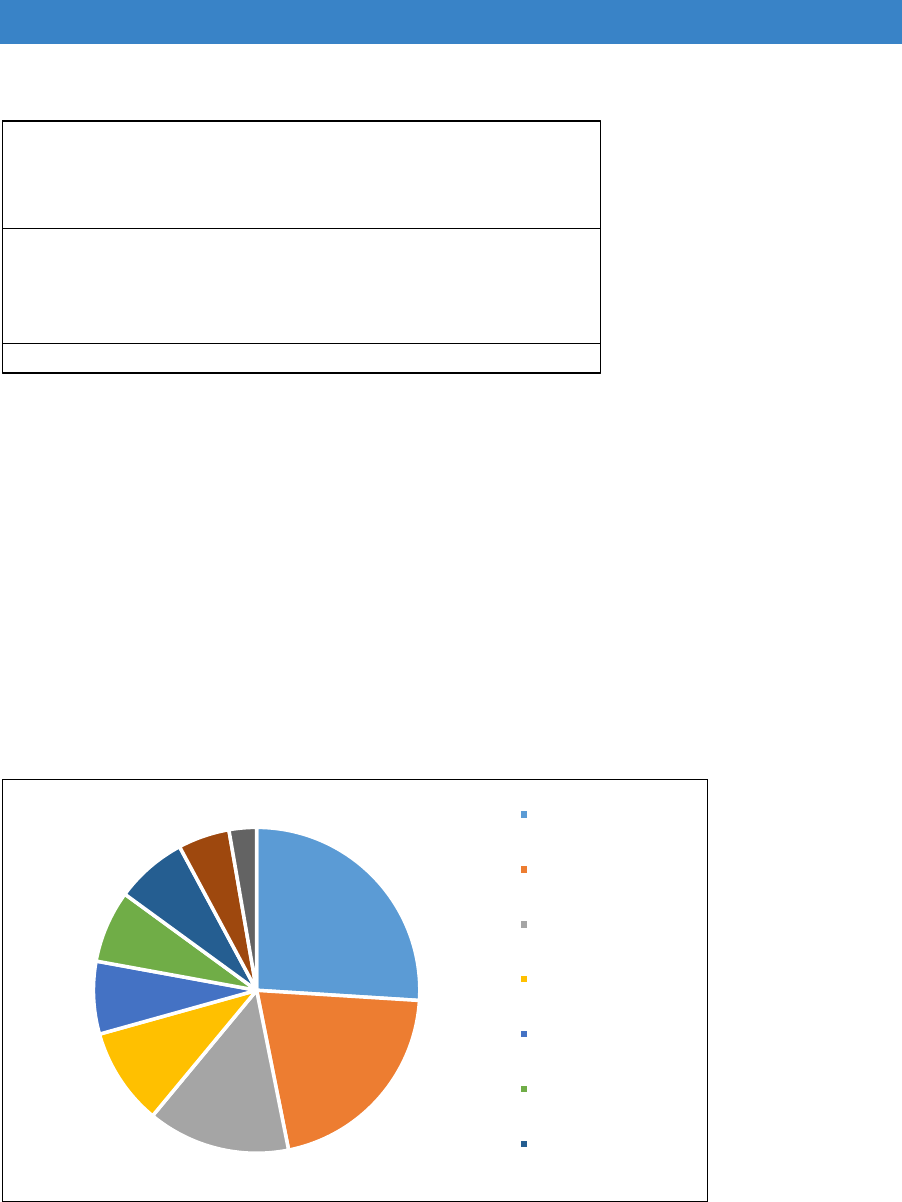
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Table 17.7 Households with illness or disability in flats with shared facilities, 2015
registered disabled, long
term illness or wheelchair
user all the time or outside
the home (000s)
percentage of
all applicable
households
owner occupier
193 15.4
private renter
336 26.9
local authority
292 23.3
registered provider
429 34.3
all households
1,250 100.0
Source: English Housing Survey, 2015
17.46 Figure 17.7 shows the estimated regional distribution of the 1.2 million
households living in flats with shared areas who potentially need assistance in
accessing their home. The EHS estimates that around one quarter of these
households live in London, while one fifth live in the South East of England.
Figure 17.7: Profile of households with illness or disability living in flats with shared
facilities by region, 2015
26
21
14
10
7
7
7
5
3
London
South East
North West
South West
Yorkshire and the
Humber
East
West Midlands
Source: English Housing Survey, 2015
240
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Potential cost of providing level access to flats with shared
facilities
17.47 The FOI data suggests that the typical cost of installing a ramp and undertaking
some path widening in flats with common areas is around £5,150.
17.48 If we use the EHS data for households in non-local authority owned homes that
have a potential need for level access (Table 17.7) and the overall proportion
of homes in each tenure that can be made more accessible by installing a ramp
(percentages in Table 17.4), it is possible to give a very rough and simplistic
estimate of the total monies potentially needed to install a ramp/undertake path
widening.
17.49 Critically, however, the estimate in Table 17.8 is unable to consider the ability
of the household to pay for the work and assumes that the cost of the work
would be the same irrespective of tenure and other issues that can impact on
costs such as any regional building costs variations. The estimate can only be
considered, therefore, as a ‘worst case scenario’ for funding needs. The
estimated monies required for the potential work is £1.6 billion pounds, roughly
four times the amount of the current DFG allocations to local authorities.
Table 17.8 Estimated budget required to provide level access for those with
potential need
registered disabiled, long
term illness or wheelchair
user all the time or outside
the home (000s)
could install
ramp where one
doesn't exist
cost per
adaptation
(£)
total
estimated
costs
(£000s)
owner occupied
193 0.30 5,150 295,621
private rented
336 0.40 5,150 693,207
registered provider
429 0.27 5,150 588,660
1,577,488
17.50 We need to bear in mind that, for all tenures, this would still leave around
216,000 households, with long-term illness or disability, living in flats with
shared facilities where it would simply not be feasible to install a ramp.
Lifts
17.51 The EHS classifies the size of lifts available in flats with common parts into three
categories: spacious, average and tight. Although exact dimensions are not
recorded, it is likely that only a spacious lift would be able to comfortably
accommodate a wheelchair user and another person, while an average sized
lift may be able to accommodate a wheelchair, but with difficulty. The EHS
241

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Potential Stock Improvements Report 2015-16
229
indicates that in 2015 there
were 3 million flats within the housing stock where the entrance level was not
on the ground floor, but only 91,000 (3%) of these had a spacious sized lift. An
average sized lift was present in 17% of these flats, 6% had a tight lift, leaving
74% with no lift available.
17.52 Any work involved to adapt a lift would be very major undertaking e.g.
constructing a new lift tower and installing a new lift. Irrespective of the huge
costs involved, in many cases it would simply not be feasible to do this work
because of lack of space to either fit an additional lift tower or install a lift or a
larger lift within the existing structure of the block of flats. Work to lifts is,
therefore, not the most realistic way of dealing with people with disabilities who
are unable to leave their flat and reach the main entrance due to lack of lift
access.
17.53 Solutions may include the installation of stairlifts
230
or platform lifts. The FOI
information suggests that typical costs for these two adaptations are £4,250
and £13,180 respectively. It is very difficult to provide any estimate for the
potential need for these types of DFGs, not least because we do not have any
data on the feasibility of undertaking work in various types of flats.
17.54 We can, however, make a very rough and simplistic estimate of improving
accessibility for some wheelchair users; once again this estimate can only be
considered as a worst-case scenario for potential funding requirements.
17.55 The EHS estimates that there are roughly 41,000 households living in upper
floor or basements flats where a member of the household uses a wheelchair
either outside their home or all the time. Although it is not possible to reliably
report on the floor level of the flat by tenure for these households, the EHS also
estimates that 74% of wheelchair users (outside the home or all the time) are
not local authority renters. Applying this percentage gives an estimated 31,000
households who would benefit from some form of lift provided under DFGs if
feasible to install - a cost of roughly £129 - £400 million.
229
Ministry of Housing, Communities and Local Government (2017a) English Housing Survey 2015-2016:
potential for stock improvements, London: MHCLG. https://www.gov.uk/government/statistics/english-housing-
survey-2015-to-2016-potential-for-stock-improvements.
230
Installing a stairlift can make stairs more dangerous for other non-disabled users as stairs are
effectively narrower and obstructed so that trip hazards may be created. In common areas, stairlifts
may also be more likely to be vandalised/misused.
242

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Housing Health and Safety Rating System (HHSRS) hazards
17.56 The EHS undertakes HHSRS
231
assessments on the prevalence of the risk of
falls that are significantly higher than average, and these are a good indicator
of serious barriers and hazards for people with mobility problems or other
disabilities. These risks are assessed for the individual dwelling and the main
rear and front routes to it but not to the whole access way system in flats with
common parts.
17.57 Among the 3.5 million flats with common parts, it is estimated that 4% (148,000)
have significant hazards related to falls (on stairs, between levels or on the
level). The EHS estimates that around a third (32%/46,000) of these 148,000
flats are occupied by households with a disability/illness.
17.58 As the estimate for significant hazards represents the worst risks only, it likely
underestimates the number of flats requiring improvements to accessibility of
common entrances, stairs and corridors. We currently have, however, no way
of knowing how great the difference may be.
17.59 Estimating the cost of work required to common parts is problematic because
there is limited data available. The EHS can model potential costs, but these
would represent the costs of reducing the hazard to an ‘acceptable’ level which
may not be good enough to ensure improved accessibility. For example, many
falls on stairs hazards could be simply reduced by providing an extra handrail
to the stairs and/or improving the lighting whereas improvements to
accessibility will generally require more extensive works.
FOI data
17.60 For those 17 local authorities that provided information on the adaptations they
approved to common parts in 2016-17, we have a breakdown of the type of
adaptation and the associated costs, Figure 17.8 and Table 17.9.
231
The HHSRS is the government’s evidence-based risk assessment procedure for residential
properties. It is a means of identifying defects in dwellings and of evaluating the potential effect of any
defects on the health and safety of occupants, visitors, neighbours and passers-by. The system
provides a means of rating the seriousness of any hazard so that it is possible to differentiate between
minor hazards and those where there is an imminent threat of major harm or even death. Potential
hazards are assessed in relation to the most vulnerable class of person who might typically occupy or
visit the dwelling. For example, for falls on stairs and falls on the level, the vulnerable group is defined
as persons over 60 years.
243
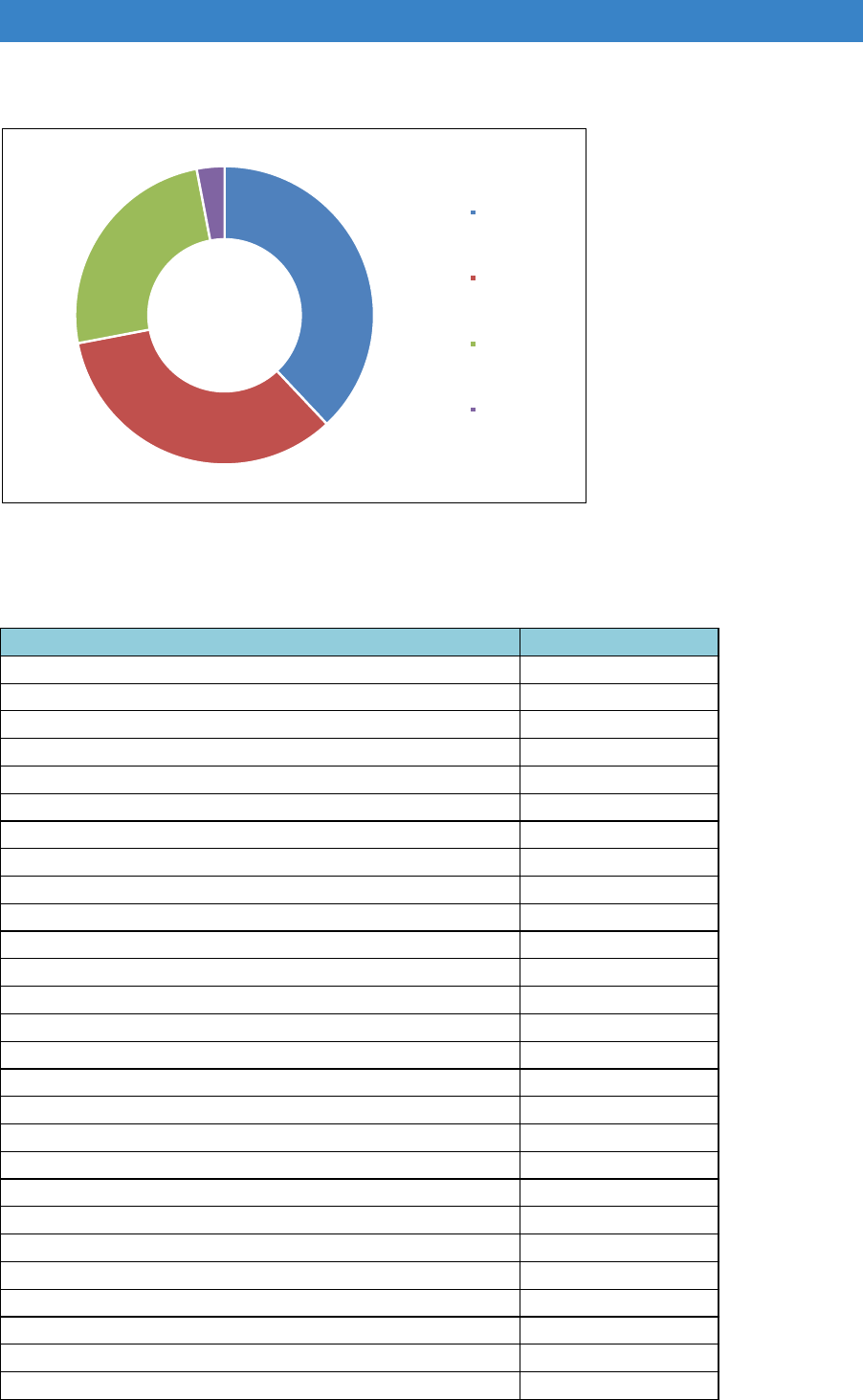
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Figure 17.8: Profile of types of DFG adaptations undertaken by local authorities,
2016-17
38
34
25
3
ramp/path
widening
automatic doors
stairlifts
platform lifts
Source: Foundations FOI 2018
Table 17.9 Cost of DFG to common parts, 2016-17
Type of DFG
External PlatformLift £13,180
Wheelchair Access and ramping/ path widening £12,000
Wheelchair Access and ramping/ path widening £9,000
Automatic doors and ramps £8,654
Automatic doors and ramp £6,560
Ramping £6,000
Electrical door access & ramping £5,300
Stairlift £5,225
Ramping/ path widening £5,000
Curved Stairlift £4,640
Stairlift to communal entrance stairs £4,485
Automation of main door to block and internal door £4,250
Reconfigure steps on communal access £3,749
External stairlift to shared access steps £3,725
Stairlift in communal stairwell £3,549
Automated Door opener £3,443
Ramping/ path widening £3,300
External stairlift on communal steps £3,175
Ramping/ path widening £3,000
Automation of main communal front door £2,814
Door Entry System £2,420
Widen shared access path £2,300
Door opening and intercom system £2,240
Automatic entrance door £2,140
Wheelchair Access and ramping/ path widening £2,000
Electrical door access £2,000
Communal door alterations £1,882
244

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Summary points – Section 36 of the Equality Act
This review seeks to better understand how the future commencement of
Section 36 of the Equality Act could impact on DFG demand and its potential
funding requirements. Regrettably there is little available data that can help
inform this, although the FOI requests have provided an insight into the DFG
work approved for common areas in 2016/17; 40 such DFGs approved by 17
local authorities. The most common types of DFG works to common areas
were installing ramps and widening paths, followed by installing
automatic doors.
We were only able to produce ‘worse case’ scenario estimates of potential
DFG costs for installing ramps and stairlifts/platform lifts to common
parts for households who reported long-term illness or disability (for the EHS).
These estimates could not factor in people’s ability to pay for the work.
The BRE 2011 review, which tried to predict DFG demand for common areas,
concluded that works to common parts should be dealt with strategically
by local housing authorities and registered providers rather than in a one-
off piecemeal manner using DFG. At the present time, it seems this
conclusion still holds, although we should add that this is another area of the
DFG where consideration should be given to more resourcing from
commissioning bodies, given the potential savings to care and hospital
budgets.
The DFG could be used to facilitate a move to more appropriate
accommodation. This would be particularly relevant where adaptations to
common parts are simply not feasible to undertake or prohibitively expensive
(for the local authority or for household where a contribution is required).
Recommendations – tenure and equality
Further research is needed on the role of social landlords in providing
adaptations and the feasibility of a national adaptations protocol for
registered providers
More research is also needed on ways to engage with private landlords
and deliver adaptations more effectively in the private rented stock.
Social housing providers to be included on Housing and Health
Partnership Boards to develop a local strategy for adaptations and
accessible housing.
A national award for landlords with effective adaptation and accessible
homes policies.
Works to common parts should be dealt with by the local Housing and
Health Partnership Board rather than in a one-off piecemeal manner
using the DFG.
245

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Chapter 18. Summary, conclusions and recommendations
18.1 This has been a practical review to suggest, not just what should change in
DFG delivery, but how it should change. It provides examples to show how
transformation has been undertaken in areas that are pioneering new ways of
working. It shows how far those areas have come in joining up housing with
health and social care to provide wrap-around services for disabled and older
people. It demonstrates the need for areas with traditional DFG policies to
develop much more integrated ways of working.
18.2 At the centre of new integrated services is the disabled or older person, their
family and carers. The home is the hub of most people’s lives, but for people
who are impaired it takes on greater significance as it is often the place where
they spend most of their time. Research is beginning to indicate the negative
effect of delays in installing adaptations on health, wellbeing and fear of falling.
To ensure that people remain independent customer pathways need to be less
complex and faster.
18.3 Disabled and older people want an efficient, seamless service, where they are
fully consulted and given choices about the changes made to their home. It is
important to provide adaptations that are effective, well designed, fit with their
personal style and are not stigmatising by making the home look like a hospital.
Housing and Health Partnership Board
18.4 The way the delivery of adaptations has been split between social care and
housing has been an obstacle to the development of effective services for
almost 30 years. A single Housing and Health Partnership Board is needed for
each county and unitary authority to oversee home adaptations services which
will report to the BCF and HWB (or any successor bodies). This approach was
endorsed by most of the contributors to the review. To ensure that mandatory
DFG funds are protected, the BCF will have to report on DFG spending
separately each year.
Making the service more visible
18.5 The grant needs renaming to bring it up to date and to reflect that it is part of a
broader set interventions to help people remain independent. The rebranding
needs to portray a youthful image and be immediately recognisable. Disabled
and older people, their families and carers need to know where to turn for help
throughout the country. It should also be easy for other professionals (outside
of adaptation teams) to know exactly where to refer people who need support
with adapting their home.
246

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Integrating services
18.6 Several examples are provided of places that have developed integrated
services. The Dorset Accessible Homes Service, Warwickshire’s HEART
service and Leicestershire’s Lightbulb service demonstrate that integration is
possible even in big county authorities and those with scattered rural
populations. Some of these services are now more integrated than urban
unitary authorities. As health and social care integration progresses, Salford
provides an example of an alternative way of organising services in an urban
unitary by co-locating the adaptation team with health staff to provide more
holistic services focussed on the home.
18.7 Each service is tailored to local circumstances and is therefore slightly different,
but common themes emerged:
A strategic partnership board and a strategic plan
Linked services using ICES and DFG budgets often including additional
funding
A single access point
Integrated teams under a single manager
Effective routing to staff with the right skills
Cross-trained staff able to support customers through the process
An RRO policy
Preventative and wrap-around services
Effective end-to-end IT systems
Effective reporting on outputs, outcomes and impact and continual feedback
and learning
18.8 The results show that fewer people drop out, there are less steps in the
customer pathway, handovers are minimised, and services are much quicker.
Customers don’t get lost in the system but have a single point of access and a
contact person to call if they have a query.
18.9 However, developing integrated services is not easy. Setting up a strategic
partnership board and having the right policies in place is just the beginning. It
is as much about cultural change and fully involving staff in the process.
18.10 The DFG is such a small budget in comparison to those in health and social
care that it has been largely ignored. Strategic managers need to appreciate
the transformative results home adaptations can bring for disabled people. To
emphasise the importance of safe and accessible housing a new metric should
be added to the reporting structure of the BCF (or successor body) on ‘the
number of people helped to remain independent at home’.
247

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Transformation funding
18.11 To enable change to happen across the country it is recommended that a Home
Independence Transformation Fund is established, which is equivalent to 1%
of the overall budget. This would provide advisors to help each authority that
needs external support to transform services. There is also scope for
secondments to areas that already have integrated services to ensure the
learning is passed on.
Working better together
18.12 The review gives practical ways of solving some of the problems inherent in
current ways of working. It starts with the beginning of the process and making
sure that good conversations are had with customers to fully understand their
needs before routing them into the right part of the service. By working out how
complex the case is likely to be, they can be directed to teams with appropriate
skills.
18.13 New staff posts which combine the skills of trusted assessor, casework and
grant officer seem to be a very effective way of dealing with straightforward
cases and provide a single point of contact for the service user. More complex
cases need occupational therapists and technical staff to work together. The
review provides a new set of tools and ways of thinking that will make this
process easier.
18.14 Nine principles for installing adaptations are given that should guide the process
of working with customers, which include: the need to retain (or restore) dignity;
the need to have values recognised; the need for relief from pain, discomfort
and danger; the need to minimise barriers to independence; the need for some
element of choice; the need for good communication as part of giving choice;
and the needs of other family members and of the family as a whole. In addition,
there should be awareness of the need for light and the needs of children to
growth and change and have enough space. To improve collaboration and
communication with customers, there should be more use of 3D visual
representation and design centres so that they can clearly see what is proposed
and how it will affect their use of the home.
18.15 There is also the potential to work in a much more preventative way. This
requires better liaison with health and social care to identify people earlier using
the principal of ‘making every contact count’ so that problems with the home
are picked up well before people get to crisis stage. New integrated adaptation
services are also more likely to provide help with falls prevention and hospital
discharge. There is also scope to use the DFG to provide dementia grants to
help people remain independent at home for longer.
Data collection and reporting
18.16 A focus on outcomes and impact is vital as part of service redesign. This means
alignment of IT systems, use of NHS numbers on all files and protocols for data
248

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
sharing. There are new reporting dashboards that can show results each
quarter, benchmark against other authorities and help with continual service
improvement. It is proposed that the old LOGASnet annual returns are replaced
with a quarterly reporting system based on the local returns to the Housing and
Health Board and the HWB. But at the heart of reporting systems should be
ways of showing how the home situation has improved for each customer and
the impact of adaptations on their health and wellbeing and their ability to meet
their own goals.
Resources
National allocation
18.17 A previous report indicated that there might be a possible misalignment of
allocations to local need, however, there are no robust data that can accurately
predict the need for DFG at regional or local level. It is further complicated by
the fact that under-spending by some local authorities and overspending by
others are not solely due to current allocations but may relate to the efficiency
of the local DFG process and the way that it is resourced.
18.18 Any change in allocations has to be based on a formula that is simple,
transparent, fair and robust. The review used disability related DWP data to
establish a baseline proxy indicator of needs, due to its transparency and
regularity of update. It then introduced other factors of potential DFG need and
examined their impact on allocations. These included: ability to pay, frail elderly
data and tenure. It also raised the question of whether further factors relating
to age and income should be included. Housing costs and regional building cost
data could also be introduced.
18.19 The initial results show that any change in allocation methodology is likely to
result in significant ‘winners’ and ‘losers’. This because the impact of bids made
in 2010/11 still influences allocations today. A new allocation formula would
need to be incrementally introduced over a number of years to prevent a
sudden, large change in resource levels.
18.20 More sensitivity analysis is needed to look at impact of factors across regions
and all local authorities to further refine a new allocations formula. It is
recommended that a new formula is established in time for the next
Comprehensive Spending Review and is applied incrementally over the
implementation period of that Review.
Other funding issues
18.21 The funding of adaptations used to be more of a partnership between local and
central government, with 40% coming from local sources. The combination of
austerity and the rise in central government funding has meant that local capital
funding provision has declined to very low levels in most areas. Fees taken from
249

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
that capital pot have had to be used to cover a large proportion of revenue
costs.
18.22 To underpin funding and staffing decisions at local level there has to be much
greater understanding of the level of need for adaptations through detailed data
analysis, working closely with housing and care providers or advertising the
service more widely. This would help staff present a case for further local
funding to match central government resources. The development of new
integrated services should include exploration of ways to bring in a broader mix
of funding options.
18.23 Given the difficulties in fine tuning allocations to need, there should be
consideration of more collaborative DFG funding arrangements among BCF
partners. Demand can vary from year to year, and the number of high-cost
cases can also fluctuate. For small authorities, major adaptations over the
upper limit are very difficult to deal with as they potentially absorb a high
proportion of the overall budget. A risk-sharing arrangement is recommended,
controlled by the Housing and Health Board, to ensure that disabled people can
get equal access to resources when they are needed.
18.24 The Housing and Health Partnership Boards and integrated working
arrangements should allow funding decisions for more expensive cases to be
made differently. A fundamental problem with the existing arrangements is that
in most areas the DFG must absorb all the costs of more complex adaptations.
However, if that adaptation work: helps to keep a family together; prevents a
disabled son or daughter becoming a ‘looked after child’; allows someone with
a major injury or impairment to leave hospital; reduces care requirements; or
has a significant effect on health and wellbeing, there is a business case for
joint funding from a number of different housing, health and social care budgets.
There is also scope for adaptation funding to be provided as part of new
personal health and care budgets to help people better achieve their own goals.
The means test
18.25 Three main options were considered to update the means test:
1) The first option is to remove the test completely, or for certain cases, say
those under £5,000. In a time of austerity there are arguments against
providing funding to those who can afford their own provision and removing
it for certain cases was thought to be unsustainable longer term. There is a
lack of robust evidence about the savings major adaptations bring to health
and social care. The best potential payback comes from the mitigation of
falls on stairs. The review therefore recommends that stairlifts are removed
from means testing, subject to certain caveats, but only where an authority
has set up an effective stairlift refurbishment and recycling scheme. There
is also a case to give a grant without means testing for palliative care.
250

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
2) The second option is to update the present test as it is complex, has not
been updated since 2008 and the passporting arrangements are out of date.
However, it is not a straightforward process. A number of different ways
were considered: including ways of assessing need, re-establishing the
links with housing benefit rates, assessing resources and entitlement and
passporting.
3) The final option considered is to adopt the Care and Support Charging
Regulations. This was favoured by people who took part in the consultation
for this review as it would remove the confusion about having two different
tests, but again it is not a straightforward solution.
18.26 The recommendation is that assessment for DFG within Care and Support
Charging Regulations is included in the Social Care Green Paper but there
should be provision for passporting arrangements and a standard minimum
amount for Disability Related Expenditure. If this is not possible, the alternative
is to update the existing means testing regulations. This will require re-
establishing the link to housing benefit rates, using LHA rates for the Housing
Allowance and updating the passporting benefits lists.
The upper limit
18.27 The upper limit of the grant has not changed since 2008 and has not been
adjusted to account for inflation. It is clearly too low to cover the costs of more
complex adaptations, particularly in areas with high building costs. As a result,
many authorities have set their own level.
18.28 The review recommends moving away from a ‘one size fits all’ model. The
maximum amount should be raised in line with inflation, with a regional
weighting based on building costs. Due to the importance of professional
expertise on larger projects it is also recommended that the regional upper
limits are increased by a further 10% to ensure that the right support is provided.
This local maximum amount should be clearly stated on each local authority
website.
18.29 Raising the limit and changing the way decisions are made could alter the
thinking about these grants from ‘expenditure’ to ‘investment’. It would allow a
much more person-centre approach which could provide long-term solutions to
increase disabled people’s independence.
18.30 There is also a need to look at the way VAT is paid on adaptations as bedrooms
and kitchens extensions are subject to VAT while bathrooms are not.
251

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Regulation
18.31 A number of other aspects of the regulation were looked at. Given the need for
a broader range of services delivered in a more flexible way it was
recommended that every authority has an RRO policy.
18.32 The 6-month time limit to approve an application is part of the primary legislation
but one that is often circumvented. It does not reflect the end to end customer
journey and the waits at other stages. As a result, future guidance should stress
the requirement to approve or refuse and application “as soon as reasonably
practicable” where the Local Authority has had prior involvement with the
application. In most cases this should take no longer than 4 weeks.
18.33 The legislation, regulations, consents and orders, guidance, good practice
guides and the Regulatory Reform Order have created a complicated system
that few people fully understand. It is recommended that all the guidance is
brought together and fully revised so that it clearly sets out expectations for
local authorities and rights of a disabled person making an application.
Developing a market
18.34 The main barriers to better design and innovation are the lack of integration in
the market, and the lack of standardisation and repetition in specification. The
traditional procurement processes of seeking multiple quotations has reinforced
these barriers. Addressing them calls for both reform of procurement processes
and greater efficiency in their operation. The review calls for services to use an
online schedule of rates, to make much more use of flat-pack extensions, to
have a stairlift recycling scheme, and for there to be some common standards
for materials.
18.35 There also needs to be better training of builders and tradespeople to give them
trusted assessor skills. If this was included in the Trustmark rating system, it
would help both adaptation service providers and people aiming to do their own
adaptations.
18.36 There are some interesting developments in assistive technology field using
already available items such as smart phones, speaker systems and low-cost
sensors. These can potentially give disabled people much more control over
their home environment. They also allow unobtrusive and effective monitoring
where someone might fall or has dementia. There is scope to use technology
in diagnostics, for example to work out when someone needs a stairlift by
monitoring their movement up and down stairs.
18.37 The average cost of installing voice-controlled smart heating, lighting and
electrical control systems is only about £250 per home. If this was routinely
included in the DFG it would cost around £12.5m a year. Customers are already
252

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
getting used to these types of systems which are non-intrusive and non-
stigmatising. Use of low-cost consumer technology as part of DFG-funded
home modifications would encourage more widespread adoption, enhancing
the UK’s potential to be a world leader in assistive technology in line with the
Industrial Strategy.
Helping people outside the DFG
18.38 The market for stairlifts and adapted bathroom and kitchen products is steadily
developing with more choice on offer in mainstream retailers and online. Many
people are choosing to put in wet rooms and to install downstairs bathrooms.
But we do not know that much about what people are already doing, how
effective it is, what holds people back and what might encourage them to do
more to ‘future-proof’ their homes. Statutory services tend to focus on older
people, but most unmet need for adaptations may be amongst younger
households.
18.39 Relying on the market to solve all the problem is unrealistic as there is an
information gap. Showrooms are not good settings to discuss personal
problems and retail staff are not trained to give appropriate advice. There are a
bewildering array of products and it is all too easy to make mistakes which are
hard to rectify, especially for people with more limited resources.
18.40 There is clearly a role for the public sector to provide more advice, information
and signposting. The problem is that home owners and people in the private
rented sector do not naturally turn to the local council for advice. Better branding
and advertising would make services better known. There is scope for more
online advice produced at national level and closer working with existing online
providers.
18.41 If designs used in the DFG, or delivered by ICES, were more aspirational it
would be possible to ‘shape the market’ and this could help drive what is shown
in mainstream retailers. There is also potential for local authorities to develop
their own service for retail customers outside of the DFG.
18.42 There are clearly a lot of people able to self-fund. For older people, in addition
to using income, there is an expanding range of options available, including:
pension freedoms, equity release, life-time mortgages, and in some place, local
authority loans. There also seems to greater willingness to use these options.
18.43 But there is a group who do not qualify for the DFG who find it hard to raise the
required funding. Particularly problematic is the situation for younger disabled
people who have low levels of equity, high mortgage costs and little spare
income. Altering the means test or bringing it into line with the test for social
care, may bring some of this group into the DFG, but there are others who will
still fall outside the requirements. Advice and information will be crucial to help
253

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
them spend their limited resources widely. Adaptation services and home
improvement agencies need to be aware of the needs of this cohort and make
sure that services are not overly geared to an older demographic.
18.44 There is also an argument for including spending on adaptations as part of the
social care cap, as removing hazards in the home is likely to lead to fewer
accidents and injuries thus reducing costs for health and social care. It would
also help to raise awareness of the benefits of preparing the home for later life
or as an alternative to paying for domiciliary care, reducing the likelihood of
people reaching the care cap. It is something that needs to be considered in
the Social Care Green Paper.
Tenure and equality issues
18.45 Tenure was not included as part of this review, but it is impossible to ignore. A
third of grants (34%) go to registered provider tenants as they have a clearly
signposted route to the DFG via their landlord. However, there are similar
numbers of people with long-term illness and impairments in the private rented
sector who may be in much poorer housing conditions and many home owners
are unaware of the grant and may also be excluded. Adaptations in the council
stock are delivered using the HRA budget and so sit outside the DFG making it
hard to develop local adaptation strategies.
18.46 Tenure issues need a separate review to see if services between tenures are
equitable and to determine if the DFG allocation formula needs to be adjusted
to give areas with higher levels of registered providers more funding. But it is a
complicated picture. Registered landlords may contribute money to the DFG
but it is not recorded in LOGASnet returns. Others are more like council
landlords and have their own budget and staff to deliver adaptations. Some also
fund home improvement agencies and so contribute in other ways to private
sector home improvement. However, other registered providers make
considerable demands on the DFG budget but give little in return.
18.47 It is important to include local providers on Housing and Health Partnership
Boards. However, it is sometimes more difficult to engage with national and
regional providers who operate across large numbers of authorities. A national
protocol would be the most effective way to get housing associations to
contribute to DFG funding, have more consistent policies for their disabled
tenants and ensure that home choice systems work effectively. This needs to
be explored to see if it is feasible.
18.48 Private renting is becoming a much bigger issue as more disabled people are
likely to be in this tenure from now on. Conditions are very variable and one in
three disabled people in this sector said that their home does not meet their
needs. Barriers to adaptation include: short term tenancies and landlords
refusing permission to change the home. Local authorities could encourage
254

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
more adaptations through licensing agreements or grant funding to remove the
adaptations at the end of the tenancy. More research is needed to understand
the barriers to adaptations in the private rented sector.
Common parts grants and the Equality Act
18.49 The Government has made a commitment to review the remaining provisions
of Section 36 of the Act which includes adaptations to the common parts of
residential properties. There is little available data to determine the likely effect
on DFG demand and funding requirements. The review was only able to give
‘worst case’ scenarios based on what little data is available. These estimates
are unable factor in people’s ability to pay for the work.
18.50 The typical cost of installing a ramp and undertaking some path widening in
flats with common areas appears to be around £5,150 which might cost £1.6
billion pounds, roughly four times the amount of the current DFG allocations to
local authorities. To provide a lift (if feasible to install) would cost roughly £129
- £400 million. In addition, it is estimated that 4% (148,000) of flats with common
parts have significant hazards related to falls (on stairs, between levels or on
the level) with around a third occupied by households with a disability or long-
term illness. However, the work required might be anything from fitting a
handrail to major improvement, so it is impossible estimate the likely cost.
18.51 Current DFG data is not helpful in arriving at cost figures as there is very little
of this work taking place. All we know is that DFG works to common areas most
frequently include installing ramps and widening paths, followed by installing
automatic doors.
18.52 The recommendation is that works to common parts should be dealt with
strategically by local housing authorities and registered providers rather than in
a one-off piecemeal manner using DFG, and consideration should be given to
more resourcing from strategic partnership bodies given the potential savings
to care and hospital budgets. Alternatively, the DFG could be used to facilitate
a move to more appropriate accommodation, particularly where adaptations are
not feasible to undertake or prohibitively expensive.
Conclusions
18.53 This review has been wide ranging. It has provided an assessment of how the
DFG is currently being used and made detailed, evidence-based
recommendations about how the DFG and the wider housing environment
should change. It has sought to give Government a way of developing more
effective ways to enable more people to live in suitable housing so they can
stay independent for longer. It has also made the case for more joined-up action
across housing, health and social care.
255

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
18.54 We set out a more person-centred and integrated way of delivering home
adaptations but recognise that this will need strong leadership and
transformation funding to enable change to happen. Better information and
advice is also recommended, both locally and nationally. This will lead to more
collaboration between housing and social care, innovation and robust data that
shows the true benefits of a safe and suitable home environment.
18.55 The current formula for allocating funding does not properly reflect need from
authority to authority, but it is not just a case of redistribution. There should be
an element of risk sharing which reflects fluctuations in demand and exceptional
cases which require significant investment over and above maximum limit –
which we are recommending should be increased in line with inflation and
regional building costs.
18.56 Joining up DFG delivery with health and social care is inconsistent with
maintaining an entirely separate means testing regime and so we recommend
ways in which the Care and Support Charging Regulation could be used.
However, we also recognise that social care charging is due to be reviewed
and so have included recommendations for also updating the current DFG
means test. Either way, we think there is a great opportunity for adaptation
costs to count towards a possible care cap, so that people are encouraged to
make changes to their home that would reduce future care costs, and thereby
decrease the chance of them ever reaching the cap which would mean savings
for Social Care.
18.57 All of this means that the current DFG Guidance would be out of date and need
completely revising.
18.58 The annual spend of nearly £0.5bn could be better co-ordinated to help shape
the market for home adaptations – encouraging more contractors to enter and
manufacturers to innovate more. The potential to adopt smart home technology
as part of the UK Industrial Strategy is also advocated.
18.59 Finally, we highlight some of the issues faced by different types of tenant when
they need to make adaptations to their home and the costs and difficulties of
making adaptations to common parts.
18.60 The following section brings together all the recommendations from throughout
the report. Although the review was based on evidence from a wide range of
sources, there is still a need for more research and development. The final
section identifies some key areas for further work.
256

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Recommendations - overview
Recommendations - strategic oversight
A Housing and Health Partnership Board in each area as a requirement of
DFG funding with representatives from housing, health and social care.
Each BCF and HWB to report separately on DFG funding and on a new
metric ‘the number of people helped to remain independent at home’.
Housing and Health Partnership Boards to have a similar structure to
Local Safeguarding Children’s Boards.
The DFG and ICES budgets to be in the same funding pot (the BCF or its
successor) to join up DFG services with equipment provision and minor
adaptations.
A single adaptations policy to be developed for each area, based on the
needs of the locality, reviewed annually and signed off by the HWB.
A new name for the grant, the services that provide it and the national
advice organisation, and for that name to be used consistently across the
country.
Recommendations – local delivery
Integrated teams in all areas to simplify and speed up customer journeys.
A Home Independence Transformation Fund equivalent to 1% of the
national DFG allocation to help develop integrated services in all areas.
Recommendations – working better together
Better analysis of local need to develop preventative strategies and
determine levels of revenue and capital funding.
Better partnerships with health and care to ensure that ‘Making Every
Contact Count’ works effectively to refer people earlier, not at crisis point.
A single point of access with ‘good conversations’ at the start so that
people are routed down appropriate pathways.
New staff roles combining occupational therapy, technical and casework
skills developed to support customers more effectively.
257

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
New decision-making tools to help occupational therapy and technical
staff collaborate more effectively.
Use of 3D design and design centres to communicate better with
customers and tailor solutions to people’s own goals.
Use of NHS number on all files, data sharing protocols, aligned IT systems
and improved local reporting focussed more on outcomes.
National reporting by each Housing and Health Partnership Board as a
requirement of future BCF plans.
Recommendations - allocation of resources and other funding issues
That the allocation formula options are explored further using sensitivity
analysis.
That a new allocation formula is established for the next Comprehensive
Spending Review and is applied incrementally over the implementation
period of that Review.
That integrated services seek capital and revenue funding from a wider
range of sources.
That risk-share funds are set up to deal with uneven demand for grants
and that very expensive adaptations are jointly funded by housing, health
and social care.
That the DFG is included in personal budgets to provide solutions that
meet people’s own goals.
Recommendations – the means test
That including assessment for the DFG within Care and Support Charging
Regulations is part of the Social Care Green Paper.
That alternatively the existing means testing regulations are updated.
That stairlifts are removed from means testing where an authority has set
up an effective stairlift refurbishment and recycling scheme.
That further work looks at removing the means test for palliative care.
258

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Recommendations – regulation and the upper limit
That the maximum amount of the DFG is raised in line with inflation, with
a regional weighting based on building costs and an amount for
professional fees.
That the VAT rules are revisited for major adaptations.
Regulatory Reform Order (RRO) Policies have been developed in about
half of local authorities and need to be adopted in all areas to provide
more flexible use of the grant.
Each area to have simple application forms available on request.
Applications should be determined within four weeks where the Local
Authority has had prior involvement with the application.
That the guidance is fully revised to reflect integrated services, the
expectations for local authorities and the rights of the disabled person.
That the Services and Charges Order list is updated to include support
with moving and the funding of extended warranties.
That the national advice line is updated and improved to give people
support with housing options.
Recommendations – developing a market
A further five-year funding programme for the DFG to improve certainty
and enable local authorities to invest in better procurement.
A national accreditation scheme for builders and tradespeople.
Use of an online schedule of rates to increase efficiencies and further
work to assess the effectiveness of framework agreements.
Flat-pack extensions to be used to provide a faster service with further
research to identify the best solutions.
A smart home starter kit as part of every DFG application.
Local authorities and home improvement agencies to provide advice,
information and handyperson services for people outside the DFG.
Further research on what people do outside the DFG to encourage more
‘future-proofing’.
259

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Spending on adaptations outside of the DFG to be included as part of the
social care cap and considered in the Social Care Green Paper to
incentivise people to prepare their homes for later life.
Recommendations – tenure and equality
Further research is needed on the role of social landlords in providing
adaptations and the feasibility of a national adaptations protocol for
registered providers.
More research is also needed on ways to engage with private landlords
and deliver adaptations more effectively in the private rented stock.
Social housing providers to be included on Housing and Health
Partnership Boards to develop a local strategy for adaptations and
accessible housing.
A national award for landlords with effective adaptation and accessible
homes policies.
Works to common parts should be dealt with by the local Housing and
Health Partnership Board rather than in a one-off piecemeal manner using
the DFG.
Further research and development work
Some of the issues discussed in both Parts A and B of the report, and in the
recommendations listed above, include the need for more research and development.
These issues are brought together below:
More research to explore Local Safeguarding Children’s Boards and work with
local authorities, and their representative bodies, to develop a suitable structure
for Housing and Health Partnership Boards.
Further sensitivity analysis to test the options for the allocation formula.
Once the details of the Social Care Green Paper are published, more work will
be needed on the means test to see if it can be aligned with the test for social
care. If not, the current test needs to be updated. Passporting for stairlifts and
palliative care needs to be further developed.
Research with disabled and older people and their representative organisations
to explore the barriers and facilitators to getting adaptations and how more
future-proofing work could be encouraged.
260

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Home Independence Transformation Fund – develop learning tools and
materials and train advisors.
Work with RCOT, CIEH, Foundations and university and college training
programme providers to develop courses to prepare staff for new integrated
roles that cross traditional professional boundaries.
Work with Foundations, Trustmark, training programme providers and others to
develop better training, accreditation and rating systems for the construction
industry.
Research procurement issues including the effectiveness of framework
agreements, use of online schedules of rates, and the design of flat-pack
extensions to establish best practice.
Work with industry, retail suppliers, designers and others to develop new
adaptation designs: that will fit the small spaces in most people’s homes; that
are robust; that are easy to clean and maintain; that are low cost or reasonably
priced; but that are also desirable and fit with today’s lifestyles.
Work with authorities and home improvement agencies in areas with large
BAME populations to better understand the needs of different groups and how
the DFG could be provided more effectively and in ways that are culturally
sensitive.
Cases are becoming more complex, there are increasing numbers of customers
with multimorbidity, frailty or mental health issues and there are rising numbers
of children with social and behavioural problems. There are also more
specialised grants for dementia or visual impairment. More staff training will be
required (both online and off-line) by Foundations, RCOT and specialist
providers.
New tools for effective working need to be more fully developed, piloted in a
small number of local authorities before roll-out nationally:
o System for ‘good conversations’ and effective routing
o Complexity Framework to show what occupational therapy and technical
skills are required for each case
o Adaptations Design Communications Toolkit to provide a guide for
standard designs
o Home Modification Process Protocol to ensure better communication in
building projects
o New complex decision-making process: necessary → practicable →
appropriate → reasonable.
o 3D design tools to encourage better communication with customers.
261

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
The guidance needs to be fully revised so that it reflects integrated services
and clearly sets out the expectations for local authorities and the rights of the
disabled person making an application.
A new, national data collection system needs to be developed to take
advantage of the introduction of a replacement to LOGASnet. There will be a
need to work with BCF and HWBB policy makers to ensure that data is collected
and returned on a quarterly basis and that this addresses the new BCF metric
of ‘the number of people helped to remain independent at home’.
Tenure issues need a separate review to look at: the role of different landlords
and the barriers and facilitators to getting adaptations carried out. The feasibility
of a national registered provider protocol needs to be explored and whether
adaptations in the council stock should be brought under the DFG umbrella.
262

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
The Review Team
BRE conducted the previous review of the DFG means test and allocation formula
and manages the English Housing Survey. Helen Garrett and Maggie Davidson
provided the expertise to re-evaluate the allocation formula and provide options for
new mechanisms to distribute DFG resources. They also contributed to other parts
of the review, including the section on Common Parts and the Equality Act.
Ferret Information Systems provides software for the DFG means test, trains staff
in its operation and runs a helpline for practitioners. Gareth Morgan (CEO) carried
out the analysis and modelling of options for revising the means test and contributed
his expertise to other aspects of the review.
Foundations provides support to adaptation teams, home improvement agencies
and handyperson services. The organisation was given the brief in 2015 to improve
the operation of the DFG. They set up the DFG Champions service, deliver training,
run an information website, and provide the secretariat for the Memorandum of
Understanding for Improving Health and Care Through the Home. Paul Smith (CEO),
Francis Philippa (Strategy Lead) and the rest of the Foundations team played a key
role in the review. They carried out Freedom of information requests, conducted
consultation events, analysed the LOGASnet data and obtained much of the case
study material. Their depth of understanding of the operation of the DFG enabled
this review to be completed within a very tight time frame.
Rachel Russell is a practicing occupational therapist who has written widely about
assessment for home adaptations. She is also an occupational therapy lecturer and
manages the international genHOME database about adaptation outcomes. She
provided expert advice about the role of occupational therapists in the DFG process
and how services could be delivered more effectively.
Sheila Mackintosh, Research Fellow at the University of the West of England, has
carried out change management projects with local authority adaptation teams,
evaluated new services run by home improvement agencies, worked on local
adaptations agreements with housing associations, and done interviews and focus
groups with many people who have received the DFG. She produced a previous
report on the operation of the DFG in 2016 and various good practice reports. She
was also part of a team which did a recent review of the evidence of the impact and
outcomes of home adaptations. She was responsible for pulling together the
information provided by the rest of the team into this report.
263

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
List of organisations contributing to the review
We received a very high response to the consultation over the short period of time of
this review. There have also been many other people we have spoken to, or worked
with, over the last few years who have helped influence our thinking about the DFG.
Apologies to anyone who we have inadvertently left off the following list.
The 212 people who attended consultation workshops in Leeds, London and
Wolverhampton.
The 234 people/organisations who completed the online survey.
The 350+ members of the DFG Champions Facebook group.
All the local authorities who have responded to Foundations’ Freedom of Information
Requests over the last two years.
The Social Change Agency for facilitating “Rethinking DFG” workshops with support
from West of England Care & Repair, Millbrook Healthcare, Revival HIA, Shropshire
Council, London Borough of Tower Hamlets, Durham County Council and Bedford
Borough Council.
Foundations’ Commercial Partners: Abacus, AKW, Altro, Contour, Impey, NRS
Healthcare, ProCare, Promoting Independence, Safespaces, Solon Security, Stannah
and The OT Practice.
Foundations Advisory Board
Kate Curran from Worcestershire Care & Repair and Nina Warrington from Worcester
City Council.
All the Home Improvement Agencies who provided information on their costs and
income.
Ian Copeman, Marney Walker and Rachel Russell from the Housing LIN and RCOT
Jeremy Porteous from the Housing LIN
Additional case studies kindly provided by Care & Repair England / Centre for Ageing
Better.
Phillip Whitehead, originally at the University of Nottingham and now at Northumbria
University, for his work on the BATH-OUT study.
Luke Clements, Sorcha McCormack and students from CEREBRA, University of
Leeds, who provided information on children and young people’s DFG cases and the
accessibility of DFG application forms.
David Everatt and Tim McSharry, Access Committee for Leeds, initiated the research
on DFG’s for children and young people and contributed to the later study on
application forms.
264

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Vaila Morrison from the charity Inclusive Home for sharing her survey of families.
We received detailed written responses from:
The Local Government Association (LGA)
The Association of Directors of Adult Social Services (ADASS)
The County Councils Network (CCN)
The District Councils Network (DCN)
Councils in Dorset / Dorset Accessible Homes Service (DAHS)
North East Adaptations Group (NEAG)
We spoke to:
Angus Cleary of the Equalities and Human Rights Commission
Dave Anderson of the Social Care Institute for Excellence (SCIE)
Dawn Stobbs of NHS England
Dr Helen Meese of the Institution of Mechanical Engineers
Dr Lorraine Morley of Allia / Seas2Grow
Dr Richard Curry of the Smart Homes and Buildings Association (SH&BA)
Ed Warner of Motionspot
Gerry Hodgson of Cascade3D
Gursh Lail of Intel 4 Housing
Jane Lord of NHS England
Jane Mold and Sarah Jane Sharman of Rutland Council
Jim Ellam and Juliet Williams of Staffordshire County Council
John Shermer and Toby Shermer of LightwaveRF
Julia Skelton and Paul Cooper of the Royal College of Occupational Therapists
Karen Sawyer of Cornwall Council
Katherine Stevenson of Arthritis Research UK
Lee Davies of Millbrook Healthcare
Neil Revely of ADASS
Paul Coopey of Warwickshire HEART
Quin Quiney of Blaby District Council
265

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Rachael Docking and Catherine Foot of the Centre for Ageing Better
Rachael Martin-Smith of the Motor Neurone Disease Association (MNDA)
Rachel Shimmin of Buckinghamshire County Council
Robert Thompson of Care & Repair Scotland
Sarah Davis of the Chartered Institute of Housing
Sarah Hillcoat-Nallétamby of Swansea University
Sue Adams and Martin Hodges of Care & Repair England
Vicky Whittle and Madeleine Bell of the Chartered Institute of Environmental Health
Will Prochaska of Baxendales
266

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Appendix
267

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Appendix 1 - Proposed DFG Metrics
These will need further development
Inputs:
Person: Age, Gender, Impairment (by category)
Property: Tenure, Type (by category)
Outputs:
Grant Approvals (categorised by level of contribution)
Drop Outs (categorised by reason)
Timescales (calendar days for main stages)
Types of Adaptation (by category)
Grant Amount (by category)
Outcomes
TBC
Programme
Use of RRO Powers (by category)
Programme Budget
Programme Design (elements included)
268

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Appendix 2 Allocation formula
A2.1 Income Deprivation Domain
The Income Deprivation Domain measures the proportion of the population in an area
experiencing deprivation relating to low income. The definition of low income used
includes both those people that are out-of-work, and those that are in work but who
have low earnings (and who satisfy the respective means tests). It is calculated using
the following six non-overlapping indicators;
Adults and children in Income Support families
Adults and children in income-based Jobseeker’s Allowance families
Adults and children in income-based Employment and Support Allowance
families
Adults and children in Pension Credit (Guarantee) families
Adults and children in Working Tax Credit and Child Tax Credit families not
already counted, that is those who are not in receipt of Income Support,
income-based Jobseeker’s Allowance, income-based Employment and
Support Allowance or Pension Credit (Guarantee) and whose equivalised
income (excluding housing benefit) is below 60 per cent of the median before
housing costs
Asylum seekers in England in receipt of subsistence support, accommodation
support, or both.
Note: families=benefit units
269
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
A2.2 Other data sources investigated but not included in the allocations
formula modelling
1. Annual Population Survey. The number of working age disabled people by
disability type, economic activity (employed, unemployed and inactive) at a local
authority level for England and Wales 2015 to 2016 based on the (Table 2).
Selection of certain health issues would be required for a formula and therefore the
data is potentially less objective. Also incomplete covered for some regions and
local authorities.
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/disabilit
y/adhocs/006231thenumberofworkingagedisabledpeoplebydisabilitytypeeconomicact
ivityemployedunemployedandinactiveatalocalauthoritylevelforenglandandwales2015t
o2016basedontheannualpopulationsurvey
2. NHS - Children and Young People's Health Services Monthly Statistics, England -
August and September 2017, Experimental statistics.
https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-sets
The CYPHS is a patient-level dataset providing information relating to NHS-funded
community services for children and young people aged 18 years or under. The data
collected includes personal and demographic information, diagnoses including long-
term conditions and childhood disabilities and care events plus screening activities.
These statistics are classified as experimental and should be used with caution. More
information about experimental statistics can be found on the UK Statistics Authority
website.
3. Housing for Older People Supply – used data from Elderly Accommodation
Counsel – for data on older persons accommodation e.g. care – homes, residential
care, extra care housing and other data that were modelled.
4. HMRC. Data from HMRC’s personal income statistics which are updated annually
and based on a large (over 700,000 sample) of records on their PAYE, National
Insurance, Self-Assessment and Tax refunds databases. Unfortunately, the data
excludes those who don’t pay tax and National Insurance (i.e. the majority of
people on means tested benefits). As the methodology section notes:
However, as HMRC does not hold information for all people with personal incomes
below this level, the SPI is not a representative data source for this part of the
population and no attempt has been made to estimate the numbers of cases below
the tax threshold or the amount of their incomes. Therefore the National Statistics in
this and our earlier publication - with the exception of Tables 3.9 and 3.10 - only cover
individuals liable to UK income tax (taxpayers) and their incomes.
For this reason we would not recommend using this data as a reliable indicator of
income differentials between regions or authorities.
270
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Appendix 3 Means Testing
A3.1 Current rates of allowances and premiums
Table A3.1 shows the current rates of allowances and premiums used in the grant
scheme and those used for HB.
Current Disabled
Facilities Grant
Scheme
Housing Benefit
Personal Allowances
Single person - 65 or over
£143.80
£176.40
Single person - aged 60 to 64
£124.05
£163.00
232
Single person - 25 to 59
£60.50
£73.10
Single person - under 25
£47.95
£57.90
Single person - in receipt of main
phase ESA
£64.30
£73.10
Lone parent - 18 to 59
£60.50
Lone parent - under 18
£47.95
£57.90
Couple - elder aged 65 or over
£215.50
£263.80
Couple - elder aged 60 to 64
£189.35
£248.00
9
Couple - one or both aged 18 to 59
£94.95
£114.85
Couple - both under 18
£72.35
£87.50
Dependent children or young people
£52.59
£66.90
Premiums
Family Premium
233
Couple
£16.75
£17.45
Lone parent
£22.20
£22.20
Baby-under-one addition
£10.50
-
Disability Premium
Single person
£25.85
£33.55
Couple
£36.85
£47.80
Enhanced Disability Premium
Single person
£12.60
£16.40
Disabled child
£19.60
£25.48
232
Over Qualifying Age for State Pension Credit
233
Only for pre-2016 claims
271
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
A3.2 Example scenarios - details
The scenarios are purely illustrative and do not represent real cases nor relate to any
representation of typical situations. They are chosen to demonstrate points of
interest in the comparison.
All figures in the scenarios are weekly and assume a continuity of circumstances.
Scenario 1
Single aged 55, disabled, receiving high rate DLA or PIP for care needs. No income other
than state benefits.
DFG
Current
DFG
Uprated
Social
Care
Personal allowances and
premiums
Adult allowances
£60.50
£73.10
£91.40
Child allowances
£0.00
£0.00
£0.00
Premiums
£88.80
£114.25
£60.05
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£210.60
£266.60
£151.45
Income
Earned Income
Net Earnings
Earnings
£0.00
£0.00
£0.00
disregard
£20.00
£20.00
Assessable earnings
£0.00
£0.00
£0.00
Net Unearned Income
£0.00
£0.00
£0.00
Benefits Income
Disability benefits
£0.00
£0.00
£153.80
Income - AA, PP, DLA
Tariff Income from
£0.00
£0.00
£85.60
Capital
£0.00
£0.00
£0.00
Total Resources
£0.00
£0.00
£239.40
Excess Income
£0.00
£0.00
£87.95
Passported?
Yes
Yes
Current banding for
contribution
Owner
£0.00
£0.00
£2,411.46
Tenant
£0.00
£0.00
£1,412.97
272

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Gilt rate linked
Gilt rate 1.5%
Owner - 10 year
£0.00
£0.00
£11,379.00
Tenant -5 year
£0.00
£0.00
£5,476.38
Notes: In this example the claimant would qualify for means tested benefits and therefore be
passported under the current DFG rules.
In the social care assessment, there is no equivalent to the housing allowance in the DFG
calculation. Instead, net housing costs, offset by any benefit for them, is taken into account.
Benefits received, in this case an Income Support entitlement has been assumed, is taken
into account as available income. The higher rate disability entitlement is also treated as
being available. The social care needs figure ensures that the equivalent of Income Support,
or Guarantee Pension Credit, plus 25% remains before any excess income is assumed. In
this example, because these incomes are taken into account, there is only an excess income
figure under the social care test.
The application of an assessment of Disability Related Expenditure (DRE) could reduce, or
eliminate, the level of excess income. DRE is intended to reflect the reality of disability that
are additional to those normally required. In practice, it is discretionary in application,
practice varies from local authority to local authority and may vary greatly between
individuals. It is often criticised as a postcode lottery.
273
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 2
Couple eldest aged 55, one disabled, receiving high rate DLA or PIP for care needs. No
income other than state benefits.
DFG
Current
DFG
Uprated
Social Care
Personal allowances and
premiums
Adult allowances
£94.95
£114.85
£71.80
Child allowances
£0.00
£0.00
£0.00
Premiums
£55.00
£71.35
£28.75
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£211.25
£265.45
£100.55
Income
Earned Income
Net Earnings
Earnings
£0.00
£0.00
£0.00
disregard
£20.00
£20.00
Assessable earnings
£0.00
£0.00
£0.00
Net Unearned Income
£0.00
£0.00
£0.00
Benefits Income
Disability benefits Income -
£0.00
£0.00
£69.20
AA, PP, DLA
£0.00
£0.00
£85.60
Tariff Income from Capital
£0.00
£0.00
£0.00
Total Resources
£0.00
£0.00
£154.80
Excess Income
£0.00
£0.00
£54.25
Passported?
Yes
Yes
Current banding for
contribution
Owner
£0.00
£0.00
£1,141.30
Tenant
£0.00
£0.00
£668.54
Gilt rate linked
Gilt rate
1.5%
Owner - 10 year
£0.00
£0.00
£7,018.88
Tenant -5 year
£0.00
£0.00
£3,377.98
Notes: The social care means test is applied only to the individual client. In the case of
couples, the personal allowance in the assessment is reduced to half of the equivalent
benefits allowance (+25%). Joint income, including means tested benefits, is similarly
proportioned. Again, in this scenario, only under the social care means test would a
contribution be payable.
274
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 3
Single aged 75, disabled, receiving high rate DLA or PIP for care needs. Full Basic State
Pension of £125.95 a week plus £200 net private pension a week.
DFG
Current
DFG
Uprated
Social
Care
Personal allowances and
premiums
Adult allowances
£143.80
£176.40
£189.00
Child allowances
£0.00
£0.00
£0.00
Premiums
£50.35
£64.30
£60.05
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£255.45
£319.95
£249.05
Income
Earned Income
Net Earnings
Earnings
£0.00
£0.00
£0.00
disregard
£20.00
£20.00
Assessable earnings
£0.00
£0.00
£0.00
Net Unearned Income
£325.95
£325.95
£325.95
Benefits Income
Disability benefits Income -
£0.00
£0.00
£0.00
AA, PP, DLA
£0.00
£0.00
£85.60
Tariff Income from Capital
£0.00
£0.00
£0.00
Total Resources
£325.95
£325.95
£411.55
Excess Income
£70.50
£6.00
£162.50
Passported?
Yes
Yes
Current banding for
contribution
Owner
£1,753.77
£113.10
£12,752.38
Tenant
£1,027.50
£66.24
£7,472.03
Gilt rate linked
Owner - 10 year
Tenant -5 year
Gilt rate 1.5%
£9,121.31
£4,389.82
£776.28
£373.60
£21,024.30
£10,118.38
Notes: Even though an excess income figure has been calculated in the existing and
uprated DFG assessments, they are still passported by a small amount of housing benefit
which has been calculated. The social care assessment, although leaving 25% over the
Guarantee Pension Credit needs figure, still produces a substantially larger amount of
excess income, and their contribution, than the other assessments.
275
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 4
Couple both aged 75, one disabled, receiving high rate AA for care needs. Full Basic State
Pension of £125.95 a week each plus £300 net private pension a week.
DFG
Current
DFG
Uprated
Social
Care
Personal allowances and
premiums
Adult allowances
£215.50
£263.80
£144.30
Child allowances
£0.00
£0.00
£0.00
Premiums
£0.00
£0.00
£28.75
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£276.80
£343.05
£173.05
Income
Earned Income
Net
Earnings
Earnings
£0.00
£0.00
£0.00
disregard
£10.00
£10.00
Assessable earnings
£0.00
£0.00
£0.00
Net Unearned Income
£551.90
£551.90
£275.95
Benefits Income
Disability benefits Income -
£0.00
£0.00
£0.00
AA, PP, DLA
£0.00
£0.00
£85.60
Tariff Income from Capital
£0.00
£0.00
£0.00
Total Resources
£551.90
£551.90
£361.55
Excess Income
£275.10
£208.85
£188.50
Passported?
No
No
Current banding for
contribution
Owner
£48,568.21
£23,596.59
£16,672.40
Tenant
£28,458.03
£13,826.05
£9,768.87
Gilt rate linked
Gilt rate
1.5%
Owner - 10 year
£35,592.53
£27,021.08
£24,388.19
Tenant -5 year
£17,129.63
£13,004.45
£11,737.32
Notes: The increase in income, coupled with the loss of premiums applicable to a single
claimant, has removed entitlement to means tested benefits and therefore to passporting. In
this scenario, contributions are more equal as the social care assessment is only taking half
of the real income into account for the individual.
276
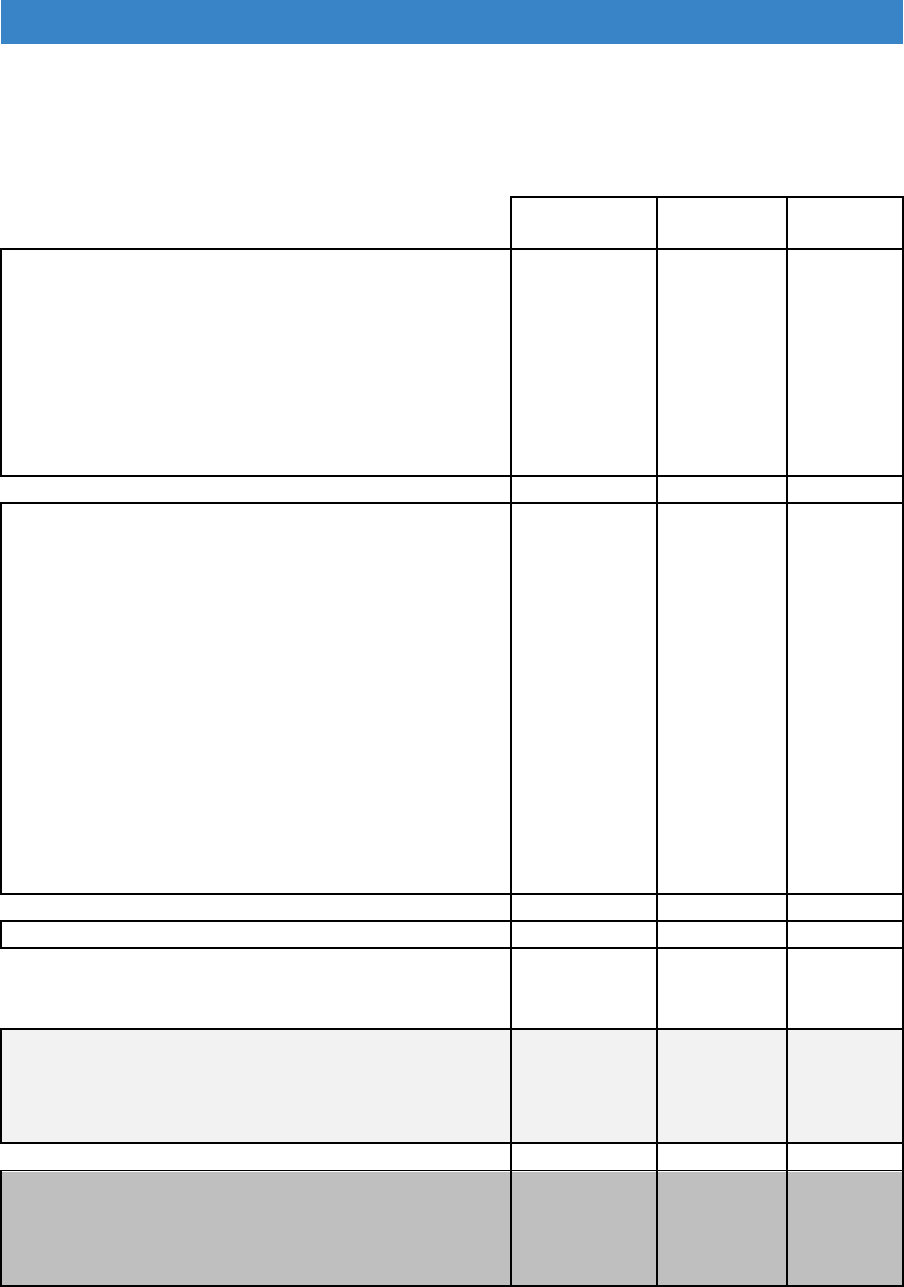
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 5
Couple both aged 55, three children aged under 16, one partner disabled, receiving high
rate DLA or PIP for care needs. Other partner working full-time and earning £400 net a
week.
DFG
Current
DFG
Uprated
Social
Care
Personal allowances and
premiums
Adult allowances
£94.95
£114.85
£71.80
Child allowances
£157.77
£200.70
£250.95
Premiums
£71.75
£88.80
£28.75
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£385.77
£483.60
£351.50
Income
Earned Income
Net Earnings
Earnings
£450.00
£450.00
£0.00
disregard
£20.00
£20.00
Assessable earnings
£430.00
£430.00
£0.00
Net Unearned Income
£0.00
£0.00
£0.00
Benefits Income
Disability benefits Income -
£48.10
£48.10
£0.00
AA, PP, DLA
£0.00
£0.00
£85.60
Tariff Income from Capital
£0.00
£0.00
£0.00
Total Resources
£478.10
£478.10
£85.60
Excess Income
£92.33
£0.00
£0.00
Passported?
No
No
Current banding for
contribution
Owner
£2,576.54
£0.00
£0.00
Tenant
£1,509.72
£0.00
£0.00
Gilt rate linked
Gilt rate
1.5%
Owner - 10 year
£11,945.69
£0.00
£0.00
Tenant -5 year
£5,749.11
£0.00
£0.00
Notes: in this scenario, there is no passported entitlement as, although Child Tax Credit is
payable, the earnings figure is above the £15,050 annual threshold. Child Tax Credit and
Child Benefit are disregarded for social care charging. The complete disregard of earnings
and the limit of assessment to the client alone, in the social care assessment, produces a
much lower resources figure in this scenario than for the other examples.
277
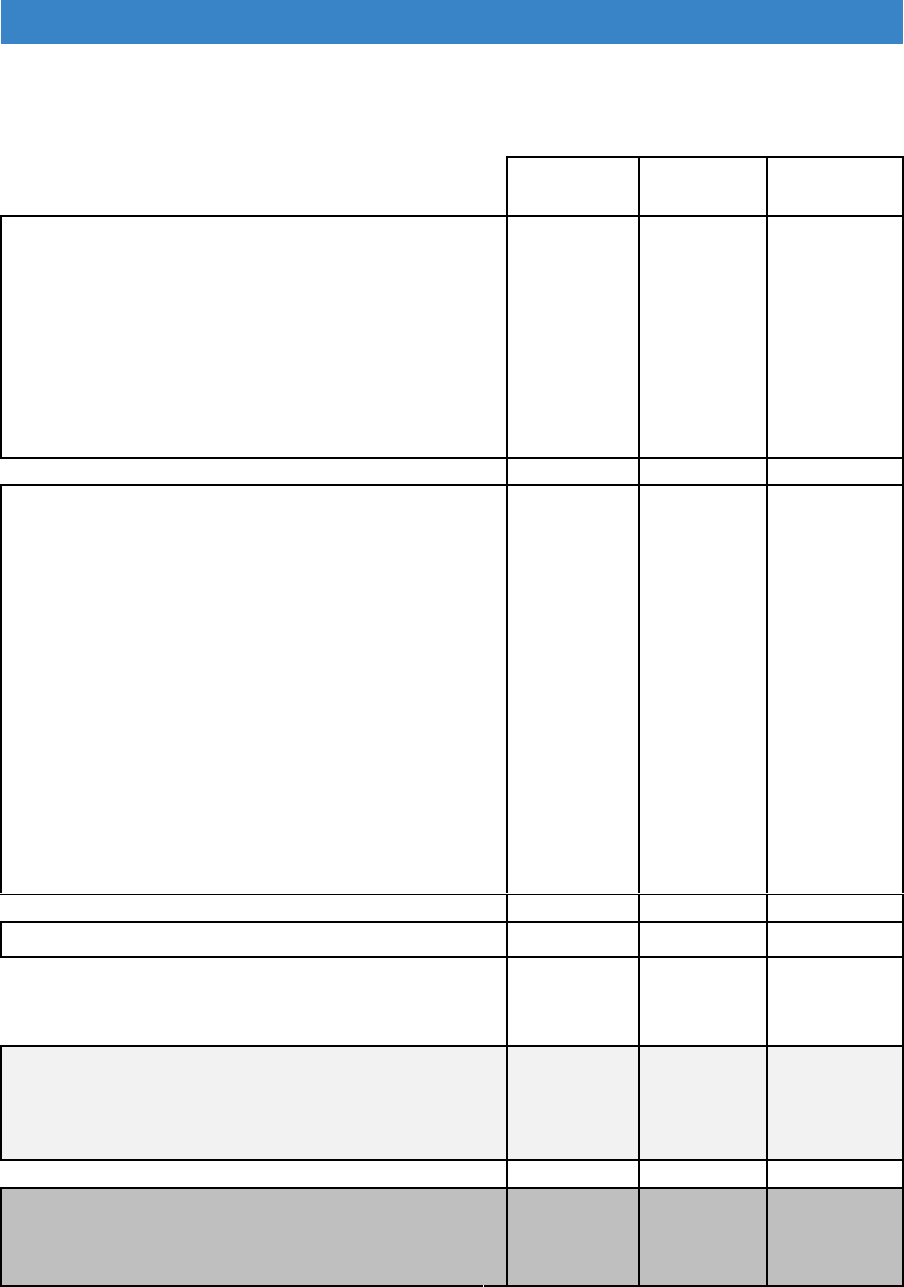
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Scenario 6 - Capital
A) Single aged 55, severely disabled, receiving high rate DLA or PIP for care needs. (as
scenario 1). Capital £10,000
DFG
Current
DFG
Uprated
Social
Care
Personal allowances and
premiums
Adult allowances
£60.50
£73.10
£91.40
Child allowances
£0.00
£0.00
£0.00
Premiums
£88.80
£114.25
£60.05
Housing Allowance
£61.30
£79.25
£0.00
Total Needs
£210.60
£266.60
£151.45
Income
Earned Income
Net Earnings
£0.00
£0.00
£0.00
Earnings
disregard
£20.00
£20.00
Assessable earnings
£0.00
£0.00
£0.00
Net Unearned Income
£0.00
£0.00
£0.00
Benefits Income
£0.00
£0.00
£137.80
Disability benefits Income -
AA, PP, DLA
£0.00
£0.00
£85.60
Tariff Income from Capital
£16.00
£16.00
£0.00
Total Resources
£16.00
£16.00
£223.40
Excess Income
£0.00
£0.00
£71.95
Passported?
Yes
Yes
Capital Barred?
No
No
No
Current banding for
contribution
Owner
£0.00
£0.00
£1,808.42
Tenant
£0.00
£0.00
£1,059.53
Gilt rate linked
Gilt rate 1.5%
Owner - 10 year
£0.00
£0.00
£9,308.91
Tenant -5 year
£0.00
£0.00
£4,480.11
278
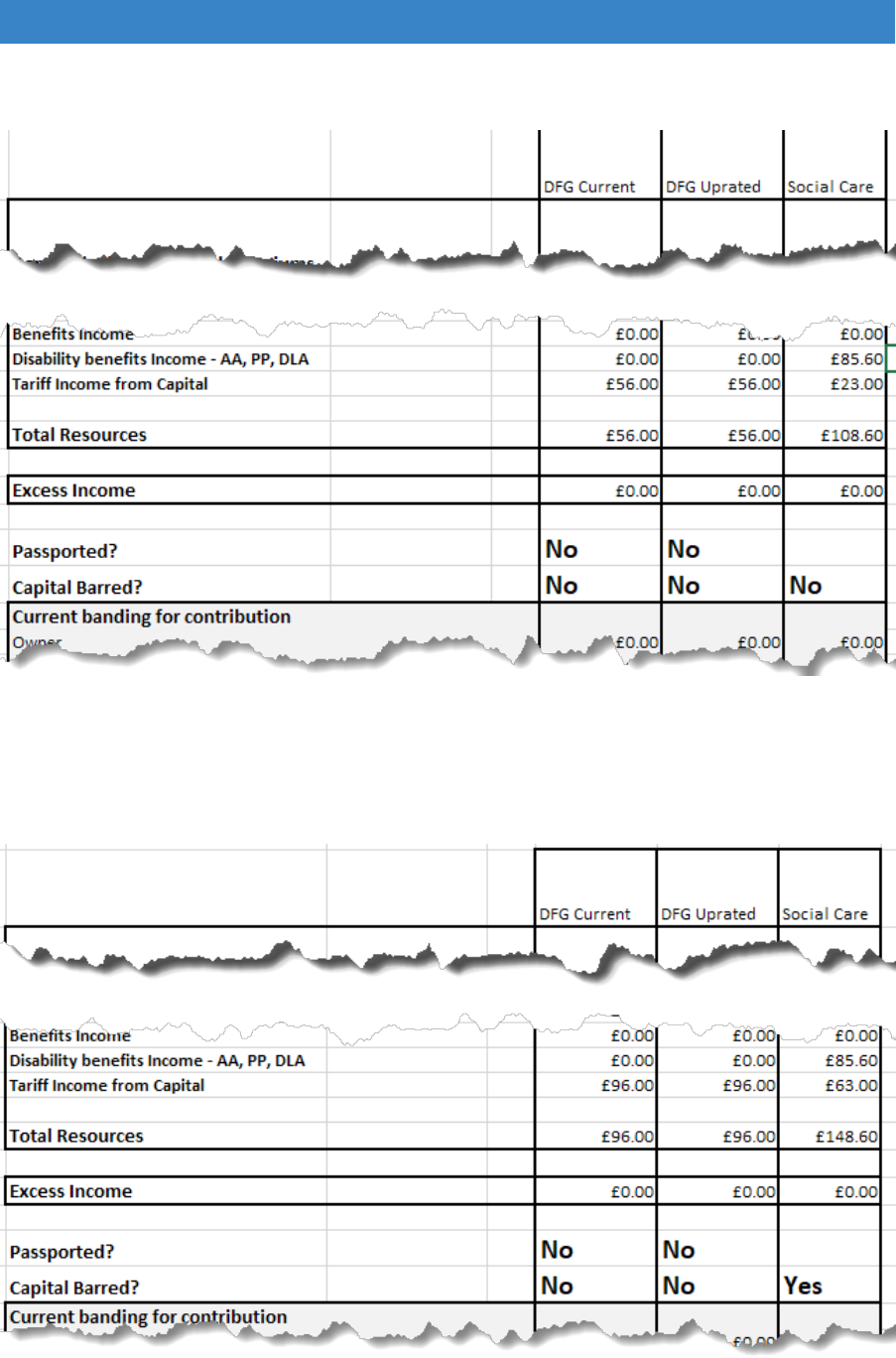
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
B) Single aged 55, severely disabled, receiving high rate DLA or PIP for care
needs. (as scenario 1). Capital £20,000
C) Single aged 55, severely disabled, receiving high rate DLA or PIP for care
needs. (as scenario 1). Capital £30,000
279
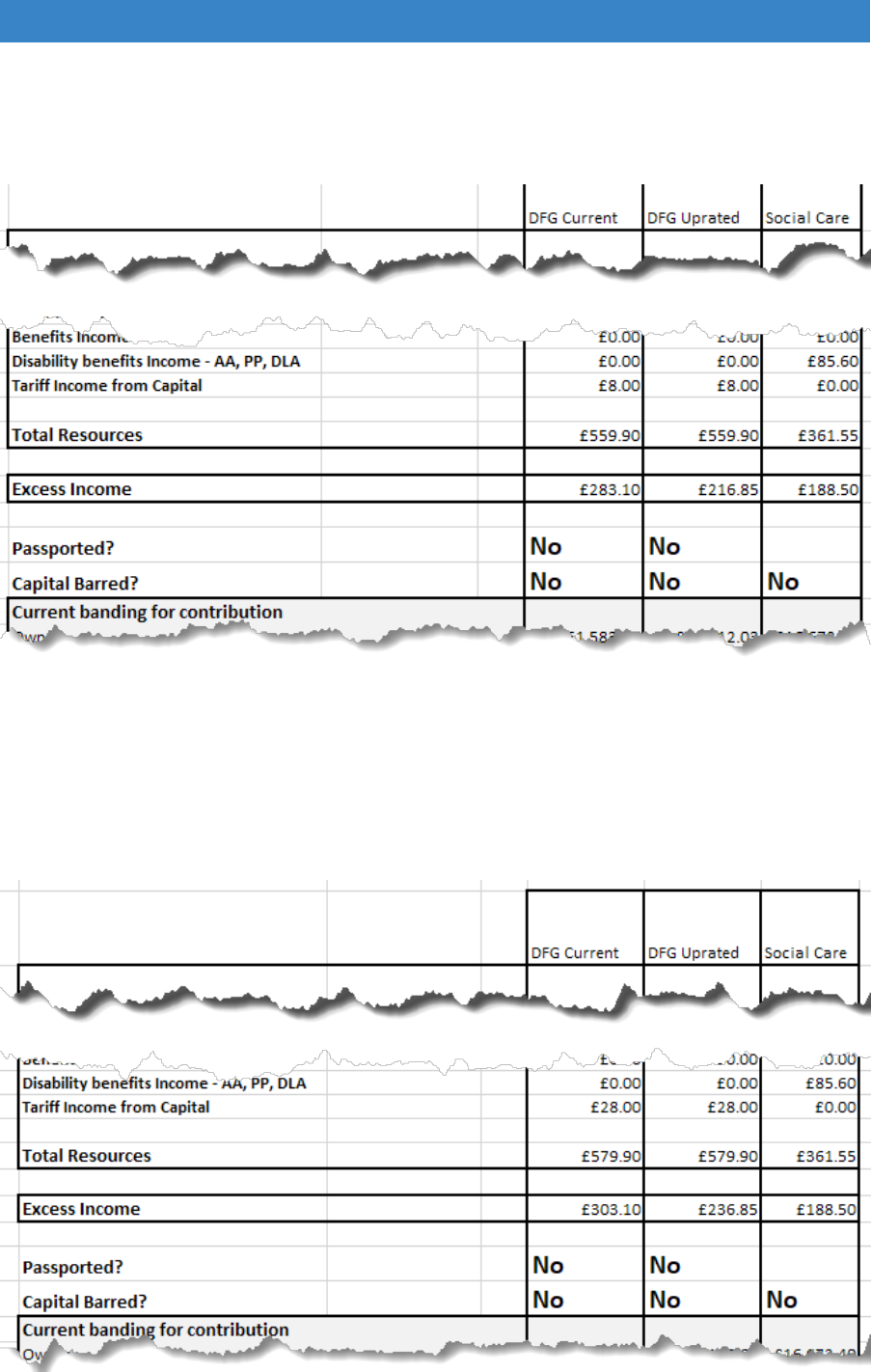
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
D) Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week. (as scenario 4). Capital £10,000
E) Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week. (as scenario 4). Capital £20,000
280

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
F) Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week. (as scenario 4). Capital £30,000
G) Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week. (as scenario 4). Capital £40,000
281
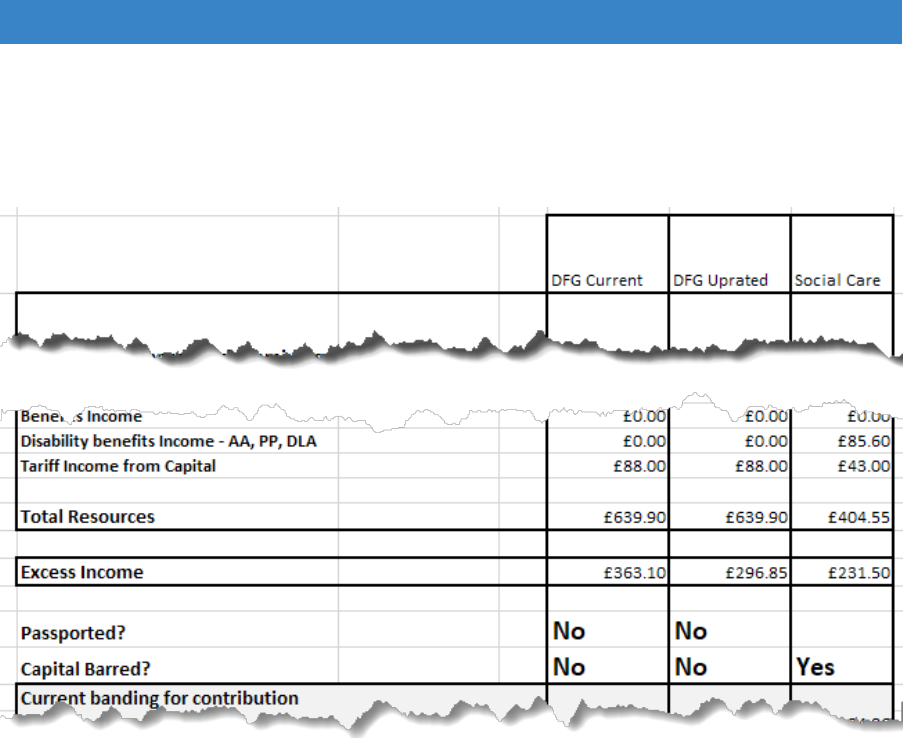
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
H) Couple both aged 75, one disabled, receiving high rate AA for care needs.
Full Basic State Pension of £125.95 a week each plus £300 net private
pension a week. (as scenario 4). Capital £50,000
Notes: Couple capital is shared for social care unless specifically attributable.
282
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
A3.3 Summary of main differences between the two preferred options
Items
Current DFG Test
Social Care
Qualification for
application
Different tests for residential
and domiciliary care
Applicant need not be part
of household
Yes
No
Older people
Start at 60
Womens state pension age
for older person.
Assessment period
previous 52 weeks
Later recovery
Various circumstances
Deprivation
Important issue
Needs
Children included
Yes
Yes
Additional amount included
for disability benefits
received
Severe Disability Premium,
Enhanced Disability
Premium, Disability
Premium
Enhanced Disability
Premium, Disability
Premium
Carer's premium
Yes
Yes
Housing costs
Fixed allowance
Housing cost disregard
Capital cut off and tariff
income
No cut-off, Tariff income
above £6,000 or £10,000 for
> 60
£23,250 cut-off. Tariff
income above £14,250
Resources
Disability benefits
Disregarded
Only Mobility disregarded.
Care amounts included in
income.
Notional contribution from
non-dependants
Yes
No
Income from boarders and
sub-tenants
Yes
No
Earnings net after tax & NI
Yes
Earnings completely
disregarded
Pension contributions
disregard
50%
No
Earnings disregard
Partial, follows most MTBs
for different family
circumstances
Complete
Income from capital
Common rules
Common type of
assessment
War Pensions
£10 disregard
Full disregard, except CAA,
from 2017 to meet Armed
Forces Covenant
requirements
Only income of individual
used
No
Yes
Housing related costs
Fixed allowance in needs
assessment
Disregarded from income
283

–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Disability related
expenditure
DRE elements and scheme
is at discretion of individual
local authorities.
Pension paid to absent
partner
50% if at least 50% paid to
partner
Assessment
Passporting
By receipt of MTBs and tax
credits
None
Difference between owners
& tenants
Yes
No
Leave a minimum amount of
income after assessment.
Only excess income used
Residential care PEA of
£24.90. MIG for non-
residential care calculated
similarly to MTBs. Includes
partner amounts.
Loan calculation
4 bands
Deferred payments possible
Family type
Disabled person and family
Disabled individual only
Changes of circumstance
Relevant date
circumstances
Weekly
284
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
References
Adams, L., Morris, S., Thomson, D., Rossiter, H., Felton, J., Newbold P. and Hazel, Z. (May 2018)
Housing and disabled people: the role of local authorities, London: EHRC.
https://www.equalityhumanrights.com/sites/default/files/research-report-115-housing-and-disabled-
people-the-role-of-local-authorities.pdf.
Adams, S. (2016) Reducing Delayed Transfer of Care through housing interventions: Evidence of
Impact. http://careandrepair-england.org.uk/wp-content/uploads/2014/12/WE-C-R-Case-Study-
Final.pdf.
Adams, S. (Mar 2017) Integration in Action: Evaluation of Age UK Warwickshire’s provision of
impartial information and advice about housing, care and related finance in later life.
http://careandrepair-england.org.uk/wp-content/uploads/2017/05/AgeUk-W-Evaluation-report-
Final.pdf.
Adams, S. and Hodges, M. (2018) Adapting for ageing: Good practice and innovation in home
adaptations, London: Centre for Ageing Better. https://www.ageing-
better.org.uk/sites/default/files/2018-10/Adapting-for-ageing-report_CfAB_0.pdf.
Age UK (Oct 2016) Hidden in plain sight: The unmet mental health needs of older people, London:
Age UK.
https://www.ageuk.org.uk/brandpartnerglobal/wiganboroughvpp/hidden_in_plain_sight_older_peoples
_mental_health.pdf.
Ainsworth, E., & de Jonge, D. (2019) Minor modifications: It’s not as simple as “Do It Yourself” (DIY).
To be published in E. Ainsworth & D. de Jonge (Eds.) An occupational therapist’s guide to home
modification practice (pp. 381-388). Thorofare, NJ: SLACK Inc.
Alzheimer’s Society (2012) Home Truth. Housing Services and support for people with dementia,
London: Alzheimer’s Society.
Alzheimer’s Society (2016) Fix Dementia Care: Homecare, London: Alzheimer’s Society.
Andrews, J. and Molyneux, P. (2013) Dementia: Finding housing solutions, London: National Housing
Federation. https://www.housing.org.uk/resource-library/browse/dementia-finding-housing-solutions/.
Astral Advisory (2013) Disabled Facilities Grants in England: a research report, London: The District
Councils’ Network (DCN) and the Society of District Council Treasurers (SDTC).
Bailey, C., Hodgson, P., Aitken, D. and Wilson G. (July 2018) Primary research with practitioners and
people with lived experience – to understand the role of home adaptations in improving later life.
https://www.ageing-better.org.uk/sites/default/files/2018-07/Primary-research-with-practitioners.pdf.
Bécaresyet, L. (2013) Dynamics of Diversity: Evidence from the 2011 Census, Manchester: Centre on
Dynamics of Ethnicity
Beresford, B. and Rhodes, D. (2008) Housing and disabled children, York: Joseph Rowntree
Foundation.
Buck, D., Simpson M. and Ross S. (2016) The economics of housing and health: The role of housing
associations, London: Kings Fund.
https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Economics_housing_and_he
alth_Kings_Fund_Sep_2016.pdf.
Building Research Establishment (2011) Disabled Facilities Grant allocation methodology and means
test: final report, London: DCLG.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/63
35/1850571.pdf.
285
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Building Research Establishment (2017) Client Report: Cost benefit analysis of home adaptations
[online] https://www.ageing-better.org.uk/sites/default/files/2017-
12/Appendices%2C%20the%20role%20of%20home%20adaptations%20in%20improving%20later%2
0life.pdf.
Care & Repair England (2016) Making the Housing Connections: An interim evaluation of the
Silverlinks Programme. https://silverlinksprogramme.files.wordpress.com/2017/01/silverlinks-interim-
report-1.pdf.
Centre for Ageing Better (July 2018) Homes that help: A personal and professional perspective on
home adaptations. https://www.ageing-better.org.uk/sites/default/files/2018-07/Homes-that-help-
research.pdf.
Chiatti, C. and Iwarsson, S. (2016) Evaluation of housing adaptation interventions: integrating the
economic perspective into occupational therapy practice, Scandinavian Journal of Occupational
Therapy, 21:5. 323-333, https://doi.org/10.3109/11038128.2014.900109.
Clements, L. and McCormack, S. (2017) Disabled Children and the Cost Effectiveness of Home
Adaptations & Disabled Facilities Grants: A Small-Scale Pilot Study, Leeds: Cerebra, University of
Leeds. http://www.cerebra.org.uk/research/university-of-leeds-cerebra-legal-entitlements-and-
problem-solving-project/student-research-projects/.
Clements, L. and McCormack, S. (July 2018) The accessibility of Disabled Facilities Grant application
forms in England. Leeds: University of Leeds, Access Committee for Leeds.
Communities and local Government Committee (Feb 2018) Housing for older people: Second report
of session 2017-19, London: House of Commons.
https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/370/370.pdf.
Connors, C., Kenrick, M. and Bloch, A. (2013) Rural Ageing Research: Summary Report of Findings,
London: DEFRA.
Construction Task Force (1998) Rethinking Construction, London: Dept of Trade and Industry.
http://constructingexcellence.org.uk/resources/rethinking-construction-the-egan-report/
Contact a Family (2011) Forgotten Families: The impact of isolation on families with disabled children
across the UK, London: Contact a Family.
Coughlin, J. F. (2015) How the Internet of Things & On-Demand Services Will Change Housing in
Retirement [online] http://bigthink.com/disruptive-demographics/how-the-internet-of-things-on-
demand-services-will-change-housing-in-retirement.
Coughlin, J. F. (2018) The Longevity Economy: Inside the World's Fastest-Growing, Most
Misunderstood Market by Joseph F. Coughlin, Cambridge, MA: Massachusetts Institute of
Technology.
Council of Mortgage Lenders (Dec 2016) The Profile of UK private landlords.
file:///C:/Users/white/Downloads/the-profile-of-uk-private-landlords-08.05.17%20(1).pdf.
Curtis, L. and Beecham, J. (2018) A Survey of Local Authorities and Home Improvement Agencies:
Identifying the hidden costs of providing a home adaptations service. https://kar.kent.ac.uk/66433/.
Dementia Services Development Centre (2013) Improving the design of housing to assist people with
dementia, Stirling: University of Stirling.
http://www.cih.org/resources/PDF/Scotland%20general/Improving%20the%20design%20of%20housi
ng%20to%20assist%20people%20with%20dementia%20-%20FINAL.pdf.
Department for Communities and Local Government (2006) Delivering Housing Adaptations for
Disabled People: A Good Practice Guide. London: DCLG.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/78
21/138595.pdf.
286
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Department for Communities and Local Government (2008) Disabled Facilities Grant – The Package
of Changes to Modernise the Programme, London: DCLG.
http://www.communities.gov.uk/documents/housing/pdf/dfgpackagechange.
Department of Health (2012) Improving outcomes and supporting transparency. Part2: Summary
technical specifications of public health indicators. Available at:
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_1
32358.
Department of Health (Mar 2017) 2017-19 Integration and Better Care Fund Policy Framework
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/60
7754/Integration_and_BCF_policy_framework_2017-19.pdf.
Department of Health and Social Care and NHS England (April 2018) A consultation on extending
legal rights to have for personal health budgets and integrated personal budgets.
https://consultations.dh.gov.uk/commissioning-integration-and-transformation/extending-rights-to-
personalised-budgets/.
Department of Work and Pensions (Mar 2018) Family Resources Survey 2016/17, London: National
Statistics. https://www.gov.uk/government/statistics/family-resources-survey-financial-year-201617.
DePoy, E. and Gilson, S. (2010) Disability Design and Branding: Rethinking Disability within the 21st
Century, Disability Studies Quarterly, Vol 30, No. 2. DOI: http://dx.doi.org/10.18061/dsq.v30i2.1247.
Diraco, G., Leone, A., & Siciliano, P. (2017). A Radar-Based Smart Sensor for Unobtrusive Elderly
Monitoring in Ambient Assisted Living Applications. Biosensors, 7(4), 55.
https://doi.org/10.3390/bios7040055 .
Doughty, K. (2004) Supporting independence: the emerging role of technology, Housing, Care &
Support 7(1), pp11–17. https://doi.org/10.1108/14608790200400004.
Equalities and Human Rights Commission (2018) Housing and disabled people: Britain’s hidden
crisis. https://www.equalityhumanrights.com/sites/default/files/housing-and-disabled-people-britains-
hidden-crisis-main-report.pdf.
Equity Release Council (2018) Spring 2018 Market Report [online]
http://www.equityreleasecouncil.com/document-library/equity-release-market-report-spring-2018/.
Evans, S., (April 2018) Dementia Dwelling Grants – evaluation of the pilot programme. Interim
evaluation report, University of Worcester Association for Dementia Studies.
Ewart, I. J. and Harty, C. (2015) Provision of disability adaptations to the home: analysis of household
survey data. Housing Studies, 30 (6). pp. 901-924. ISSN 0267-3037
https://doi.org/10.1080/02673037.2014.991379.
Foundations (2016a) Linking Disabled Facilities Grants to Social Care Data.
http://foundationsweb.s3.amazonaws.com/4210/foundations-dfg-foi-report-nov-2015.pdf.
Foundations (2016b) Supporting people in private rented sector housing: A good practice guide,
Glossop: Foundations. http://www.foundations.uk.com/media/4441/prs-good-practice-guide.pdf.
Foundations (2016c) Preparing a policy under the Regulatory Reform Order (2002) Housing renewal.
www.foundations.uk.com/media/4696/preparing-a-policy-under-the-rro.pdf.
Gardiner C, Ryan T and Gott M. (2018) What is the cost of palliative care in the UK? A systematic
review BMJ Supportive & Palliative Care 8:250-257. http://dx.doi.org/10.1136/bmjspcare-2018-
001519.
Garrett, H. and Burris, S. (2016) Homes and ageing in England.
https://www.bre.co.uk/filelibrary/Briefing%20papers/86749-BRE_briefing-paper-PHE-England-A4-
v3.pdf.
287
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Greater London Authority (May 2018) London Housing Strategy, Section 5.39, p. 145.
https://www.london.gov.uk/sites/default/files/2018_lhs_london_housing_strategy.pdf.
Halsall, B. and MacDonald, R. (2015) Design for dementia – Vols 1 and 2.
http://www.hlpdesign.com/images/case_studies/Vol1.pdf.
http://www.hlpdesign.com/images/case_studies/Vol2.pdf.
Heinbüchner, B., Hautzinger, M., Becker, C. et al. (2010) Satisfaction and use of personal emergency
response systems, Z Gerontol Geriat 43: 219. https://doi.org/10.1007/s00391-010-0127-4.
Heywood et al. (2005) Reviewing the Disabled Facilities Grant Programme, Bristol: School for Policy
Studies.
Heywood, F. (1994) Adaptations: finding ways to say yes, Bristol: SAUS Publications.
Heywood, F. (2001) Money well spent: the effectiveness and value of housing adaptations, Bristol:
The Policy Press.
Heywood, F. and Mackintosh, S. (2008) Housing Associations and Home Adaptations: Making it Work
Smoothly, London: Habinteg.
https://www.habinteg.org.uk/download.cfm?doc=docm93jijm4n432.pdf&ver=519.
Hilditch, M. (May 2018) Repairs and maintenance spend tracker: what did your association do in
2016/17? Inside Housing Insight. https://www.insidehousing.co.uk/insight/repairs-and-maintenance-
spend-tracker-what-did-your-association-do-in-201617-
56310?utm_source=Ocean%20Media%20Group&utm_medium=email&utm_campaign=9493587_IH-
THE-FRIDAY-LONG-READ-18-5-2018-GR&dm_i=1HH2,5NHAR,L7J0AM,LZEN1,1.
HM Government (Mar 2015) Working Together to safeguard children: A guide to inter-agency working
to promote the welfare of children, Chapter 3: Local Safeguarding Children Boards.
http://www.workingtogetheronline.co.uk/chapters/chapter_three.html.
HM Government (2017) UK Industrial Strategy: Building a Britain fit for the future [online]
https://www.gov.uk/government/publications/industrial-strategy-building-a-britain-fit-for-the-future.
HM Government (2018) Industry Strategy: Construction Industry Deal [online]
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/73
1871/construction-sector-deal-print-single.pdf.
HM Treasury (Nov 2015) Spending Review and Autumn Statement 2015, Adult Social Care, Section
1.109, p. 33. https://www.gov.uk/government/publications/spending-review-and-autumn-statement-
2015-documents.
Home Adaptations Consortium (2013) Home adaptations for disabled people: a detailed guide to
related legislation, guidance and good practice, Nottingham: Home Adaptations Consortium.
http://careandrepair-england.org.uk/wp-content/uploads/2014/12/DFG-Good-Practice-Guide-30th-
Sept-13.pdf.
Housing LIN (2018) Home from Hospital tool [online] https://www.housinglin.org.uk/home-from-
hospital/tool/.
Jeffs, M. (2018) Moving from outputs to outcomes [online]
https://goodpracticeexchange.wales/2018/05/15/moving-from-outputs-to-outcomes/.
Johnson, C. (2016) The Future of Connected Home Health, Saffron Waldon: Plextec.
https://www.plextek.com/wp-content/uploads/2016/07/The-future-of-connected-home-health.pdf
Kempton, O. and Warby, A. (2011) Measuring the Social Return on Investment of Stage 3
Adaptations and Very Sheltered Housing in Scotland. https://www.hanover.scot/wp-
content/uploads/2015/11/SROI-VSH-and-Adaptations-full-report-final-Sept-2011.pdf.
288
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Latham, M. (1994) Constructing the Team, London: HMSO.
http://constructingexcellence.org.uk/resources/constructing-the-team-the-latham-report/.
Leonard Cheshire (2015) The long wait for a home, London: Leonard Cheshire.
https://www.leonardcheshire.org/sites/default/files/Leonard-Cheshire-Disability-The-Long-Wait-for-a-
Home.pdf.
Local Government Association (2018) Housing Advisors Programme 2018/19.
https://www.local.gov.uk/topics/housing-and-planning/housing-advisers-programme-201819.
Local Government Ombudsman (2016) Making a house a home: Local authorities and disabled
adaptations. https://www.lgo.org.uk/information-centre/news/2016/mar/delays-to-disabled-facilities-
grant-process-have-major-impact-on-people-s-lives-says-ombudsman.
Mackintosh, S. and Collingbourne, L. (2015) Home Adaptations for Disabled People Good Practice
Case Study: Wigan. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-
wigan1.pdf.
Mackintosh, S. and Collingbourne, L. (2015) Home Adaptations for Disabled People Good Practice
Case Study: Sunderland, Home Adaptations Consortium.
https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-of-good-practice-sunderland-
care-support.pdf.
Mackintosh, S. and Collingbourne, L. (2016) Home Adaptations for Disabled People Good Practice
Case Study: Middlesbrough. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-
of-good-practice-middlesbrough-staying-put.pdf.
Mackintosh, S. and Collingbourne, L. (2016) Home Adaptations for Disabled People Good Practice
Case Study: Knowsley. https://homeadaptationsconsortium.files.wordpress.com/2013/10/cameo-of-
good-practice-knowsley-centre-for-independent-living.pdf.
Mackintosh, S. and Heywood, F. (2015) The Structural Neglect of Disabled Housing Association
Tenants in England: Politics, Economics and Discourse, Housing Studies, 30:5, 770-791.
https://doi.org/10.1080/02673037.2015.1044947.
Mackintosh, S. and Leather, P. (2016) The Disabled Facilities Grant Before and after the introduction
of the Better Care Fund, Glossop: Foundations, p. 36-37.
http://www.foundations.uk.com/media/4665/dfg-report-final-interactive-converted-draft-6-small.pdf
Marie Curie Cancer Care (2014) Understanding the cost of end of life care in different settings.
https://www.mariecurie.org.uk/globalassets/media/documents/commissioning-our-
services/publications/understanding-cost-end-life-care-different-settingspdf.
Marmot, M. (2015) The Health Gap, London: Bloomsbury.
MICRA (2017) The Golden Generation: Wellbeing and Inequalities in Later Life, Manchester:
University of Manchester Institute for Collaborative Research on Ageing.
http://hummedia.manchester.ac.uk/institutes/micra/reports/golden-generation-report-2017.pdf.
Ministry of Housing, Communities and Local Government (2016a) English housing survey 2014-2015:
Adaptations and accessibility of homes report, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-adaptations-and-
accessibility-of-homes-report.
Ministry of Housing, Communities and Local Government (2016b) English housing survey 2014-
2015: Housing for older people report, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-housing-for-older-
people-report.
Ministry of Housing, Communities and Local Government (2016c) English Housing Survey 2014-
2015: Private Rented Sector report, London: MHCLG.
289
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
https://www.gov.uk/government/statistics/english-housing-survey-2014-to-2015-private-rented-sector-
report.
Ministry of Housing, Communities and Local Government (2017a) English Housing Survey 2015-
2016: Potential for stock improvements, London: MHCLG.
https://www.gov.uk/government/statistics/english-housing-survey-2015-to-2016-potential-for-stock-
improvements.
Ministry of Housing, Communities and Local Government (2017b) English Housing Survey: Housing
costs and affordability, 2015-16, London: MHCLG. https://www.gov.uk/government/statistics/english-
housing-survey-2015-to-2016-housing-costs-and-affordability.
Ministry of Housing, Communities and Local Government (Mar 2018) English Housing survey:
Headline Report 2015/16, London: DCLG. https://www.gov.uk/government/statistics/english-housing-
survey-2015-to-2016-headline-report.
Money, A. et al (2015) Using the Technology Acceptance Model to explore community dwelling older
adults’ perceptions of a 3D interior design application to facilitate pre-discharge home adaptations,
BMC Medical Informantics and Decision Making, 15:73. https://doi.org/10.1186/s12911-015-0190-2.
Moran, A. (Jul 2017) The Lightbulb Project: Switched on to integration in Leicestershire, London:
Housing LIN.
https://www.housinglin.org.uk/_assets/Resources/Housing/Practice_examples/Housing_LIN_case_stu
dies/HLIN_CaseStudy_135_Lightbulb_Project.pdf.
National Audit Office (2017) Health and social care integration. https://www.nao.org.uk/report/health-
and-social-care-integration/.
National Audit Office (Mar 2018) Reducing emergency admissions. https://www.nao.org.uk/wp-
content/uploads/2018/02/Reducing-emergency-admissions.pdf.
National Housing Federation (2016) Can our homes pay for the care we need in older age? Asset
wealth and an ageing population. http://s3-eu-west-
1.amazonaws.com/pub.housing.org.uk/Can_our_homes_pay_for_the_care_we_need_in_older_age_-
_asset_wealth_and_an_ageing_population_PDF_for_web.pdf.
NHS England (2016) The variation between standard and optimal pathways - Janet’s story: Frailty,
RightCare scenario. https://www.england.nhs.uk/rightcare/wp-content/uploads/sites/40/2016/08/janet-
story-narr.pdf.
NHS England (2017) Integration and Better Care Fund planning requirements for 2017-19.
https://www.england.nhs.uk/wp-content/uploads/2017/07/integration-better-care-fund-planning-
requirements.pdf.
NHS England (Aug 2017) The Better Care Fund Planning Requirements 2017-19: Frequently Asked
Questions, p. 9. https://www.england.nhs.uk/wp-content/uploads/2017/08/bcf-planning-requirements-
faqs.pdf.
Northern Ireland Housing Executive (2018) Adaptations Design Communications Toolkit [online]
https://www.nihe.gov.uk/adaptations_design_communications_toolkit.pdf.
Papworth Trust (2012) Home solutions to our care crisis, Cambridge: Papworth Trust.
https://www.housinglin.org.uk/_assets/Resources/Housing/OtherOrganisation/homesolutionstoourcar
ecrisis.pdf.
Parker, I. and Isaksen, M. (2017) A state of disrepair: Why renters deserve a better deal.
https://www.citizensadvice.org.uk/Global/CitizensAdvice/Housing%20Publications/PRS-
AStateofDisrepair.pdf.
290
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Pension and Lifetime Savings Association (2017) Decumulation Decisions: Pension Freedom
Journeys. https://www.plsa.co.uk/Policy-and-Research/Document-library/Decumulation-decisions-
pension-freedoms-journeys.
Phillips, C., Keller, J., Popescu, M., Skubic, M., Rantz, M., Cuddihy, P. and Yardibi, T. (2012). Radar
walk detection in the apartments of elderly. Conference proceedings of Annual International
Conference of the IEEE Engineering in Medicine and Biology Society.
https://doi.org/10.1109/EMBC.2012.6347327.
Porteus, J. (2018) Rural Housing for an Ageing Population: Preserving Independence, The Rural
HAPPI Inquiry, HAPPI 4.https://www.housinglin.org.uk/Topics/type/Rural-Housing-for-an-Ageing-
Population-Preserving-Independence-HAPPI-4/.
Powell, J., Mackintosh, S., Bird, E., Ige, J., Garrett, H. and Roys, M. (Nov 2017) The role of home
adaptations in improving later life, London: Centre for Ageing Better. https://16881-presscdn-0-15-
pagely.netdna-ssl.com/wp-content/uploads/2017/11/The-role-of-home-adaptations-in-improving-later-
life.pdf.
Public Health England (2016) Evaluation of the impact of Fire and Rescue Service interventions in
reducing the risk of harm to vulnerable groups of people from winter-related illnesses.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/57
3558/FRS_winter_pressures_evaluation.pdf.
Public Health England (Feb 2018) A return on investment tool for the assessment of falls prevention
programmes for older people living in the community.
https://www.gov.uk/government/publications/falls-prevention-cost-effective-commissioning.
RIBA (2013) Plan of Work [online] https://www.ribaplanofwork.com/.
Royal College of Occupational Therapists (2006) Minor Adaptations without Delay [online]
https://www.rcot.co.uk/practice-resources/rcot-publications/downloads/minor-adaptations-without-
delay.
Royal College of Occupational Therapists and Foundations (2015). DFG Summit. [online]
https://www.rcot.co.uk/file/1550/download?token=UJrn-qHx.
Royal Collage of Occupational Therapists (2016) Care Act 2014: Guidance for Occupational
Therapists, The Disabled Facilities Grant, London: RCOT. https://www.rcot.co.uk/practice-
resources/rcot-publications/downloads/care-act-2014-dfg.
Royal College of Occupational Therapists (In Press) Adaptations without delay: a guide to thinking
about and delivering adaptations differently. London: Royal College of Occupational Therapists.
Royal College of Physicians (2011), NHS services for falls and fractures in older people are
inadequate, finds national clinical audit. Available at: https://www.rcplondon.ac.uk/news/nhs-services-
falls-and-fractures-older-people-are-inadequate-finds-national-clinical-audit.
Rugg, J. and Croucher, K (2010) Older People’s Experiences of Renting Privately, London: Age
Concern and Help the Aged.
Russell, R., Ormerod, M. and Newton, R., (2018) The development of a design and construction
process protocol to support the home modification process delivered by occupational therapists.
Journal of aging research. https://doi.org/10.1155/2018/4904379.
Scottish Government (2017) Evaluation of Adapting for Change, Edinburgh: Scottish Government.
http://www.gov.scot/Resource/0052/00524668.pdf.
Seas 2 Grow (2017) Silver Economy Accelerating Strategies: Market Study.
https://www.seas2grow.com/wp-content/uploads/2017/06/SEAS-2-Grow-Market-Study-EN.pdf.
Silk Road (Jan 2018) Considerations when moving to a retirement style home [online]
http://www.wearesilkroad.com/pages/news/older_people.php?v3.
291
–Disabled Facilities Grant (DFG) and Other Adaptations Main Report
Snell, T. Fernandez, J. Forder, J. (2012) Building a business case for investing in adaptive
technologies in England, Personal Social Services Research Unit, Discussion Paper 2831, London:
School of Economics and Political Science.
Statutory guidance, Care Act 2014: supporting implementation [online].
https://www.gov.uk/government/publications/care-act-statutory-guidance.
Sum S, Mathews RM, Hughes I, Campbell A. (2008) Internet Use and Loneliness in Older Adults,
Cyberpsychol Behav. Apr;11(2):208-11. https://doi.org/10.1089/cpb.2007.0010.
The Academy of Medical Sciences (Apr 2018) Multimorbidity: a priority for global health research,
London: The Academy of Medical Sciences. https://acmedsci.ac.uk/file-download/99630838.
Thirteen Group Annual Report 2016/17 (2017) [online]
https://www.thirteengroup.co.uk/uploaded/thirteen/files/Thirteen%20Financial%20Annual%20Report%
2016-17.pdf.
University of Stirling (2018) App to help improve environments for people living with dementia.
https://www.stir.ac.uk/news/2017/06/newapptohelpimproveenvironmentsforpeoplelivingwithdementia/.
Vibert, S. (2017) MND Costs: Exploring the Financial Impact of Motor Neurone Disease, London:
DEMOS. https://www.mndassociation.org/wp-content/uploads/DEMOS-FULL-report.pdf.
Wales Audit Office (2018) Housing Adaptations, Cardiff: Wales Audit Office.
http://www.audit.wales/publication/housing-adaptations.
Walker, M. (2016) Effective communication methods for Housing OTs http://ot-
magazine.co.uk/effective-communication-methods-for-housing-ots.
Wallace, A., Rhodes, D. and Roth, F. (Feb 2018) Home owners and poverty, York: JRF.
https://www.jrf.org.uk/report/home-owners-and-poverty.
Whitehead, P., Golding-Day, M., Belshaw, S., Dawson, T., James, M. and Walker, M. Bathing
adaptations in the homes of older adults (BATH-OUT): Results of a Feasibility Randomised Controlled
Trial (RCT) Manuscript submitted to BMC Public Health March 2018.
Whitehead, P., James, M., Belshaw, S., Dawson, T., Day, M. and Walker, M. (2016) Bathing
adaptations in the homes of older adults (BATH-OUT): Protocol for a Feasibility Randomised
Controlled Trial (RCT) BMJ Open. 6, e013448. http://dx.doi.org/10.1136/bmjopen-2016-013448.
Wilson, W. (1996) Housing renovation grants, House of Commons Library Research Paper 96/34
596/34. https://researchbriefings.parliament.uk/ResearchBriefing/Summary/RP96-34.
Wilson, W. and Fears, C. (Dec 2016) Disabled Facilities Grants for home adaptation, Briefing Paper
No. 03011, London: House of Commons Library.
http://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN03011.
Worcestershire Housing Partnership Plan 2017
http://moderngovwebpublic.redditchbc.gov.uk/documents/s27809/170322%20Final%20Worcestershir
e%20Housing%20Partnership%20Plan%2011d.pdf.
Zhou, W., Oyegoke, A.S. & Sun, (2017) Service planning and delivery outcomes of home adaptations
for ageing in the UK, M. J Hous and the Built Environ. https://doi.org/10.1007/s10901-017-9580-3.
292
